Surgery Dr.Abd Al Hadi
HELICOBACTER PYLORI
1-Gram + spiral bacteria
2-Produces Urease
3-Found in gastric auntrum & area of gastric metaplasia in the duodenum deep to
mucous layer closely adherent to epithelial
surface, protected from acid & pepsin digestion by over lying mucous, bicarbonate &
by release of ammonia (Urease action) & high PH.
4-Prevalence increases with age & 2/3 are acquired in childhood.
5-Person to person transmission
6-Found in 90% of patients with DU & 70% with GU.
Pathogenesis
1-Increases fasting & postprandial gastrin.
2-Increases pepsinogen secretion
3-Decreases gastric mucosal resistance
4-Suppresses somatostatin release
5-Releases tissue damaging cytotoxins
-Cag
– A (Cytotoxin associated gene)
-Vac
– A (Vacillating Cytotoxin)
Clinicopath. features
1-Though 2/3 of population are infected with H. pylori, only 10 to 15 % develop PU &
the majority are asymptomatic.
2-Lead to acute gastritis
chronic gastritis
o & PU
3-Long standing chronic gastritis >>> > gastric atrophy & increased risk of
metaplasia & the earlier H. pylori acquired , the greater is risk of Ca .
4-More than 90% of MALT lymphomas have H. pylori & low grade tumours regress
with H. pylori eradication
5-Treat all patients with H. pylori because of associated risk of Ca.
Diagnosis
1-Rapid Urease breath test:-
Used for screaning & to test for H. pylori eradication following treatment, expensive.
2-Serology:-
Sensitive, specific & used for epidemiological surveys.
3- Endoscpic antral biopsy for
-Rapid Urease test (CLO)
-Culture & sensitivity (Gold standard investigations)
-Histological examination
H. pylori eradication therapy
P.P.I based triple therapy with two antibiotic
1-Omeprazole 20mg bid +
Metronidazole 400mg bid + Claithromycin 500mg bid for 7 days,
(90% effective) OR
2-Omeprazole 20mg bid + 400mg bid +Amoxil 1gm bid
for 7- 10 days (85- 90% effective) OR
3-Omeprazole 20mg bid + Amoxil 1gm bid + Claithromycin 250mg bid
for 7-10 days. (85%) effective
B) H2 RA based triple therapy
*Bisthmus is included in some regimens
GASTRITIS
Inflammatory disease involving superficial epithelium erosion + ulceration.
-In chronic active gastritis there is infiltration of lamina propria with lymphocytes & plasma
cells leading to atrophic gastritis & gastric atrophy with loss of parietal & chief cells &
subsequent metaplasia.
Autoimmune gastritis (type A GASTRITIS)
This is an autoimmune condition in which there are circulating antibodies to the parietal cell.
This results in the atrophy of the parietal cell mass, hence hypochlorhydria and ultimately
achlorhydria.
As intrinsic factor is also produced by the parietal cell there is malabsorption of vitamin B12,
which, if untreated, may result in pernicious anaemia.

This results in chronic hypergastrinaemia>>>>hypertrophy of the ECL cells in the body of
the stomach, which are not affected by the autoimmune damage>>>microadenomas
develop in the ECL cells>>>> identifiable tumour nodules.
H. pylori gastritis
Previously described as type B gastritis, this affects the antrum, and it is these patients who
are prone to peptic ulcer disease.
Helicobacter-associated pangastritis is also a very common manifestation of infection, but
gastritis affecting the corpus alone does not seem to be associated.
Patients with pangastritis seem to be most prone to the development of gastric cancer.
Intestinal metaplasia is associated with chronic pangastritis with atrophy.
Intestinal metaplasia associated with dysplasia has significant malignant potential and, if
this condition is identified, endoscopic screening may be appropriate.
Stress gastritis
This is a common sequel of serious illness or injury and is characterised by a reduction in
the blood supply to superficial mucosa of the stomach.
Prevention of the stress bleeding from the stomach is much easier than treating it, and
hence the routine use of H2 antagonists with or without barrier agents, such as sucralfate, in
patients who are on intensive care. These measures have been shown to reduce the
incidence of bleeding from stress ulceration.
Ménétrier’s disease
This is an unusual condition characterised by gross hypertrophy of the gastric mucosal
folds, mucus production and hypochlorhydria , premalignant and may present with
hypoproteinaemia and anaemia. There is no treatment other than a gastrectomy.
Lymphocytic gastritis
This type of gastritis is seen rarely. It is characterised by the infiltration of the gastric mucosa
by T cells and is probably associated with H. pylori infection. The pattern of inflammation
resembles that seen in coeliac disease or lymphocytic colitis.
Other forms of gastritis
Eosinophilic gastritis appears to have an allergic basis, and is
treated with steroids and cromoglycate. Granulomatous gastritis
is seen rarely in Crohn’s
disease and also may be associated with tuberculosis. Acquired immunodeficiency
syndrome
(AIDS) gastritis is secondary to infection with cryptospiridiosis.
Phlegmonous gastritis is a rare bacterial infection of the stomach found in patients with
severe intercurrent illness.
PEPTIC ULCER
Although
the name ‘peptic’ ulcer suggests an association with pepsin, this is essentially
unimportant as in the absence of acid, peptic ulcers do not occur. Nearly all peptic ulcers
can be healed by using proton pump inhibitors, which can render a patient virtually
achlorhydric.
Common sites for peptic ulcers are the first part of the duodenum and the lesser curve of
the stomach, but they also occur on the stoma following gastric surgery, the
oesophagus and even in a
Meckel’s diverticulum, which contains ectopic gastric
epithelium.
In general, the ulcer occurs at a junction between different types of epithelia, the ulcer
occurring in the epithelium least resistant to acid damage.
It is now widely accepted that infection with H. pylori and the consumption of NSAIDs are
the most important factors in the development of peptic ulceration.
Cigarette smoking predisposes to peptic ulceration and increases the relapse rate after
treatment,
Multiple other factors may be involved in transition between the superficial and the deep
penetrating chronic ulcer, but they are of lesser importance.
Duodenal ulceration
Most occur in the first part of the duodenum. A chronic ulcer penetrates the mucosa and into
the muscle coat, leading to fibrosis, the fibrosis causes deformities such as pyloric
stenosis.
Sometimes there may be more than one duodenal ulcer. The situation in which there is both
a posterior and an anterior duodenal ulcer is referred to as ‘kissing ulcers’.
Anteriorly placed ulcers tend to perforate and, in contrast,
posterior duodenal ulcers tend to bleed, sometimes by eroding into the gastroduodenal
artery.
Occasionally, the ulceration may be so extensive that the entir duodenal cap is ulcerated
and devoid of mucosa.
Malignancy in this region is so uncommon , In the stomach the situation is different .
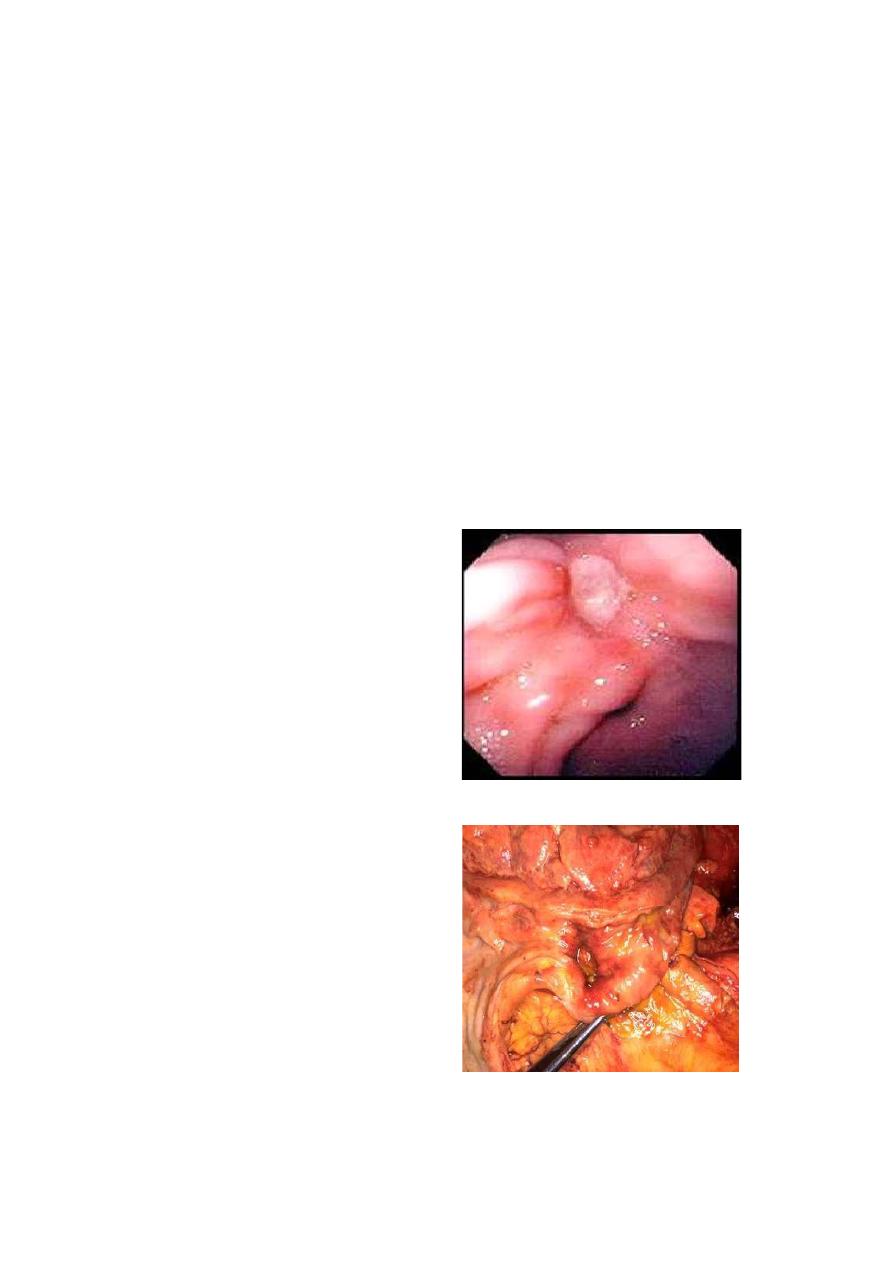
Peptic Ulcer
Size
– variable; 0.3 – 4 cm in
diameter
Shape - round to oval
Sharply demarcated, clean-cut,
punched-out area with clean base
Margins are usually level with
surrounding mucosa or slightly
elevated due to edema; the mucosa
is undermined at the edges
Radiating mucosal rugae
80% are solitary, 80% occur in the
duodenum, of which 90% in the
first part of the duodenum on the
anterior wall’ within a few
centimeter of the pyloric ring.
19% occur in the stomach(usually at
the lesser curvature at the border of
the body and antrum.
Gastric ulcers
As with duodenal ulceration, H. pylori and NSAIDs are the important aetiological factors.
Gastric ulceration is also associated with smoking; other factors are of lesser importance.
Gastric ulceration is substantially less common than duodenal ulceration. The sex incidence
is equal and the population with gastric ulcers tends to be older. It is more prevalent in low
socioeconomic groups. It is essentially similar to that of a duodenal ulcer, except
that gastric ulcers tend to be larger.
Fibrosis, when it occurs, may result in the now rarely seen hourglass contraction of the
stomach. Large chronic ulcers may erode posteriorly into the pancreas and, on other
occasions, into major vessels such as the splenic artery. Less commonly, they may erode
into other organs such as the transverse colon.
Chronic gastric ulcers are much more common on the lesser curve (especially at the
incisura angularis; than on the greater curve and, even when high on the lesser curve, they
tend to be at the boundary between the acid-secreting and the non-acid-secreting epithelia.
Classified in 4 groups according anatomical location:
Type I: lesser curvature
Type II: arise same place as duodenal ulcers/ combination of both
Type III: pre-pyloric region
Type IV: high in lesser curvature
*Type I are the most common ones (lesser curvature) and type IV
less common ones both are associated with low acidity.
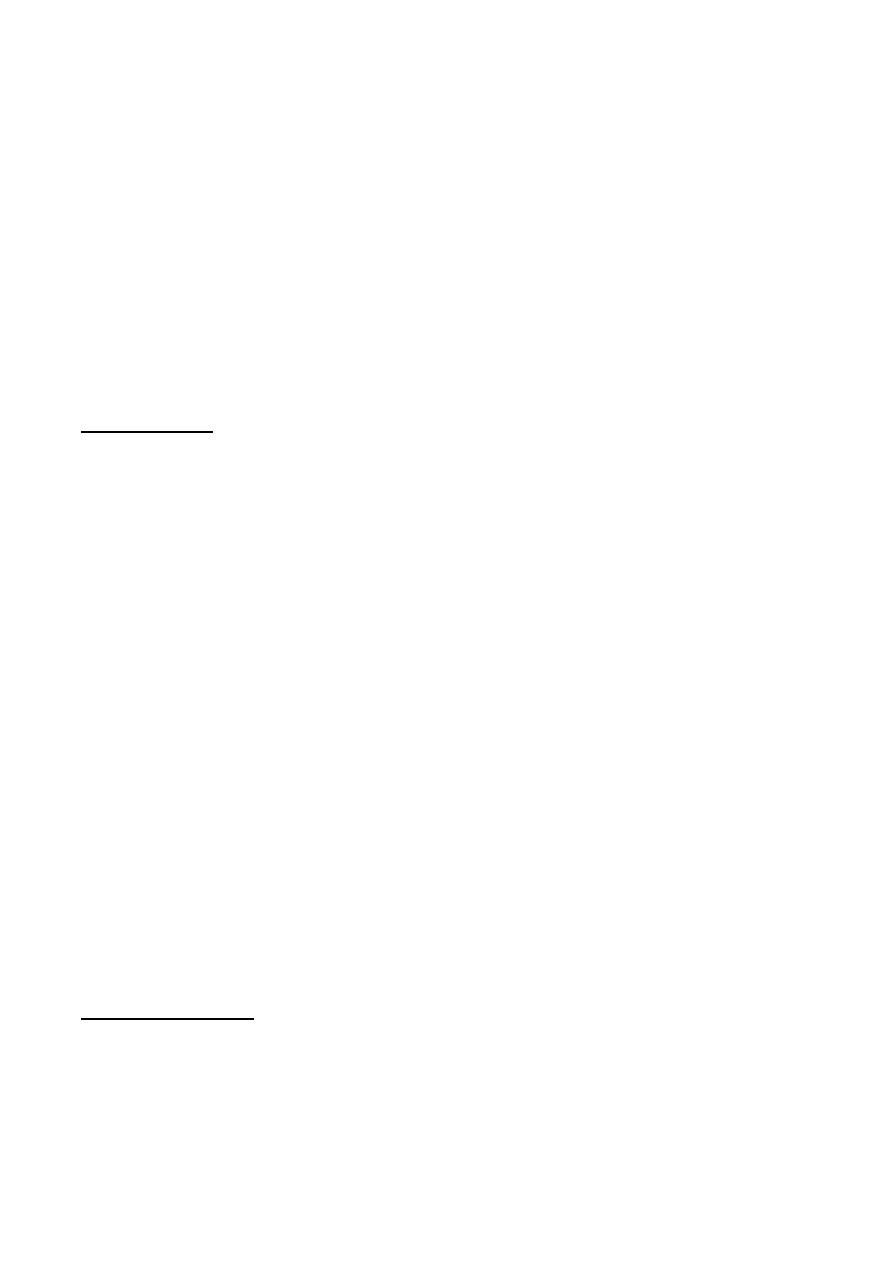
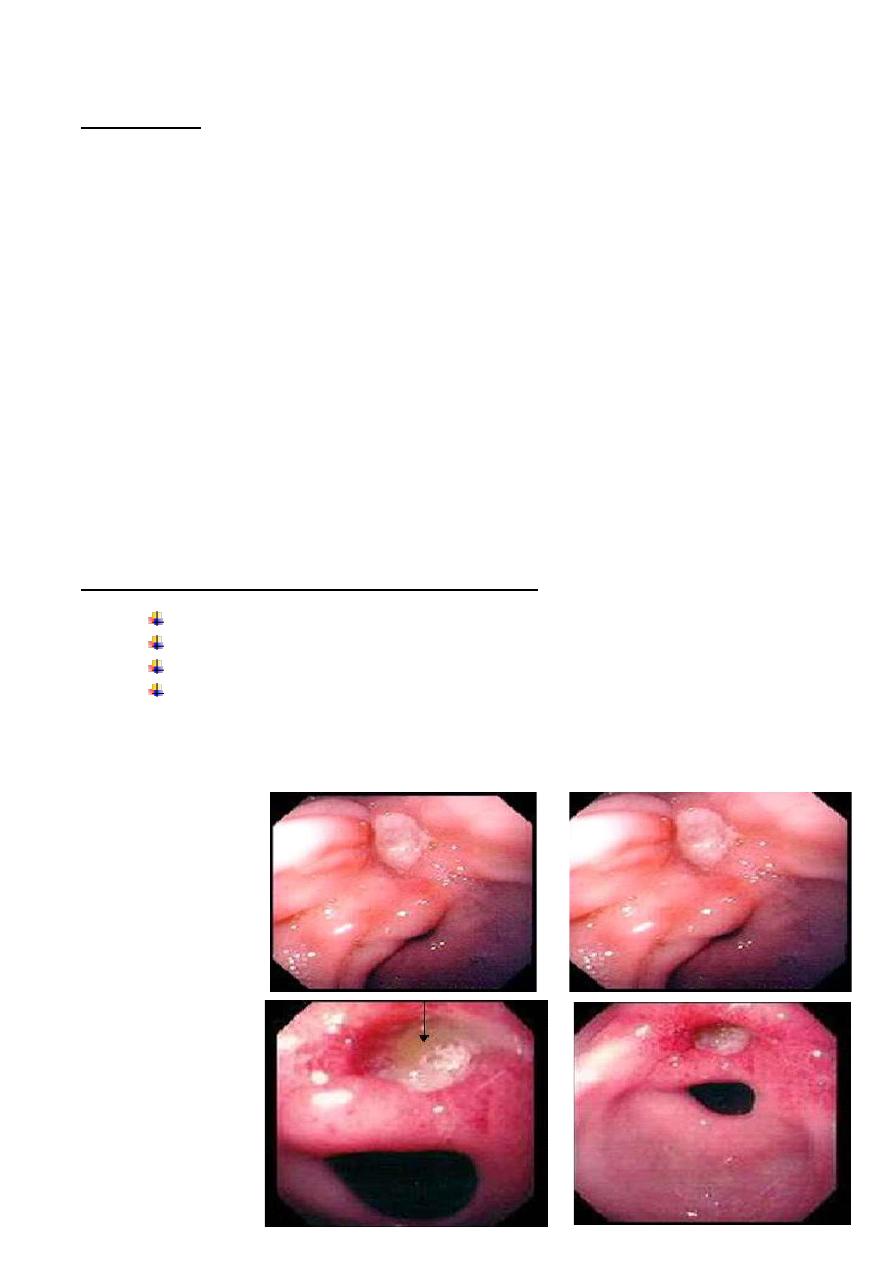
Gastric
Ulcer-
Endoscopic
Appearance
Malignancy in gastric ulcers
Chronic duodenal ulcers are not associated with malignancy and, in contrast, gastric ulcers
are.
Two clinical extremes must be distinguished to understand this problem properly.
*First, there is the situation in which a benign chronic gastric ulcer undergoes malignant
transformation ,this is known to happen, albeit rarely.
* The contrasting clinical extreme is the patient identified as having an ulcer in the stomach,
either endoscopically or on contrast radiology,
which is assessed as benign but biopsies reveal malignancy,(has presented with an
ulcerated cancer).
*It is fundamental that any gastric ulcer should be regarded as being malignant, no matter
how classical the features of a benign gastric ulcer. *Multiple biopsies should always be
taken, perhaps as many as 10 well-targeted biopsies, before an ulcer can be tentatively
accepted as being benign.
Modern antisecretory agents can frequently heal the ulceration associated with gastric
cancer but, clearly, are ineffective in treating the malignancy itself.
If, at operation for perforation, it is determined that the ulcer is probably benign it should,
nonetheless, be excised, in totality if possible, and submitted for histological examination.
Other peptic ulcers
The pre-pyloric gastric ulcer was in the past difficult to treat, a problem overcome with the
introduction of proton pump inhibitors.
Pyloric channel ulcers are similar to duodenal ulcers.
Both pre-pyloric and pyloric ulcers may be malignant, biopsy is essential.
Stomal ulcers occur after a gastroenterostomy (now most commonly after bariatric surgery)
or a gastrectomy of the Billroth II type. The ulcer is usually found on the jejunal side of the
stoma.
Clinical features of peptic ulcers
Pain The pain is epigastric, often described as gnawing and may radiate to the back.
Eating may sometimes relieve the discomfort.
Periodicity One of the classical features of untreated peptic ulceration is periodicity.
Symptoms may disappear for weeks or months to return again. This periodicity may be
related to the spontaneous healing of the ulcer.
Vomiting (stenosis has occurred ?).
Alteration in weight Weight loss or, sometimes, weight gain may occur. Patients with
gastric ulceration are often underweight but this may precede the occurrence of the ulcer.
Bleeding All peptic ulcers may bleed. The bleeding may be chronic and presentation with
microcytic anaemia is not uncommon. All such patients should be investigated with
endoscopy. Acute presentation with haematemesis and melaena .
Examination of the patient may reveal epigastric tenderness.
Investigation of the patient with suspected peptic ulcer
• Gastroduodenoscopy
This is the investigation of choice in the management of suspected
peptic ulceration.
In the stomach, any abnormal lesion should be multiply biopsied, and in the case of a
suspected benign gastric ulcer numerous biopsies must be taken in order to exclude, as far
as possible, the presence of a malignancy. Commonly, biopsies of the antrum will be taken
to see whether there is histological evidence of gastritis and a CLO test performed to
determine the presence of H. pylori.
A ‘U’ manoeuvre should be performed to exclude ulcers around the gastro-oesophageal
junction. This is important as the increasing incidence of cancer at the gastro-oesophageal
junction requires that all mucosal abnormalities in this region should undergo multiple
biopsy.
If a stoma is present, it is important to enter both afferent and efferent loops. Attention
should be given to the pylorus to note whether there is any pre-pyloric or pyloric channel
ulceration, and also whether it is deformed, which is often the case with chronic duodenal
ulceration.
In the duodenum, care must be taken to view all of the first part. It is not infrequent for an
ulcer to be just beyond the pylorus and easily overlooked.
Treatment of peptic ulceration
The vast majority of uncomplicated peptic ulcers are treated medically. Surgical treatment of
uncomplicated peptic ulceration has decreased markedly. Surgical treatment was aimed
principally at reducing gastric acid secretion and, in the case of gastric ulceration, removing
the diseased mucosa. When originally devised, medical treatment also
aimed to reduce gastric acid secretion, initially using the highly successful H2-receptor
antagonist and, subsequently, proton pump inhibitors. This has now largely given way to
eradication therapy.
Medical treatment
It is reasonable that a doctor managing a patient with an uncomplicated peptic ulcer should
suggest m
odifications to the patient’s lifestyle, particularly the cessation of cigarette
smoking.
H2-receptor antagonists and proton pump inhibitors
H2-antagonists (Black) revolutionised the management of peptic ulceration. Most duodenal
ulcers and gastric ulcers can be healed by a few weeks of treatment with these drugs.
There remained,however, a group of patients who were relatively refractory to conventional
doses of H2-receptor antagonists. This is largely now irrelevant as proton pump inhibitors
can effectively render
a patient achlorhydric and all benign ulcers will heal using these drugs, the majority within 2
weeks. Symptom relief is impressively rapid, most patients being asymptomatic within a few
days.
Like H2-antagonists, proton pump inhibitors are safe and relatively devoid of serious side
effects. The problem with all gastric antisecretory agents is that following cessation of
therapy relapse is almost universal.
Eradication therapy
Eradication therapy is now routinely given to patients with peptic ulceration, and H. pylori
infection .
There are some patients with peptic ulcers in whom eradication
therapy may not be appropriate and this includes patients with NSAID-associated ulcers.
Such patients should avoid these drugs if possible and, if not, they should be coprescribed
with a potent antisecretory agent.
Similarly, patients with stomal ulceration are not effectively treated with eradication therapy
and require prolonged prescription
of antisecretory agents.
Patients with Zollinger
–Ellison syndrome should be treated in the long term with proton
pump inhibitors unless the tumour can be adequately managed by surgery.
Ulcers that fail to heal
Despite these advances peptic ulceration fails to heal in a small minority of patients.
Endoscopic re-evaluation should be regarded as mandatory to confirm healing of all gastric
ulcers. The most common cause of failed healing is persistent H. pylori infection. Biopsies
should be repeated at the time of endoscopy as false-negative results with breath tests may
be expected soon after eradication therapy .
The ingestion of NSAIDs should once again be addressed.
A diagnosis of Zollinger-Ellison syndrome ,should be suspected in H. pylori negative, non-
NSAID-related peptic ulcerationand serum gastrin levels should be measured.
Very rarely, a recently described autoimmune IgG4-related phenomenon is the cause of
resistant and recurrent gastric ulceration.
Surgical treatment of uncomplicated
peptic ulceration
the incidence of surgery for uncomplicated peptic ulceration has fallen markedly, to the
extent that peptic ulcer surgery is now of little more than historical interest.
A description of operations used in the treatment of peptic ulcers is still necessary because
surgery is occasionally employed for the complicated ulcer and, in addition, many patients
are left suffering from the consequences of the more destructive operations
Operations for duodenal ulceration Duodenal ulcer surgery (rationale)
This has been achieved by diversion of the acid away from the duodenum, reducing the
secretory potential of the stomach, or both.
There is now no role for acid-reducing operations in the routin management of peptic ulcer
disease but occasionally operations which involve gastrectomy have to be performed in the
emergency situation.
The operations are described in historical sequence.
Billroth II gastrectomy
The original Billroth operations consisted of a gastric resection with gastroduodenal
anastomosis (Billroth I technique), It soon became evident that the use of gastrojejunal
anastomosis after gastric resection could be safer and easier than the Billroth I procedure,
and it became popular and effective in the surgical treatment of duodenal ulcer. its
disadvantages, such as higher operative mortality and morbidity, it has not been used for
many years in the patient with an uncomplicated ulcer.
Gastrojejunostomy
Because of the potential for mortality after gastrectomy, the use of gastrojejunostomy alone
in the treatment of duodenal ulceration was developed , stomal ulceration was extremely
common, hence the
procedure in isolation was ineffective.
Truncal vagotomy and drainage
Truncal vagotomy was combined with drainage, was the mainstay
of treatment of duodenal ulceration .The principle of the operation is that section of the
vagus nerves, which are critically involved in the secretion of gastric acid, Because the vagal
nerves are motor to the stomach, denervation of the antropyloroduodenal segment results in
gastric stasis . The most popular drainage procedure is the Heineke
–Mikulicz
pyloroplasty.
Highly selective vagotomy in which only the parietal cell mass of the stomach was
denervated. This operation became the gold standard for operations on duodenal ulceration
in the 1970s.
Truncal vagotomy and antrectomy
In addition to a truncal vagotomy, the antrum of the stomach is removed, thus removing the
source of gastrin, and the gastric remnant is joined to the duodenum.
Operations for gastric ulcer
In contrast with duodenal ulcer surgery, when the principal objective was to reduce
duodenal acid exposure, in gastric ulceration the diseased tissue is usually removed as well.
Billroth I gastrectomy This was the standard operation for gastric
ulceration until medical treatments became prevalent.
Sequelae of peptic ulcer surgery
Recurrent ulceration
Small stomach syndrome early satiety follows most ulcer operations , there is loss of
receptive relaxation .
Bile vomiting can occur after any form of vagotomy with drainage or gastrectomy.
Following gastrectomy, Roux-en-Y diversion is probably
the best treatment.
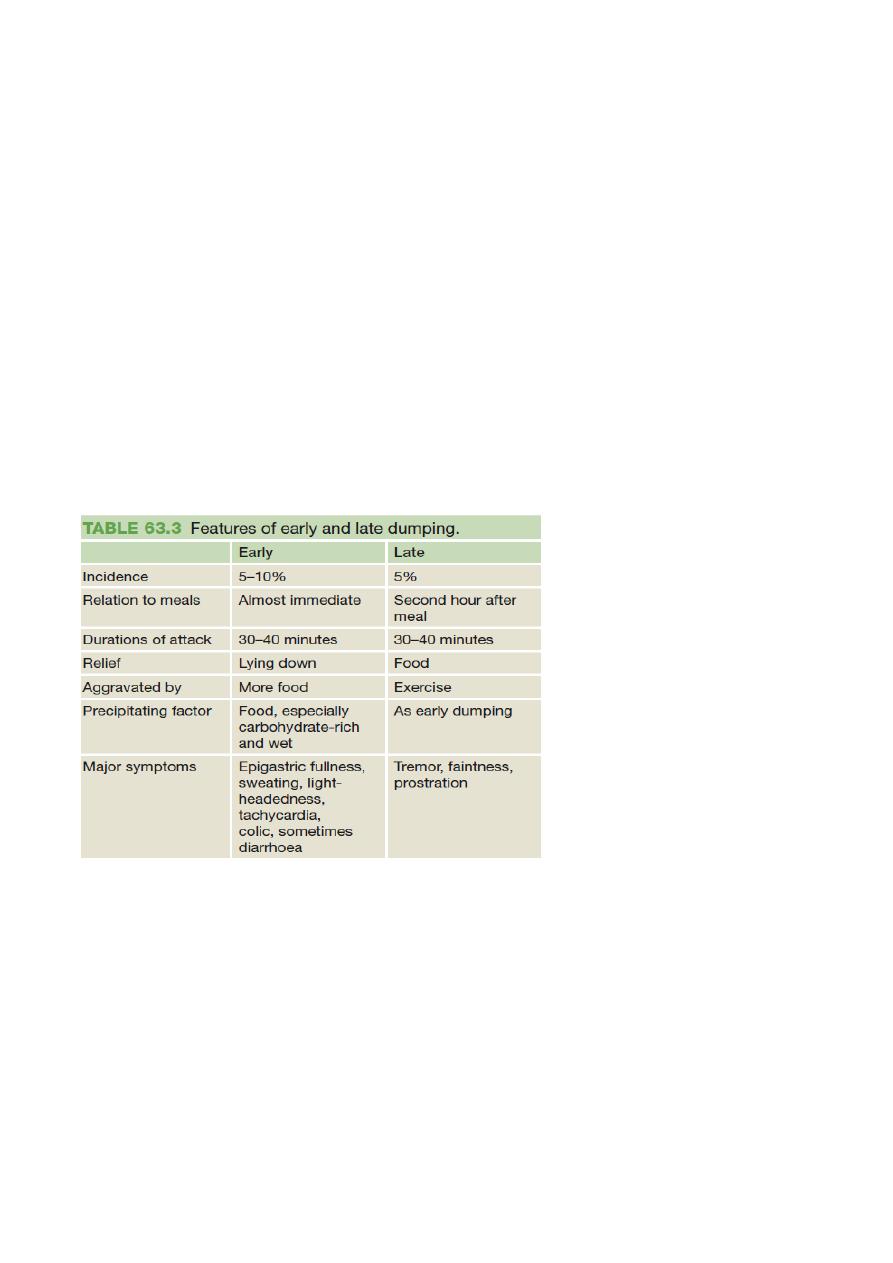
EARLY DUMPING consists of abdominal and vasomotor symptoms
that are found in about 10% of patients following gastrectomy or vagotomy and drainage.
The small bowel is filled with foodstuffs from the stomach, which have a high osmotic load,
and this leads to the sequestration of fluid from the circulation into the gastrointestinal tract.
This can be observed by the rise in the packed cell volume
LATE DUMPING is reactive hypoglycaemia. The carbohydrate load in the
small bowel causes a rise in the plasma glucose, which, in turn, causes insulin levels to rise,
causing a secondary hypoglycaemia.
Post-vagotomy diarrhoea in about 5%, it may be intractable. It is related, to some degree,
to rapid gastric emptying.
Malignant transformation
Many large studies now confirm that operations such as gastrectomy
or vagotomy and drainage are independent risk factors for the development of gastric
cancer.

Nutritional consequences are more common after gastrectomy than after vagotomy and
drainage. Weight loss is common after gastrectomy and the patient may, in fact, never
return to their original weight. Iron-deficiency anaemia, Vitamin B12 deficiency, Bone
disease is essentially indistinguishable from the osteoporosis commonly seen in post
menopausal women.
Gallstones following truncal vagotomy, the biliary tree, as well as the stomach, is
denervated, leading to stasis and hence stone formation .
D.H