
Management of urinary stone
Diagnostic imaging
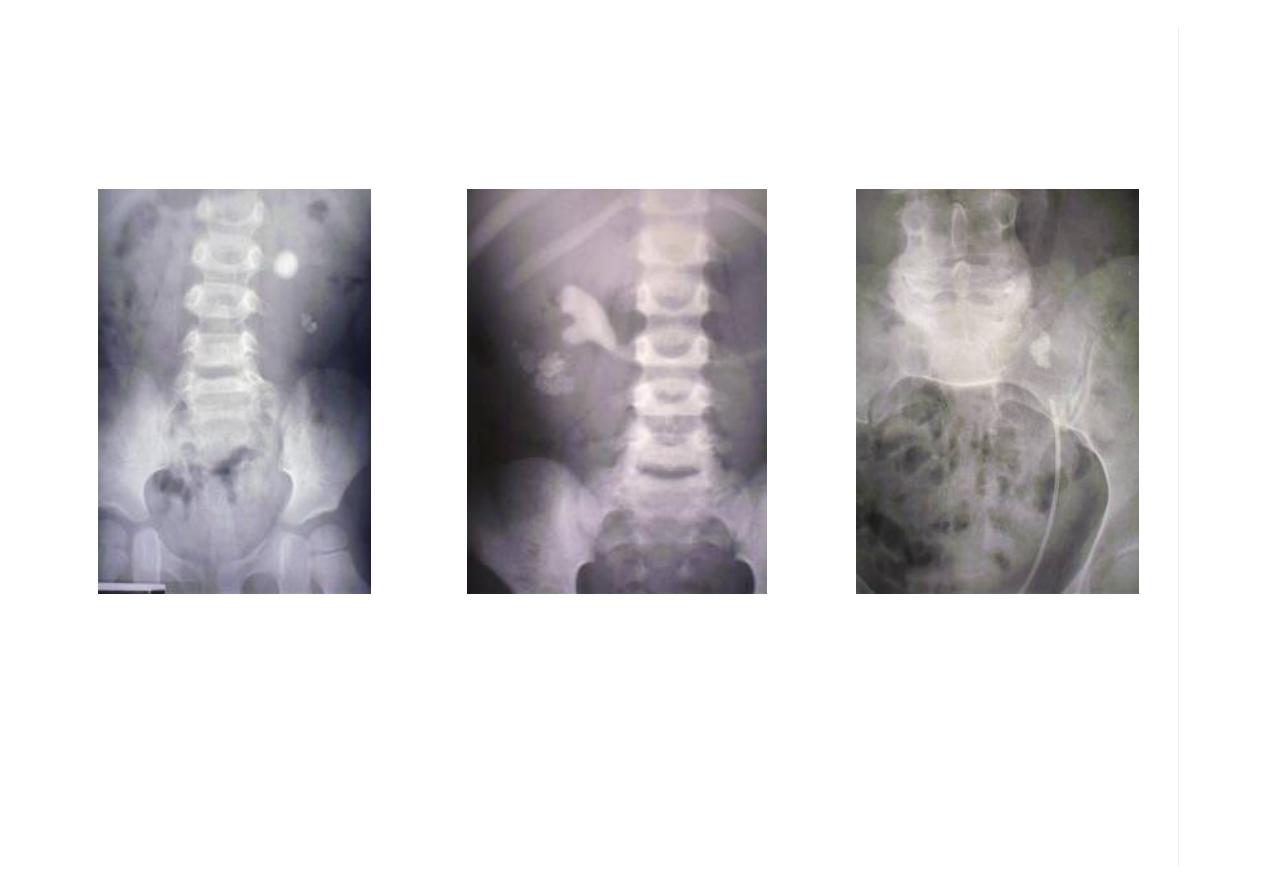
Routine examination involves a plain abdominal film of the
kidneys, ureters and bladder (KUB) At least 90% of all
renal stones are radiopaque and therefore readily visible
on a plain film of the abdomen

Loading…
RENAL CALCULI
Most (about 80% to 85%) patients harboring “simple” renal calculi can be treated
satisfactorily with ESWL
*One must consider stone-related factors (size, number, location, composition), renal
anatomy, and clinical factors of the patient
*Is the patient an appropriate candidate for SWL or should other treatment modalities
be used?

*Factors with poor stone clearance rates by ESWL
-large renal calculi (mean, 22.2 mm),
-stones within dependent or obstructed portions of the collecting system,
-stone composition (mostly calcium oxalate monohydrate brushite and cystine),
-obesity or a body habitus that inhibits imaging, and unsatisfactory targeting of the
stone
those patients may achieve a better outcome with a percutaneous nephrolithtomy
(PCNL) rather than with ESWL
Loading…
In summary,
-For patients with stones smaller than 10 mm, SWL is usually the primary approach.
-For patients with stones between 10 and 20 mm, SWL can still be considered a first-
line treatment unless factors of stone composition, location, or renal anatomy suggest
that a more optimal outcome may be achieved with a more invasive treatment modality
(PNL or ureteroscopy).
-Patients with stones larger than 20 mm should primarily be treated by PNL unless
specific indications for ureteroscopy are present (e.g., bleeding diathesis, obesity).

URETERAL CALCULI
-the width of the stone is the most significant measurement affecting the likelihood of
stone passage
-those with stones smaller than 4 mm, 4 to 6 mm, and larger than 6 mm experienced
rates of spontaneous passage of 80%, 60%, and 20%, respectively
-rate of spontaneous passage is highly dependent on stone location; passage rates
from the proximal, middle, and distal ureter were 22%, 46%, and 71%, respectively
-for patients with stones of 5 mm or less, conservative management should be
considered

-Infection associated with ureteral stones, or obstructed pyelonephritis, is a not
uncommon and potentially life-threatening urologic emergency
-Upper ureteric stone ESWL is the 1st option, and ureteroscope 2nd modality
-Middle ureteric stone treated by ureteroscpe (ESWL is C.I)
-Lower ureteric stone ureteroscope 1st option, ESWL if ureteroscope is not
recommended for anesthetic purpose or other C.I

Bladder stones
Usually manifestations of underlying pathologic condition, include voiding dysfunction
or foreign body.
~Voiding dysfunction may be due to urethral stricture, BPH, bladder neck contracture,
or flaccid or spastic neurogenic bladder, all of which result in static urine.
~Most bladder calculi seen in men.
~Stone analysis frequently reveals ammonium
urate, uric acid, or calcium oxalate stones

Presentation.
Irritative voiding symptoms, intermittent weak urinary stream, UTI, hematuria, or pelvic
pain.
Physical examination is unrevealing but DRE could elicit BPH,
Large percentage of bladder stones are radiolucent (uric acid)
U/S of the bladder identify the stone with its characteristic shadowing.
The stone move with changing position.
Stones within ureterocele don’t move with
body position. Usually treated by endoscopic incision &stone removal.

~Early instrument used to remove bladder calculi were both clever & bizarre.
~Simple mechanical crushing devices are still used today. It should be used with
caution to prevent bladder injury.
~cystolitholapaxy allow most vesical stone to be broken & subsequently removed.
Electrohydraulic, ultrasonic, laser, & pneummatic lithotrites may be used.
~cystolithotomy can be used through small
incision no more indicated now.
Loading…
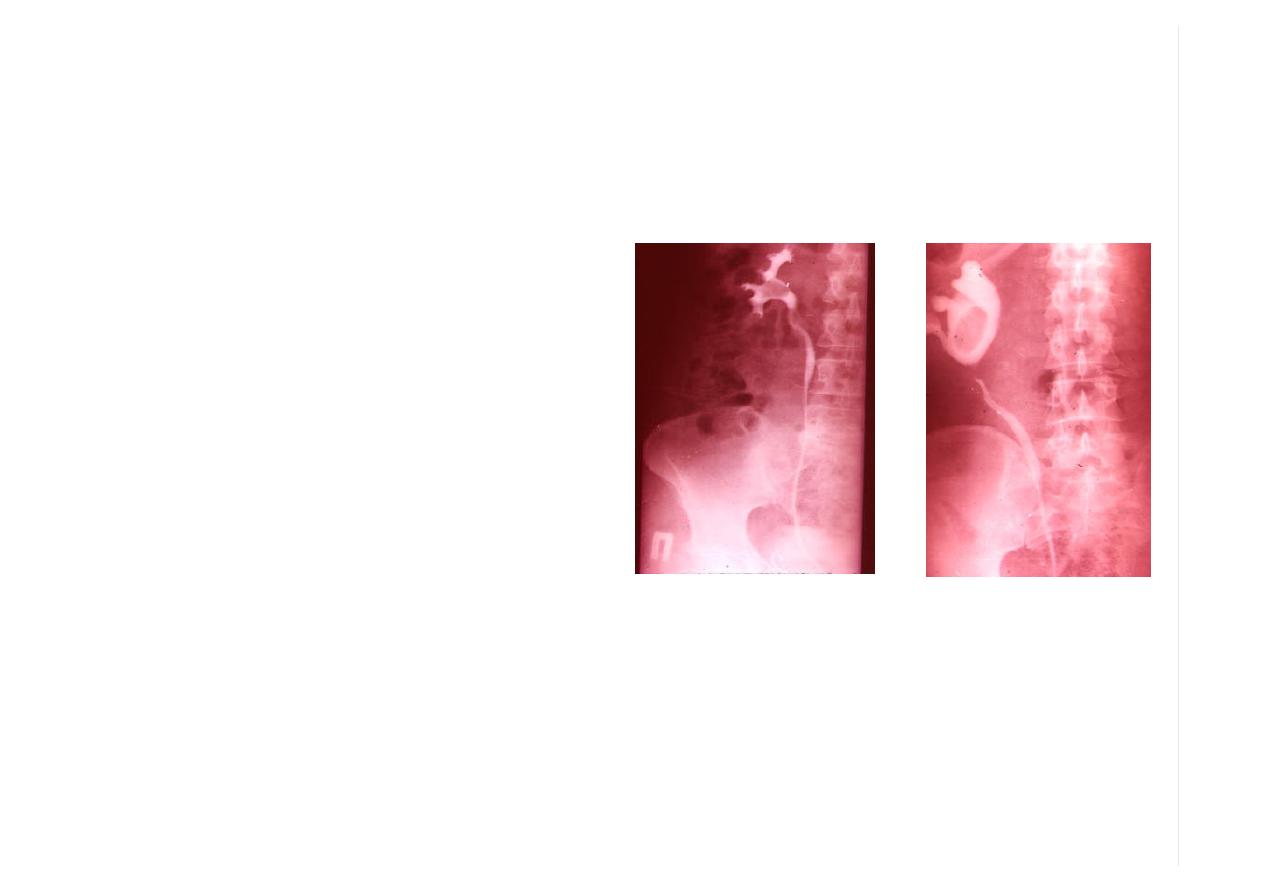
Diagnostic imaging
Excretory pyelography must not
be carried out in the following
patients - those:
•
With an allergy to contrast
media
•
With S-creatinine level > 200
µmol/L
•
On medication with metformin
should stop 24 hr. before
contrast to prevent lactic
acidosis
•
With myelomatosis contrast-
induced nephropathy in patients
with multiple myeloma

Extracorporial shock wave lithotirpsy
ESWL

ESWL
has revolutionized the treatment of urinary stone.
1st clinical application with successful fragmentation of renal calculi in 1980.
All require energy source to create shock wave, coupling mechanism to transfer the
energy from outside to inside the body, & either fluoroscope or ultrasound or both to
identify & position the calculi at a focus of converging shock waves.

Shock wave physics.
2 basic types of shock waves sources;
1-supersonic emitters
release energy in
confined space
, thereby producing an expanding plasma & an
acoustic shock wave.
such shock waves occur in nature –the familiar thunderstorm with lightening (electrical
discharge) followed by thunder (an acoustic sonic boom) is an analogous situation.
Under controlled conditions, such an acoustic shock waves can successfully fragment
calculi.

2-finite amplitude emitters.
Create shock waves by
displacing surface
activated by electrical discharge.
There are 2 major types of finite amplitude emitters.
Piezoceramic
result in shock wave after an electrical discharge causes the ceramic
component to elongate in such manner that the surface is displaced & an acoustic
pulse is generated.
Thousands of such component placed on the concave side of the spheric surface
directed toward a focus.

Electromagnetic.
similar in concept to stereo speaker system an electrical discharge to a slab, adjacent
to an insulating foil, create an electric current that repulses a metal membrane,
displacing it & creating an acoustic pulse into an adjacent medium.
These waves need to be focused toward the offending stone.
~All shock waves despite their source are capable of fragmenting stones when
focused.

Fragmentation is achieved by erosion & shattering .
~cavitational forces result in erosion at the entry &exit sites of the shock waves.
~shattering result from shock wave absorption
Preoperative evaluation.
Physical examination should be as thorough as in preparation for any surgical
procedure.
Vital signs including blood pressure should be noted.

Contraindications:
1-Pregnant women.
2-uncorrectable bleeding disorders.
3-Body habitus including any gross skeletal abnormalities, contractures, or excessive
weight may severely limit ESWL
4-pt. with large abdominal aortic aneurysm
5-Pt. with cardiac pacemakers should be thoroughly evaluated by cardiologist.
6-Lower ureteric stone in child bearing age
7-Eswl is not an option for mid ureteric stone.

Intraoperative considerations:
Stone localization-
proper pt positioning is prerequisite for successful lithotripsy.
Anterior located kidneys, medial oriented portions of horse shoe kidney, or transplant
kidneys are best treated in prone position.

Small or poorly calcified calculi can be difficult
to image with fluoroscopy.
Using radio contrast agent intravenous or by ureteral catheter may help to localize the
stone as filling defect.
Fluoroscopic imaging
.
Require adequate bowel preparation to decrease bowel gas & decrease radiation
exposure.
Ultrasonic imaging
.
Has the advantage of eliminating radiation exposure to the pt. or lithotripsy team.
Identify radiolucent or small calculi that are difficult to visualize with fluoroscopy.

Coupling.
Should have properties similar to those of human skin. Optimal system should prevent
pain, ecchymoses, hematomas, or skin breakdown. Interface between gas & tissue
can result in tissue damage.
Air bubbles entrapped by hair, by pandages from prior percutaneous procedures or by
inadequately degassed fluid, can significantly impede directed shock waves & result in
skin ecchymoses or breakdown.

Fragmentation
.
Safe shock wave dosage is unknown.
Shock waves induce trauma, including intrarenal & perirenal hemorrhage & edema,
thus the minimal shocks need to achieve fragmentation should be given.
Over treatment should be avoided since long term
complications are not yet known.
-double-j catheter should be placed to decrease the likelihood of obstruction in pt with
single kidney, or bilateral nephrolithiasis treated at the same session, and in large
stone burden.

Postoperative care
.
pt should be encourage to maintain active ambulatory state & excess fluid intake to
facilitate stone passage. Gross hematuria should resolve during the 1st post
operative week.
Follow up in approximately 2 weeks for discussion & evaluation of KUB & renal
ultrasonography will help assess success of fragmentation &passage of gravel.

Complications.
~
Perirenal hematoma (rare) pt presented with severe pain unresponsive to routine
medication CT should be taken to stage the injury.
~
steinstrrasse (stone street) columnation of stone gravel in the ureter usually occur in
large stone burden that’s why ESWL not indicated in stone >2.5-3cm.
-in asymptomatic pt follow up by serial KUB & u/s but in cases of sever pain &fever
require intervention by percutaneous nephrostomy drainage.

*
Pt. with large renal pelvic stone >1.5 cm have stone free rate at 3 months
approximately 75%,
-similar stone in lower calyx 50%,
*
Pt with small renal pelvic stone <1.5 cm have 90% stone free rate while
-similar stone in mid calyx have only 75%,
-or lower calyx 70%.

Percutaneous endourology
&ureterorenoscope
Retrograde instrumentation invade the urinary tract via the nature route of the urethra
under endoscopic guidance, while
Antegrade instrumentation
involve access via percutaneous puncture.
This approach must respect the renal anatomy &need imaging technique to guide the
procedure.

For percutneous puncture of the collecting system preparation & draping of the surgical
field is require as for open surgery, local anesthesia is sufficient for
small bore tract dilation.
puncture rout must be provide straightforward access to the target & safe blood less
instrumentation.
Visualization of the puncture needle &target &precise guidance to the target require the
use of imaging techniques such as u/s fluoroscope &in selected cases CT.

Indications of antegrade instrumentation .
Diagnostic
–antegrade pyelography.
Therapeutic
-nephrostomy catheter drainage
-antegrade ureteral stenting
-dilatation of ureteral strictures
-percutaneous endopyeloplasty
-percutaneous nephrolithotomy
-percutaneous resection &coagulation of urothelial tumor

Loading…
Antegrade pyelography.
Renal puncture is rarely indicated for diagnostic
purposes only. because less invasive radiographic techniques are available eg IVU,
U/S, CT, MRI, retrograde pyelography.
However, obtaining radiograph should be part of every percutaneous puncture for any
indications like, drainage & decompression of upper urinary tract if retrograde ureteral
catheterization is not advisable (eg, impassable ureteral obstruction due to stone,
tumor, or stricture).

Percutaneous nephrolithotomy (PNL)
Through the percutaneous nephrostomy tract nephroscope (endoscopic instruments
with
sheaths 15-26F that are inserted through a nephrostomy tract- under G.A- these have
telescopes with offset eyepieces).
However, ESWL is now used for treatment of > 90% of renal stones, percutaneous
lithotripsy & extraction of renal stones is still indicated in cases for which ESWL is not
primary choice

Indication 0f PNL:
1-
urinary obstruction not caused by stone itself, eg stone in caliceal diverticulum, stone
in association with puj obstruction. These stone could be broken up by ESWL, but
gravel not pass .
2-
large volume stone,( >3cm) eg, staghorn stones must be disintegrated by mechanical,
ultrasonic, electrohydrolic, or laser energy.
These stones need several session by ESWL& stone free rate only 30%.

3-
stones cannot be positioned within the focus of shock wave apparatus. Due to
anomalies of urinary tract or skeleton.
4-
lower pole caliceal calculi even under 2-3 cm range. The overall stone free rate with
ESWL is 60%.

ureterorenoscope
Is endoscopy of the ureter up to the renal pelvis for both diagnostic & therapeutic
purposes.
Ureteroscope can be rigid or flexible.
Indication of ureteroscope.
A-diagnostic:
1-lesions of the ureter or renal pelvis. If their nature cannot be determined by less
invasive procedures like retrograde pyelography, CT, or MRI.
2-hematuria from upper tract, however limited irrigation through ureteroscope resulting
in poor visibility sp. In gross hematuria.

B-therapeutic:
1-ureteral stone, although > 90% of ureteral stones can be treated by ESWL,
ureterorenoscopy still most frequently performed for treatment of ureterl stones.
Like distal or proximal ureteral stones not responding to ESWL.
Perforation of the ureter may occur, and treated by stenting using doubl-j for 2-6 weeks
usually allow healing without complications.
2-ureteral stricture, direct vision internal ureterostomy
3-ureteral tumor, endoscpic resection & coagulation.

1-stones that are most radiopaque and have density like
that of bone
a. calcium phosphate
b. calcium oxalate
c. cystine
d. magnesium ammonium phosphate
2-studies on urodynamics indicate that an increase in
diuresis generally ----- the rate of ureteral peristalsis
a. increases
b. reduces
c. flattens

4-the most accurate and certain means of diagnosing
vesical calculi remains the
a. KUB
b. ultrasonography
c. cystoscpic examination
d. CT scan
5-which of the following is an absolute contraindication to
ESWL
a. cardiac pacemaker and renal artery calcification
b. pregnancy and uncontrolled coagulation parameter
c. sever orthopedic deformity and serum creatinine more
than 3mg/dl
d. children and obstruction distal to stone

6-the most sever complication of ureteroscopy is
a. ureteric perforation
b. false passage
c. avulsion
d. stricture formation
7-radiolucent filling defect in the renal pelvis and ureter
include all of the following except
a. transitional cell carcinoma
b. blood clot
c. air
d. calcium phosphate stone