Orthognathic Surgery
Seminars in Oral Surgery
١
SURGICAL MANAGEMENT OF MAXILLOFACIAL DEFORMITIES
Malformations of the maxilla and the mandible, even when mild, can produce a wide
range of maxillofacial deformities which may be classified into 3 groups:
1) Congenital: may be unilateral or bilateral, e.g. those associated with Treacher-
Collins syndrome, hemifacial microsomia, and cleft palate and alveolus.
2) Developmental: causes: congenital anomalies of adjacent structures like
hemangioma; trauma like condylar fractures, infection like osteomyelitis, and
endocrine imbalance like acromegaly.
3) Acquired: e.g. malunited facial fractures.
The resultant jaw deformities can either be skeletal or dento-alveolar.
I- SKELETAL JAW DEFORMITIES
Mandibular prognathism
Etiology: can be hereditary (Habsburgs family), due to trauma, or due o disease.
Classification: 4 patterns exist: prognathism with normal maxilla, prognathism with
underdeveloped maxilla (the commonest type), prognathism with anterior open bite,
and bimaxillary prognathism. Clinical features: acromegalic face, protruded chin and
lower lip, concave facial profile, CIII occlusion, and anterior cross bite. When severe,
eating and speech are affected. Cephalometric findings: ↑ SNB angle, and mandibular
plane angle is frequently reduced. Treatment: mandibular set back after bilateral
condylectomy, condylectomy with removal of bone from below the sigmoid notch,
horizontal and oblique blind ramus osteotomy (Kosteĉka), or inverted L osteotomy
(Trauner). However, the most commonly performed procedures nowadays are sagittal
split osteotomy and vertical ramus osteotomy.
Mandibular retrognathism (micrognathism)
Etiology: may be congenital, developmental (trauma at birth or early growth), or
acquired. Classification: unilateral or bilateral. Clinical features: short body of
mandible, short ramus, retruded chin, bird face appearance, CII occlusion (mostly
division 2), laterognathism and posterior cross bite (in unilateral cases), restricted
mouth opening (when TMJ ankylosis exists). Cephalometric findings: ↓ SNB angle, and
mandibular plane angle is often increased. Treatment: body elongation osteotomies
(rarely used because of many disadvantages), vertical ramus osteotomy (for mild cases),
and sagittal split osteotomy (most popular).
Mandibular laterognathism
A truly symmetric face does not exist. However, when the
mandible deviates to one side beyond the average, facial
asymmetry becomes clinically pronounced. Etiology: trauma to
condyle in early life, congenital (hemifacial microsomia),
unilateral condylar hyperplasia, or due to bone loss by surgery.
Treatment: early intervention to improve growth potential or to
restrict progressive growth may be necessary. A mandibular
osteotomy alone may not completely resolve the skeletal
asymmetry. Sagittal split + LeFort I osteotomy + genioplasty

Orthognathic Surgery
Seminars in Oral Surgery
٢
may be required to establish facial symmetry.
Chin deformities
Microgenia: small receding chin may be an isolated deformity, associated with
mandibular micrognathism, or even with mandibular prognathism. It may be hereditary
or due to severe trauma to the chin. In cephalogram, SN-Pogonion angle is reduced.
Treatment: chin augmentation by onlays, buccal inlays (extension of mandibular
prosthesis), sliding genioplasty, or mandibular body osteotomy (rarely used).
Macrogenia: large chin is strongly related to hereditary factors. It causes prognathic
(aggressive) appearance which may be acceptable in males but esthetically unpleasant
in females. Macrogenia may be isolated or associated with mandibular prognathism. In
cephalogram, SN-Pogonion angle is increased. Treatment: chin contouring by removing
excess bone, or horizontal chin recession by sliding genioplasty.
Maxillary prognathism
Maxillary prognathism (of the entire maxilla) is a rare condition. However, protrusion
in the anterior segment can be seen in patients with mandibular micrognathism. Severe
maxillary protrusion can also be found when associated hemangioma or fibrous
dysplasia exists. Excessive posterior maxillary width may produce unilateral or bilateral
cross bite. Treatment: maxillary advancement by LeFort I osteotomy.
Maxillary retrognathism (micrognathism)
Posterior positioning of entire maxilla can be seen in patients with malunited midfacial
fractures. Underdevelopment of skeletal maxilla is often seen in patients with cleft
palate or craniofacial synostosis (e.g. Crouzon's disease). Treatment: anterior
repositioning by LeFort I, II, or III osteotomies.
II- DENTO-ALVEOLAR JAW DEFORMITIES
Maxillary protrusion
Clinically: labial inclination of upper anterior teeth and convex profile in upper lip
region. Cephalometry: PNS-ANS measurement and SNA angle are increased.
Treatment: many cases can be treated by orthodontic therapy alone. When surgery is
required, anterior segmental osteotomy or LeFort I osteotomy are useful options.
Maxillary retrusion
Clinically: retruded upper anteriors with normal molar occlusion, and retruded
appearance of upper lip. Frequently associated with cleft palate deformity.
Cephalometry: PNS-ANS measurement and SNA angle may be reduced. Treatment:
maxillary advancement by anterior segmental osteotomy or LeFort I osteotomy.
Mandibular protrusion
Isolated mandibular protrusion is an uncommon deformity. Unlike prognathism, molar
occlusal relationships are satisfactory. Treatment: many cases can be treated by
orthodontic therapy alone. When surgery is required, set back can be achieved by
anterior segmental osteotomy.

Orthognathic Surgery
Seminars in Oral Surgery
٣
Bimaxillary protrusion
Clinically: thick incompetent lips. It is more common in Black and Oriental people than
in Whites. There is often an associated microgenia. Treatment: extraction of first or
second premolars + preoperative orthodontic therapy + anterior segmental osteotomies
(upper: Wassmund procedure, lower: Köle procedure). Genioplasty and rhinoplasty
may be required.
Open bite deformity (apertognathism)
Failure of occlusion when the jaws are brought together. It may be anterior, posterior, or
in both segments. Clinically: long lower third of the face, incompetent lips, upper
incisor show at rest and gingival exposure on smiling,
speech
impairment,
and
difficulty
in
mastication.
Cephalometry: ↑ anterior facial height (N-Me), steep
mandibular plane, and height of ramus (Ar-Go) is often
reduced. Treatment: in few cases, orthodontic therapy is
adequate. When surgery is planned, anterior segmental
upper and lower osteotomies, posterior upper segmental
osteotomy
(Schuchardt
procedure),
sagittal
split
osteotomy, and Le Fort I osteotomy are available options.
MANAGEMENT OF PATIENTS WITH MAXILLOFACIAL DEFORMITIES
History: chief complaint; medical and dental history; oral habits.
Clinical examination: Extraoral: the patient should be
examined in a neutral position with the Frankfort horizontal
parallel to the floor and teeth in centric occlusion. In the frontal
view, the facial height is divided into 3 thirds by horizontal
lines: the upper 1/3 from trichion to glabella, the middle 1/3
from glabella to subnasale, and the lower 1/3 from subnasale
to menton. In the normal face, these thirds are usually equal.
The lower 1/3 is further subdivided into 3 equal parts, the lips
should meet near the junction of upper and middle thirds.
Facial profile is also inspected which can be convex, straight,
or concave. TMJ, ear, and neck should also be examined.
Intraoral: mouth opening, oral hygiene status, palatal and lingual anatomy, dental
occlusion, lateral and protrusive movement of mandible, and deglutition.
Investigations: Radiographs including panoramic and lateral cephalometric radiographs
along with a full series of photographs to evaluate the facial skeleton. Mounted study
models are also required to simulate surgery and to fabricate intra-operative splints.
Indications of orthognathic surgery: skeletal deformities which are not amenable to
routine orthodontic management like those in patients:
who cannot retrude (or protrude) into an edge-to-edge occlusion i.e. Class III (or
Class II) occlusion [overjet > 10 mm].
with anterior open bites due to skeletal causes.
with true asymmetry.

Orthognathic Surgery
Seminars in Oral Surgery
٤
with marked discrepancies in the vertical dimension.
who are unwilling to accept appliance therapy.
Presurgical orthodontics
Objectives: 1) Proper alignment of teeth: by decrowding, space closure, and ideal
inclination. Optimum occlusal relationship at the time of osteotomy contributes to long
term stability of the mobilized skeletal segments.
2) Decompensation: skeletal malocclusion is usually accompanied by natural dental
compensation which reduce the extent of real deformity. Teeth should be compensated
to prevent occlusal discrepancies after surgery, e.g. expansion of maxillary arch to
accommodate the wider portion of the advancing mandibular arch in the treatment of
skeletal CII malocclusion.
3) Creating interdental space for segmental osteotomies.
Preoperative planning
After identifying the deformity, different patient's records can be utilized to simulate
surgical procedures, to predict the outcome, and to define the operative plan. Simulated
(mock) surgery can be performed on the following records:
Mock surgery on dental study models (model surgery): Traditional model surgery can
be used to transfer the workup to the operating room. A set of dental study models
mounted on articulator enable to plan the surgical correction. After drawing marking
lines on the cast corresponding to the planned osteotomies, the cast is sectioned at
these lines and the segments are repositioned according to the type of surgery. The
cast is then secured with sticky wax, and an acrylic splint is fabricated, to serve as an
intra-operative guide of occlusion after repositioning.
Mock surgery on cephalometric tracings: transparent sheets are applied on
cephalogram and anatomical landmarks are traced on the sheets to simulate the
planned surgical procedure and see the resultant profile.
Mock surgery on photographs: a scissor is used to cut portions of the facial anatomy
from the lateral photographs to allow measuring the magnitude and direction of
skeletal and soft tissue change needed.
Computer-aided planning: various hardware and software combinations are available
that create 3-D images from cephalometric or CT data provided by the original
scanner. Imaging software permits virtual osteotomies to be created that can be
manipulated and repositioned according to the anticipated surgical plan.
MANDIBULAR ORTHOGNATHIC PROCEDURES
Sagittal split osteotomy (SSO)
History: Hugo Obwegeser first developed this technique. He aimed to design an
osteotomy that could be performed transorally with broad contacting bone surfaces.
After studying cadaver mandibles, the first clinical case was performed in 1953, under
local anesthesia. The initial osteotomy was limited to the ramus only. Over the next 30
years, multiple modifications by Obwegeser and others were suggested. The most
common one currently performed include the buccal cortex of the mandibular body in
Orthognathic Surgery
Seminars in Oral Surgery
٥
the area of the second molar. The original osteotomies were secured with wire
osteosynthesis, while today’s SSO includes rigid fixation.
Indications: SSO is a versatile technique in that it allows wide range of mandibular
movement, so it can be used for mandibular prognathism, retrognathism, and lateral
deviations. It could also be used to correct anterior open bite (but relapse rate is high).
Contraindications: the presence of unerupted second molars; a severely narrow
anteroposterior or mediolateral dimension of the ramus with no medullary bone
between the buccal and lingual cortices; and significant mandibular asymmetry.
Advantages: avoidance of external scar because it is done intraorally; wide area of
cancellous bone contact with rapid bone consolidation; wide range of positional
changes between the fragments; minimum spatial alteration between condyle and
glenoid fossa; and possible use of internal rigid fixation.
Disadvantages: high incidence (up to 80%) of lower lip altered sensation (anesthesia or
paresthesia). Limitations: should not be used alone to close anterior open bite because
of high rate of relapse.
Procedure: The incision typically extends 1 cm up on the
anterior ramus and continues inferiorly along the external
oblique ridge into the mandibular vestibule to the mesial
side of the first molar, often with a vertical release.
Subperiosteal dissection is carried to the inferior border of
the mandible in the molar region. The anterior border of
the ramus is stripped of the temporalis attachment to the
tip of the coronoid. Dissection is also performed along the
medial aspect of the ascending ramus to identify the
sigmoid notch and the lingula.
The medial ramus corticotomy is completed with either a thin reciprocating saw or a
bur. The osteotomy is then carried along the external oblique ridge and buccally down
through the inferior border of the cortex. The junction areas between osteotomies
should be checked for continuity. Then, a series of osteotomes of increasing width are
used to achieve the split. Once the SSO is completed bilaterally, the mandible should be
repositioned into its planned position. Bone trimming from either the proximal or distal
segment is required in mandibular setback or rotation surgeries . Once the tooth-bearing
segment of the mandible is repositioned and IMF performed, the SSO is rigidly fixated.
Vertical ramus osteotomy (VRO)
History: VRO first developed by Caldwell and Letterman in 1954, through an extraoral
approach. Its novelty lay in that it was an osteotomy that minimized injury to the
mandibular nerve. In 1970, intraoral approach was described. Some authors also
championed VRO as a treatment of TMJ dysfunction.
Indications: mandibular prognathism is the primary indication. VRO can also be used
for mild mandibular retrognathism to advance the mandible for no more than 2 mm.
Contraindications: patients with tendency toward hypertrophic and keloid scar
formation (extraoral approach); limited mouth opening (intraoral approach).
Advantages: facility of execution; avoidance of injury to the inferior alveolar nerve; and
teeth do not have to be sacrificed.
Orthognathic Surgery
Seminars in Oral Surgery
٦
Disadvantages: cutaneous scar and risk of injury to marginal mandibular nerve
(extraoral approach); requires special instrumentation for exposure and osteotomy
(intraoral approach); long postoperative IMF (3 weeks wire + 2-3 weeks elastics);
unsuitable to use rigid internal fixation.
Extraoral approach: submandibular incision is made followed
by dissection through the platysma muscle to expose the
mandibular angle. The masseter muscle is raised from bone by
subperiosteal elevation, from the lower border to the sigmoid
notch. The osteotomy is made with a powered reciprocating saw
from the deepest part of sigmoid notch to just anterior to the
angle. After repositioning of distal segment, IMF is done.
Intraoral approach: The incision starts on the anterior border of the ramus 1 cm
posterior to the third molar region and sweeps forward into the buccal vestibule to the
area adjacent to the first molar. Dissection of the lateral ramus is then performed antero-
posteriorly until identifying the sigmoid notch and the posterior border of the ramus.
Bauer retractors are placed in the sigmoid notch superiorly and at the antegonial notch
inferiorly. Use of fiberoptic Bauer retractors is also helpful for illuminating the surgical
cavity and maximizing visualization. VRO saw is used to create the osteotomy which
should relate posterior to the antilingula, down the lateral ramus to the antegonial angle.
Once bilateral VROs are completed, the mandible should be passively repositioned
posteriorly into final occlusion. The proximal segments are lateralized. IMF is
established, and the wound is irrigated and closed.
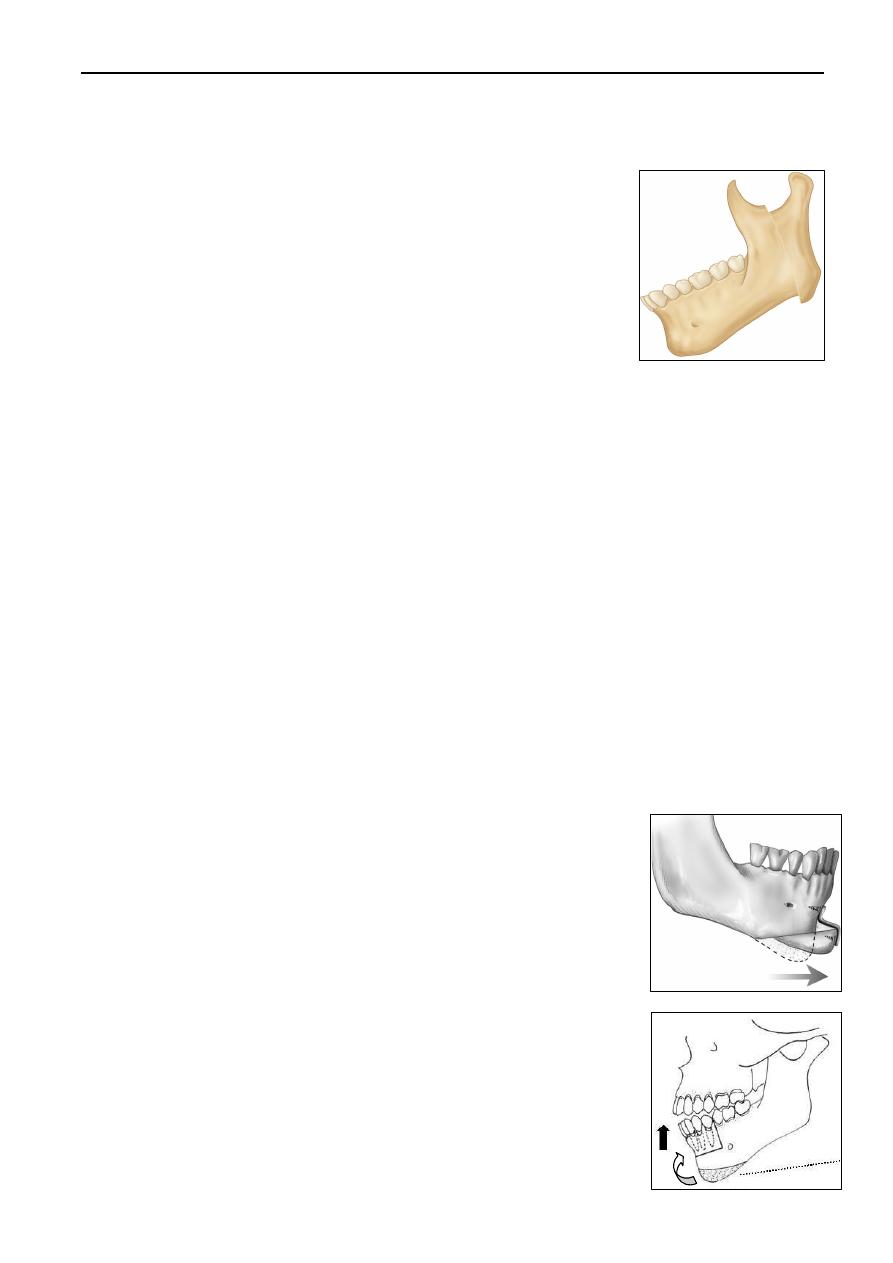
Oblique vertical ramus osteotomy (Thoma): the osteotomy is made from the sigmoid
notch to a point posterior to the mandibular angle.
Inverted L ramus osteotomy (Trauner): the horizontal limb is made above the
mandibular foramen, and the vertical limb dropped down behind the foramen, parallel
to the posterior border of the ramus. Indication: treatment of mandibular prognathism.
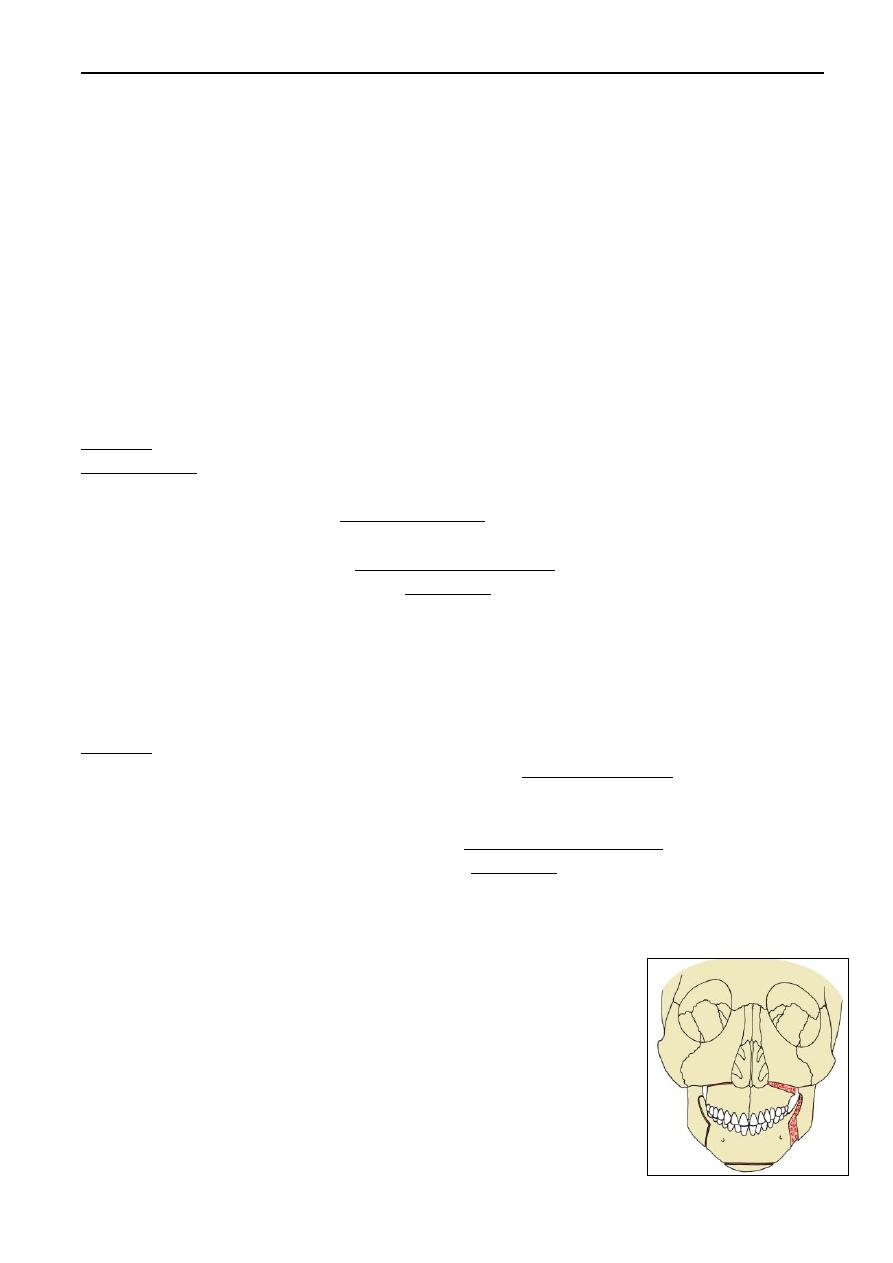
Sliding genioplasty
First described by Hofer in 1942 using external approach.
Nowadays the procedure is done by intraoral degloving
technique. An anterior labial incision is followed by subperiosteal
dissection to the lower border and around the mental foramen. A
powered saw is used for doing osteotomy. After repositioning, the
mobilized segment is rigidly fixated by miniplates. Indications:
correction of microgenia, macrogenia, or laterognathism, and in
patients with vertical symphyseal abnormalities.
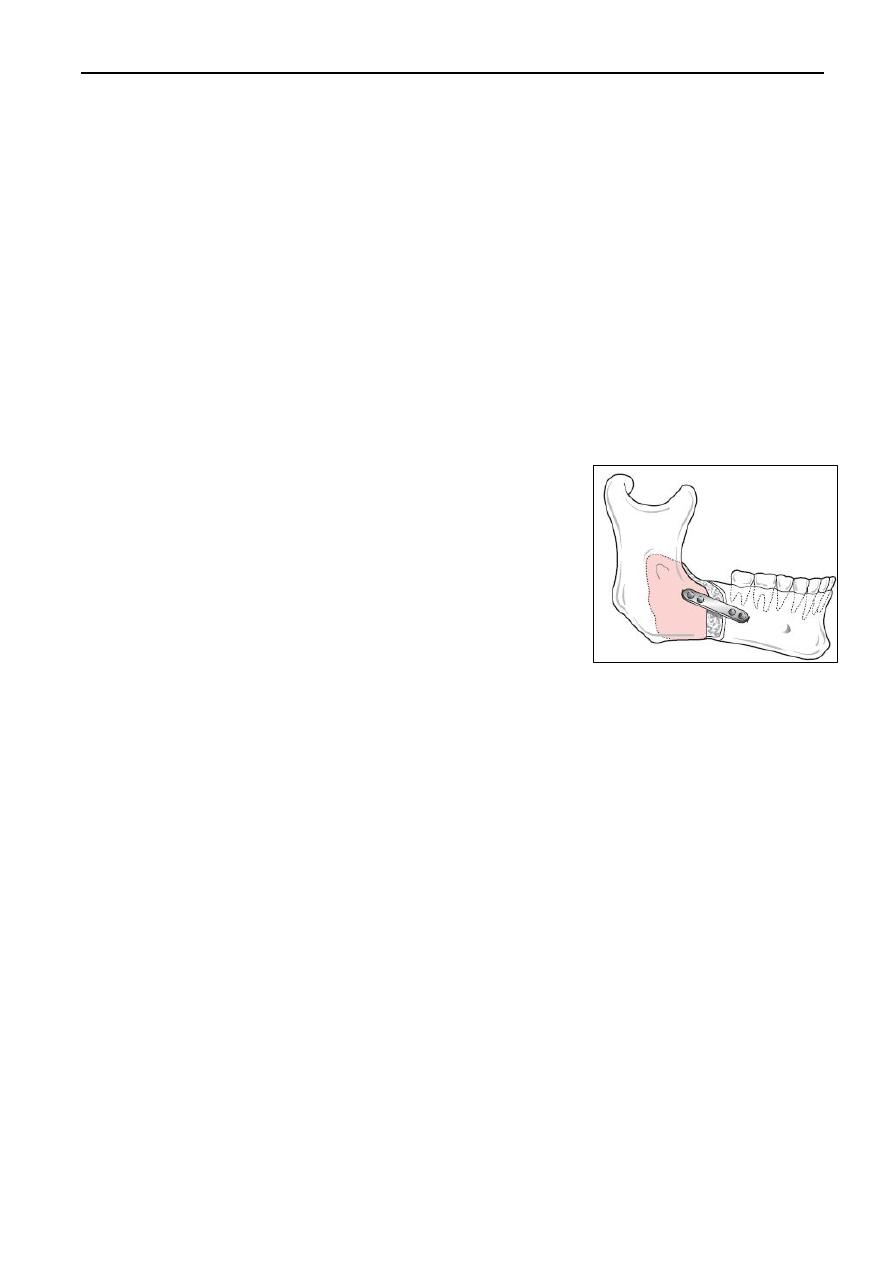
Anterior segmental mandibular osteotomies: Köle procedure
Procedure: A transverse anterior segmental osteotomy is made at
least 5 mm below the teeth apices. The anterior open bite is
closed, and the resulting defect is filled with bone taken from the
inferior border of the symphysis. Indication: to correct minor
anterior open bite and reduce the vertical height of the symphysis.
Orthognathic Surgery
Seminars in Oral Surgery
٧
Mandibular body osteotomies: rarely used. The main drawbacks: possible injury to
inferior alveolar nerve, creation of dental gaps, technical difficulties, need to provide
soft tissue coverage for osteotomy sites, and need for bone grafts.
MAXILLARY ORTHOGNATHIC PROCEDURES
LeFort I Osteotomy
Indication: for treatment of maxillary retrognathism, maxillary protrusion, or skeletal
open bite for maxillary advancing, setting back, or downfracturing respectively.
Segmental LeFoet I osteotomies can also be used to treat transverse maxillary
derformities and to correct long face deformity.
Procedure: Local anesthetic with vasoconstrictor is injected into the maxillary
mucobuccal fold prior to giving general anesthesia to allow time for the vasoconstrictor
to take effect. A circumvestibular incision, extending from first molar to first molar, is
made through the buccolabial mucoperiosteum. Subperiosteal dissection begins at the
piriform rim and is carried superiorly and laterally along the anterior maxilla, and then
posteriorly toward the pterygomaxillary fissure. A fine periosteal elevator is used to
elevate the nasal floor.
A reciprocating saw is used to make a horizontal osteotomy from the maxillary buttress
to the piriform rim on each side. The nasal septum is separated from the nasal crest of
the maxilla using a septal osteotome. The pterygoid plates
are separated with a small, sharp and curved osteotome.
After complete mobilization of maxilla is achieved, it can be
repositioned forward or backward according to procedure,
and temporary IMF is performed using the prefabricated
oral surgical splint. Excess bone is removed and maxilla is
rigidly fixated in the new position. Bone grafting is needed
in advancement surgery. IMF is released and occlusion is
checked before wound irrigation and closure, followed by
definitive IMF.
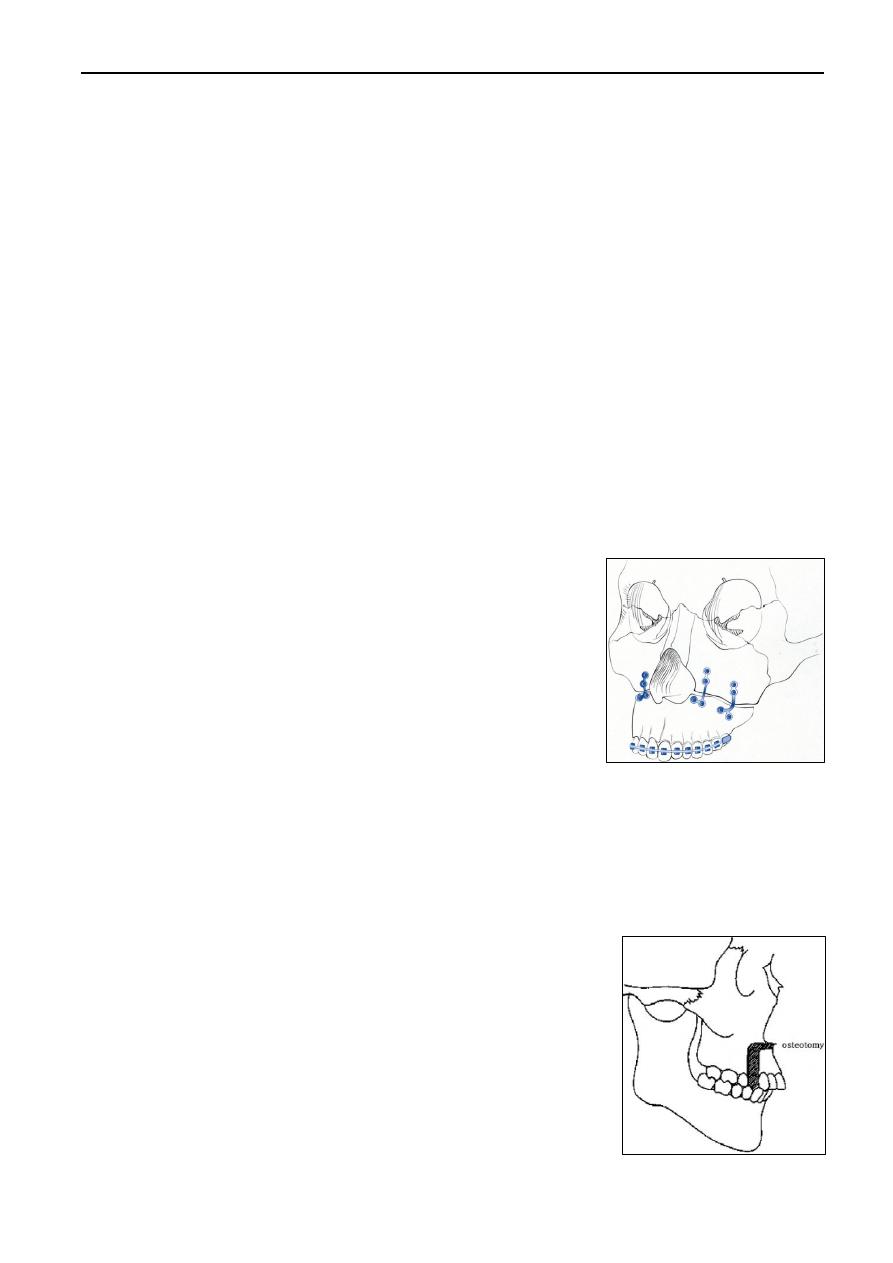
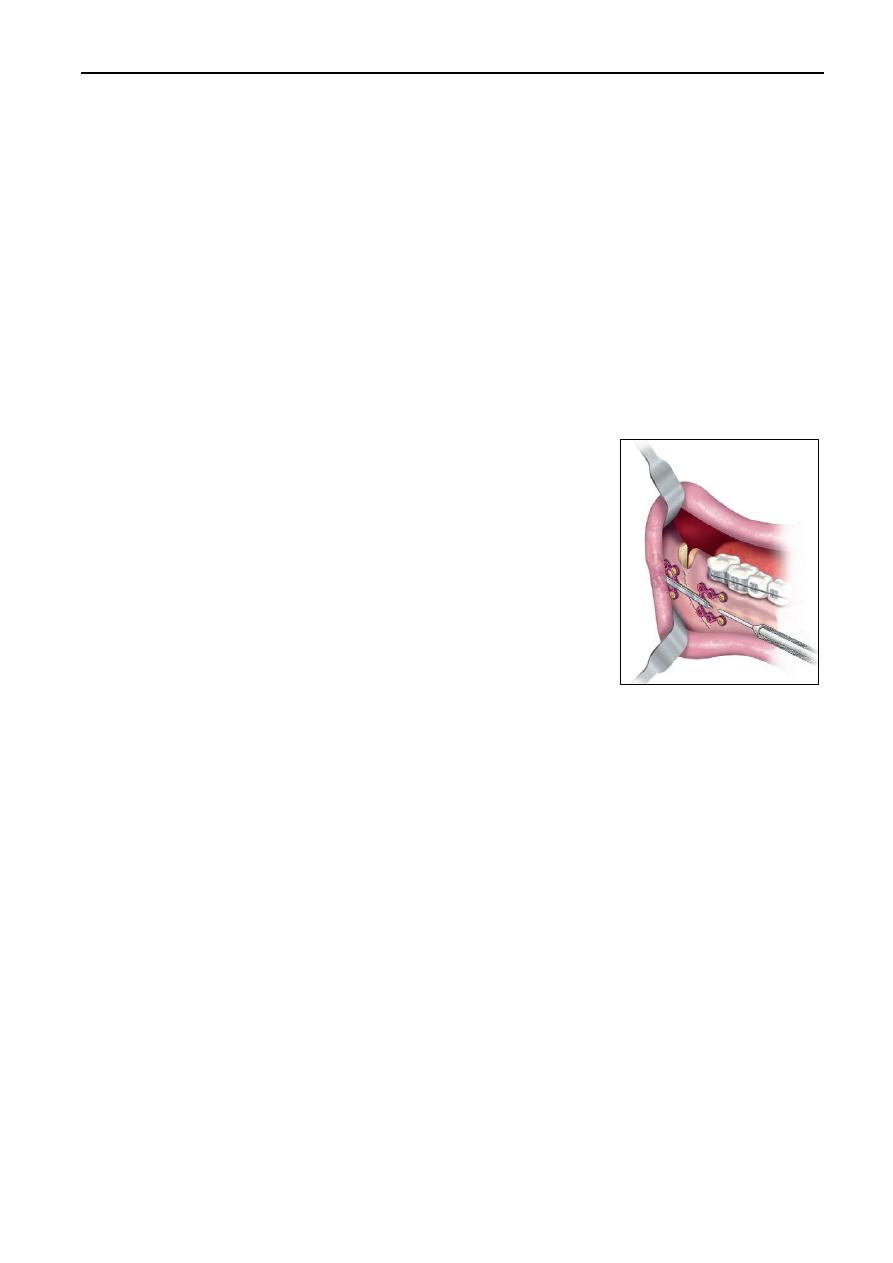
Segmental maxillary osteotomies
Anterior segmental maxillary osteotomy is indicated primarily for correction of dento-
alveolar protrusion. Other indications: correction of anterior open bite, closure of dental
spaces between segments, and combined with other osteotomies to achieve optimal
correction of dentofacial aesthetics and occlusion. Three techniques are available: in
Wassmund procedure, a tooth (premolar) is extracted and a
vertical bone cut is performed on the extraction space. The
horizontal osteotomy between the canine root tip and the
piriform rim is then carried out to connect the vertical
osteotomies on the right and left sides. Horizontal osteotomy
is also performed on palatal side. The planned osteotomy sites
are reached by tunnelling under mucoperiosteum. The anterior
segment is then pushed posteriorly and inferiorly by surgeon's
fingers, and monomaxillary fixation is done with the posterior
upper teeth.
Orthognathic Surgery
Seminars in Oral Surgery
٨
In Wunderer modification, a palatal flap raised by means of a transverse incision of the
palate, while the anterior osteotomy is made after tunneling, leaving the buccal blood
supply intact. In downfracture technique, a buccal flap is raised, and the palatal
osteotomy is made after tunnelling, leaving the palatal blood supply intact.
Posterior segmental maxillary osteotomy (Schuchardt procedure) can be used to close
posterior open bite or anterior open bite due to premature posterior occlusion. It can be
done as one-stage or two-stage procedure.
OTHER TECHNIQUES
Distraction osteogenesis: a relatively new surgical technique based on the principle of
'tension stress' that allows lengthening of bone and surrounding soft tissues through
progressively controlled fracture separation by means of a distraction device. It was
early used by Ilizarov in the 1950s to lengthen limbs. McCarthy et al. initiated osteo-
distraction in the craniofacial skeleton in 1991, applying external distractor devices
similar to those of Ilizarov to the mandible.
Indications: can be used for mandibular or maxillary
lengthening and widening, ramus lengthening, and alveolar
ridge augmentation (for preprosthetic purposes).
Advantages: no need for bone grafting, associated soft tissue
lengthening, and diminished relapse.
Procedure: consists of 4 phases: osteotomy at the area to be
lengthened, latency period without activation which usually
takes 7 days after osteotomy, activation period in a rate of 1
mm per day, and consolidation period during which mature
bone is formed between osteotomy ends.
POSTOPERATIVE CARE OF ORTHOGNATHIC SURGERY PATIENTS
As with any maxillofacial surgical patient, protection of the airway is the primary
concern at extubation. In patients placed into wire/elastic IMF, the team should be
prepared to remove the wires on an emergency basis if needed. Postoperative antibiotics
and steroids are recommended during the first 24 hours. Detailed instructions are given
to patients about their diet and oral hygiene. Postoperative orthodontic therapy with
elastics or extraoral appliances may be required to treat 'immediate relapses' after
releasing the IMF. Replacement of missing teeth and closure of created spaces after
elongation procedures is achieved by fixed bridges or removable appliances.
COMPLICATIONS OF ORTHOGNATHIC SURGERY
Bad splits (inappropriate osteotomy), bleeding, neurosensory impairment in the mental
or infraorbital distribution, condylar sag, proximal segment malpositioning, TMJ
problems and condylar resorption, unesthetic scar (in extraoral approaches), nasal septal
deviation, maxillary sinusitis, malunion and non-union, tooth damage, infection, bone
necrosis, airway obstruction, speech changes, and relapse.