Stomach surgery Dr.Abdulhadi Alawadee
The stomach
• The stomach is a dilated part of the alimentary canal between the esophagus and the small
intestine.
• It is a muscular sac.
• It is a J-shaped.
• It occupies the left upper quadrant, epigastric, and
umbilical regions, and much of it lies under cover of the
ribs.
• Stomach located at level of T10 and L3 vertebral.
• Position of the stomach varies with bod Habitués
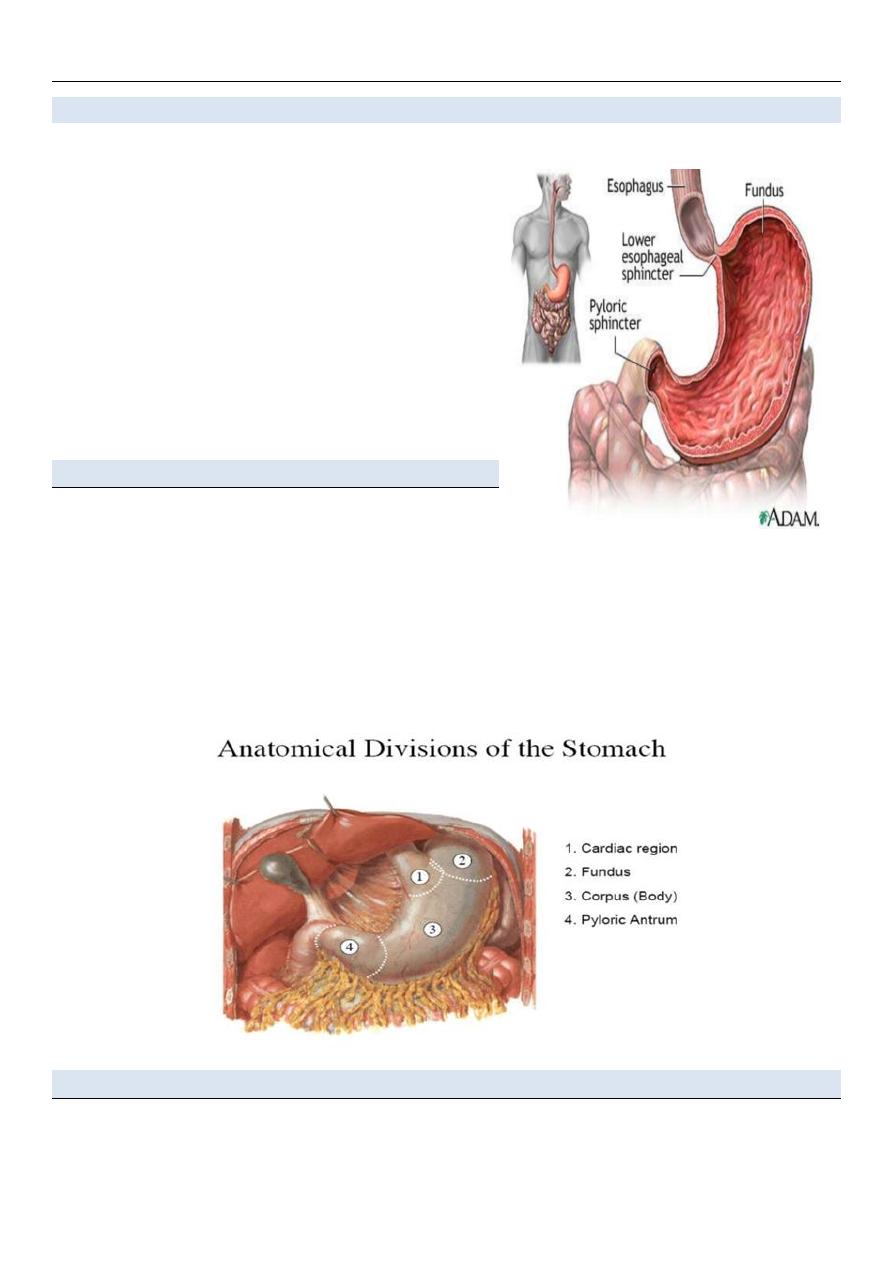
The stomach is divided into four regions:
1. The cardia, which surrounds the opening of the
esophagus into the stomach.
2. The fundus of stomach, which is the area above the level of the cardial orifice.
3. The body of stomach, which is the largest region of the stomach.
4. The pyloric part, which is divided into the pyloric antrum and pyloric canal and is the distal
end of the stomach.
Sphincters
Ø The cardiac sphincter (lower esophagus sphincter) closes off the top end of the stomach.
Ø The pyloric sphincter closes off the bottom.
Other features of thev stomach include:
• The greater curvature, which is a point of
attachment for the gastrosplenic ligament and the
greater omentum
• The lesser curvature, which is a point of
attachment for the lesser omentum.
• the cardial notch, which is the superior angle
created when the esophagus enters the stomach.
• the angular notch, which is a bend on the lesser
curvature.
Stomach Anatomical Relation
Antero-superior Surface
• The left half of this surface is in contact with the
diaphragm, which separates it from the base of the left
lung, the pericardium, and the seventh, eighth, and ninth
ribs, and intercostal spaces of the left side.
• The right half is in relation with the left and quadrate
lobes of the liver and with the anterior abdominal wall.
The Postero-inferior surface
is in relation with the diaphragm, the spleen, the left
suprarenal gland, the upper part of the front of the left
kidney, the anterior surface of the pancreas, the left
colic flexure, and the upper layer of the transverse mesocolon.
These structures form a shallow bed, the stomach bed, on which the viscus rests.
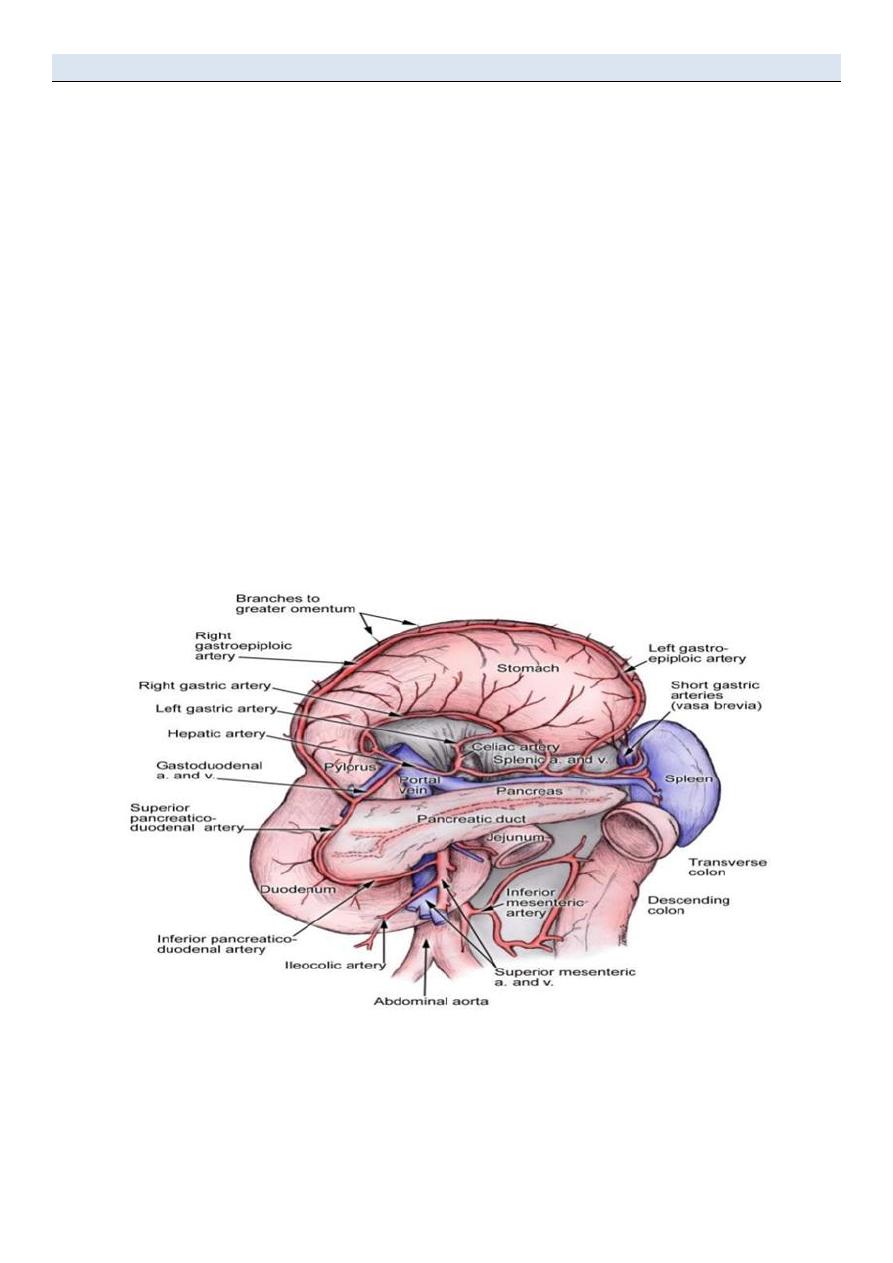
Stomach Blood Supply
Arterial blood supply(Coeliac trunk) : 3 Branches
• Left Gastric Artery
– Supplies the cardia of the stomach and distal esophagus
• Splenic Artery
– Gives rise to 2 branches which help supply the greater curvature of the stomach
» Left Gastroepiploic
» Short Gastric Arteries
• Common Hepatic or Proper Hepatic Artery 2 major branches
» Right Gastric- supples a portion of the lesser curvature
» Gastroduodenal artery
-Gives rise to Right Gastroepiploic artery
-helps supply greater curvature in conjunction with Left Gastroepiploic Artery
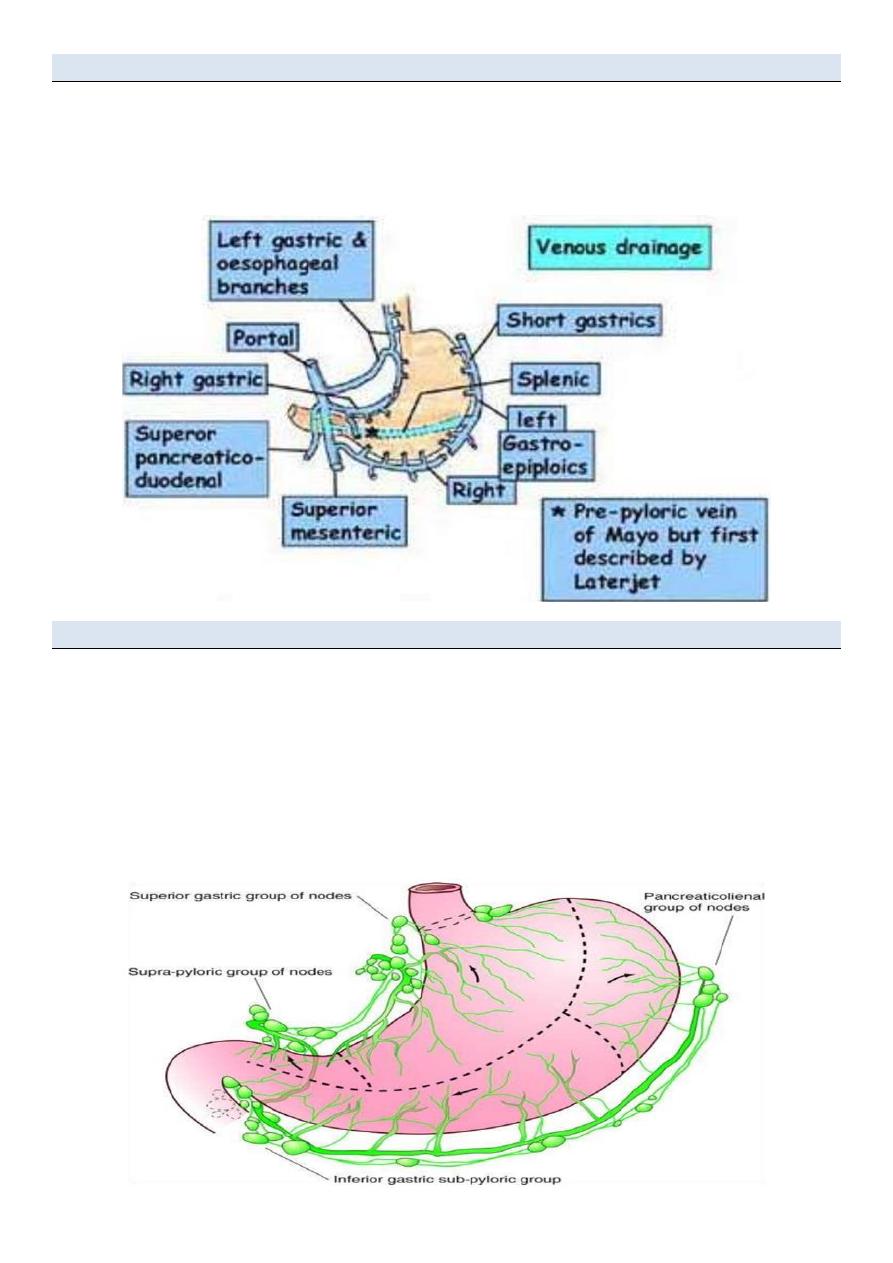
Stomach Venous Drainage
• Parallels arterial supply
• Rt &Lt gastric veins drain to the portal
• Rt gastroepiploic drains to the SMV
• Lt gastroepiploic drains to the splenic
Stomach Lymphatic Drainage
– Lymph from the proximal portion of the stomach drains along the lesser curvature first drains into
superior gastric lymph nodes surrounding the Left Gastric Artery.
– Distal portion of lesser curvature drains through the suprapyloric nodes.
– Proximal portion of the greater curvature is supplied by the lymphatic vessels that traverse the
pancreaticosplenic nodes.
– Antral portion of the greater curvature drains into the subpyloric and omental nodal groups.
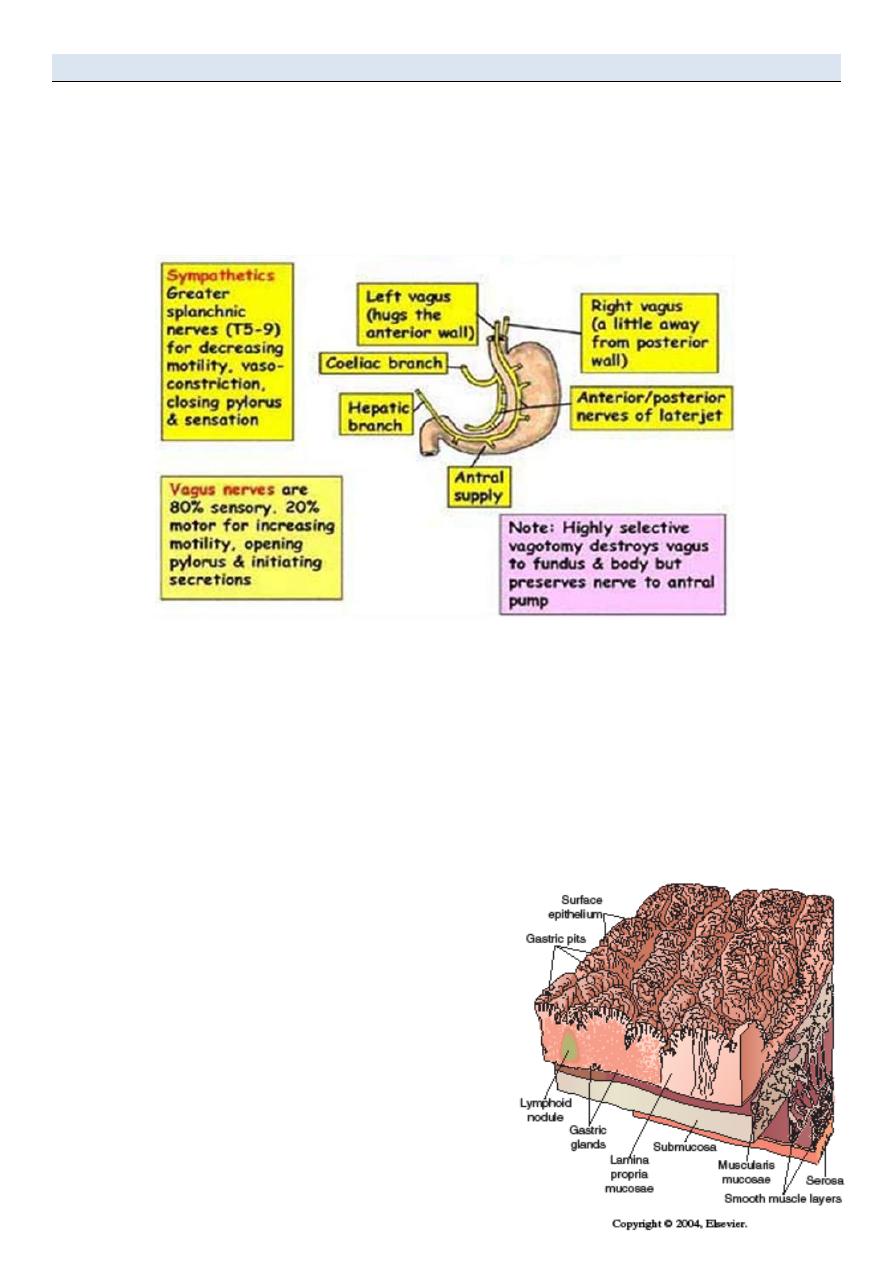
Stomach Innervations
The main innervations are Left and Right Vagus Nerves.
• Parasympathetic innervation of Stomach- Vagus Nerve
– 90% of fiber in vagal trunk is afferent (info transmitting from stomach to CNS)
• Sympathetic innervation of Stomach- Splanchnic Nerve
– Derived from spinal segement T5-T10
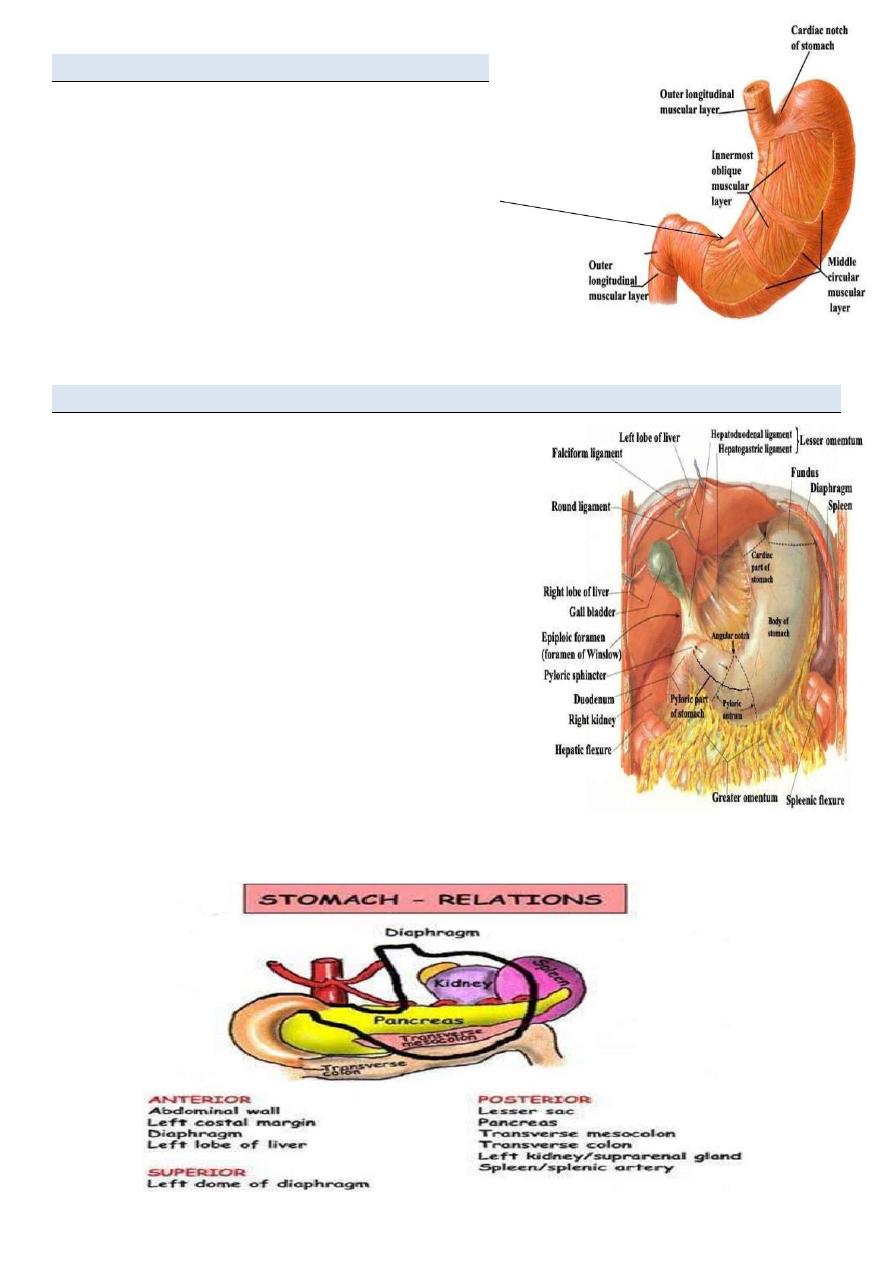
•The stomach is almost entirely covered with peritoneum.
•The peritoneum forms the outer gastrc serosa.
•Beneath the serosa is the muscularis propria.
•The MP is made up of 3 layers of smooth muscle.
•The middle layer is the circular muscle and is the only “complete” layer of muscle
•As you progress distally the middle layer of muscle
begins to thicken and form the pyiorus ,which
functions as a true sphincter.
•This and the GE junction form the gastric “borders”
and are the two “fixed” points of the stomach.
•The outer muscle layer (longitudinal) is contiguous
with the outer layer of the esophagus.
•The submucosa lies between the MP and the mucosa.
It is a collagen rich layer of connective tissue and is the
strongest layer of the gastric wall.
•The submucosa also contains the rich blood vessel network and the lypmhatics as well as
Meissner‟s plexus.
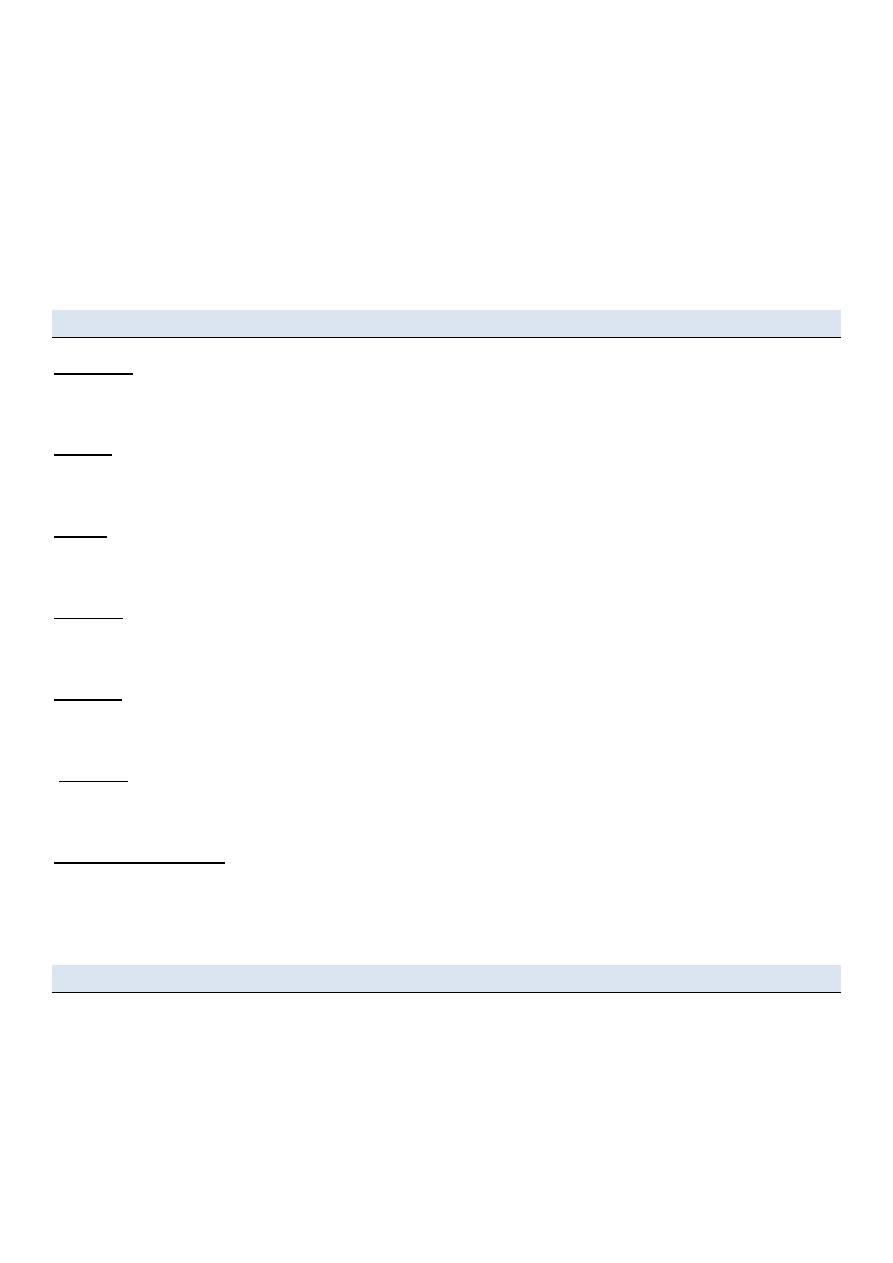
The mucosa consists of 3 layers:
•Surface epithelium (columnar).
•Lamina propria : Connective tissue layer that supports the surface epithelium.
•Muscularis mucosae (probably the reason for rugal folds). The MM is the boundary for
invasive/noninvasive gastric cancer.
Cell Types
•Parietal:
•Location: Body •Function: secrete acid and intrinsic factor
•Chief:
•Location: Body •Function: produce Pepsin
•ECL:
•Location: Body •Function: Histamine production
•G cells:
•Location: Antrum •Function: Gastrin production
•D cells:
•Location: Body, Antrum •Function: produce Somatostatin
•Mucus:
•Location: Body, Antrum •Function: mucus production
•Surface epithelium:
•Location: Diffuse •Function: produce mucus, bicarb, prostaglandins
Gastric Physiology
•Principle Function:
• Storage:
Receptive relaxation
• Start digestion:
Separates meal into fat/protein/carbohydrates

Regulation of Function
•The stomach is under both neural and hormonal control.
Gastric Hormones:
•Synthesized as inactive precursors
•Converted to active form by post-translational modification
• stimulus for release is: FOOD
•Composition of food dictates timing and specific hormone release.
Inhibition:
•Removal of stimulus
•Negative feed-back loops
•Inhibitory peptides, ie. Somatostatin
Gastric Hormones:
•Gastrin
•Somatostatin
•Gastrin-releasing peptide (GRP)
•Histamine
Gastrin
•Synthesis: G-cells in the antrum
•Release: AA, protein, vagal tone, antral distention, GRP, pH > 3.0, ETOH, Histamine.
•Inhibition:
•pH < 3.0, somatostatin, secretin, CCK, VIP, GIP, glucagon.
•Target cells: Parietal and Chief cells
•Action(s):
• Stimulates acid secretion
• Direct action on parietal cells
• Potentiating interaction with histamine
• Possible: releasing of histamine
• Stimulates motility in stomach, intestine, and gall bladder
• Inhibits contraction of pylorus and sphincter of Oddi.
• Stimulates GI mucosal growth.

Somatostatin
•Synthesis: CNS, antrum, fundus, sm. bowel, colon, and D-cells in pancreas.
•Release:
• Antral acidification
• Fats, protein, acid in duodenum
• Pancreatic: glucose, amino acids, CCK
•Inhibition:
•Release of acetyl-choline from vagal nerve fibers
•Action(s):
• The “master off switch”
• Inhibits the release of most GI hormones
• Inhibits pancreatic and GI secretion(s)
• Inhibits intestinal motility.
•Clinical:
• Octreotide- decrease fistula output
• Treatment of esophageal variceal bleed
• Can ameliorate symptoms of endocrine tumors
GRP
•Synthesis: Gastric antrum, small bowel mucosa
•Release: vagal stimulation
•Action(s):
• The “master on switch”
• Stimulates the release of all GI hormones (? Secretin).
• Stimulates GI secretion
• Stimulates GI motility
• * most important: stimulates gastric acid secretion and release of antral gastrin
Histamine
• •Stimulates parietal cells
• •Found in ECL cells and resident Mast cells.
• •Release is stimulated by: Gastrin, acetyl-choline, epinephrine
• •Inhibited by Somatostatin.
• A necessary intermediary of acid production.
Acid Secretion
Two forms:
• Basal Acid Secretion
• Stimulated Acid Secretion
Stimulated Acid Secretion
Three Phases:
• •Cephalic phase
• •Gastric phase
• •Intestinal Phase
These phases occur concurrently NOT consecutively.
Cephalic Phase
• Originates with the sight, smell, thought or taste of food.
• Stimulates the cortex and hypothalamus.
• Signals cause Vagus to release Ach, Ach causes increase in parietal cell acid production.
• Accounts for 20-30% of acid production.
Gastric Phase
• Begins when food enters the gastric lumen (gastric distention).
• Digestion products stimulate the G cells, they release gastrin, parietal cells release acid.
• Distention alone can increase acid production.
• Accounts for 60-70% of acid production.
• Phase lasts until the stomach is empty.
Intestinal Phase
• Poorly understood.
• initiated by chyme entering the small bowel.
• Accounts for ~10% of acid production.
Other functions
• Gastric acid suppression
• Mucosal protection
• B12 absorption
INVESTIGATION OF THE STOMACH AND DUODENUM
Contrast radiology
Upper gastrointestinal radiology is not used as much as in previous years, as endoscopy is a more
sensitive investigation for most gastric problems
Flexible endoscopy is the most commonly used and sensitive technique for investigating the
stomach and duodenum
Great care needs to be exercised in performing endoscopy to avoid complications and missing
important pathology
Axial imaging, particularly multislice CT, is useful in the staging of gastric cancer, although it
may be less sensitive in the detection of liver metastases than other modalities
CT/positron emission tomography
Positron emission tomography (PET) is a functional imaging technique which relies on the uptake
of a tracer in most cases by metabolically active tumour tissue. Fluorodeoxyglucose (FDG) is the
most commonly used tracer.
Endoscopic ultrasound is the most sensitive technique in the evaluation of the „T‟ stage of gastric
cancer and in the assessment of duodenal tumours
Laparoscopy is very sensitive in detecting peritoneal metastases, and laparoscopic ultrasound
provides an accurate evaluation of lymph node and liver metastases
Gastric emptying studies
These are useful in the study of gastric dysmotility problems, particularly those that follow gastric
surgery. The principle of the examination is that radioisotope-labelled liquid and solid meals are
ingested by the patient and the emptying of the stomach is followed on a gamma camera.
Angiography
Angiography is used most commonly in the investigation of upper gastrointestinal bleeding that is
not identified using endoscopy. Therapeutic embolisation may also be of valuein the treatment of
bleeding in patients in whom surgery is difficult or inadvisable. In expert centres embolisation now
replaces surgery in the majority of cases.
Thanks
Lec.1