1
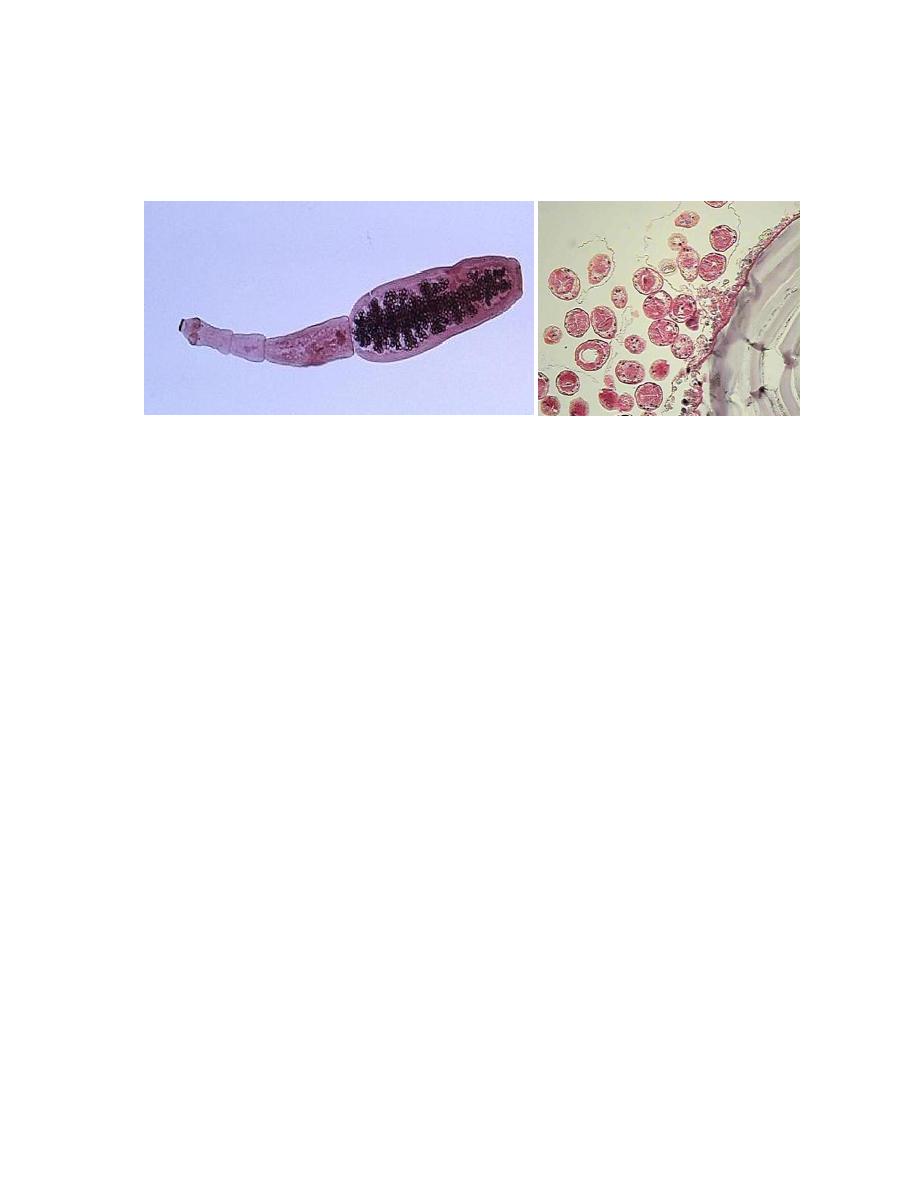
Echinococcus granulosus
Adult worm protoscolices
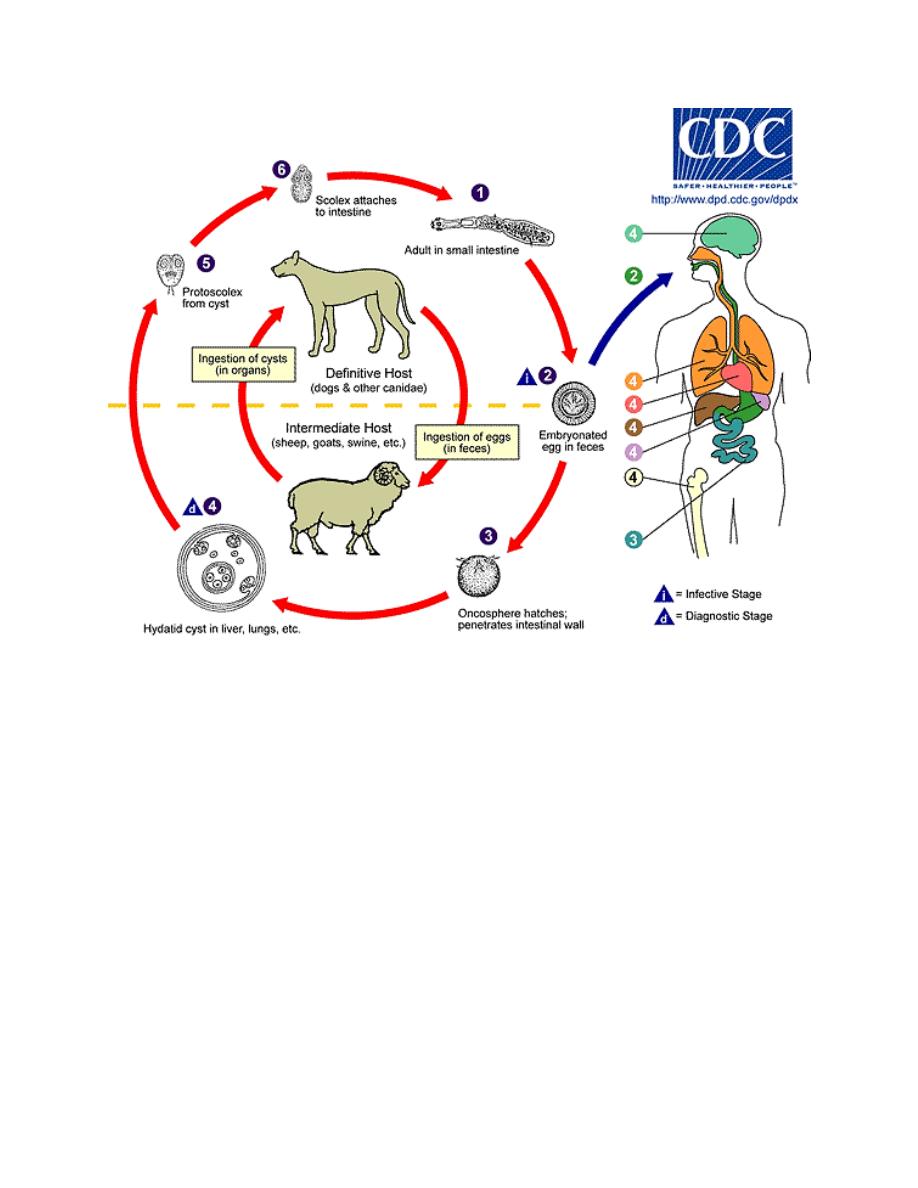
Morphology, Biology and Life Cycle
The adult of E.granulosus lives in the small intestine of the canine host, with its
“head” embeded between the villi. The worm measures 3 to 6 mm long.
When ripe eggs are swallowed by man, they hatch in the intestine and the freed
embryos migrate through blood and lymphatic channels to the liver and less
frequently to other viscera. Here they develop rather slowly into vaculated
unilocular hydatids, characterized by an external, milky white laminated
membrane and an internal germinative layer typically producing multiple scolices,
each capable of developing into daughter hydatids within the parent cyst. Usually
the cyst has a host-tissue capsule.
2
Pathogenesis and Symptomatology
A majority of human hydatids develop in liver, after the hexacanth embryos have
burrowed into the intestinal wall and gotten into the mesenteric venules, infection
of the lungs is next in prevalence; if they pass the pulmonary filter the embryos
may settle down in any organ or tissue including bone, and proceed to develop into
hydatids.
In heavily endemic areas in South America, the pulmonary location is more
frequent than the hepatic. The primary hydatid cyst is usually single, but they may
be multiple.
Types of Hydatids produced by E.granulosus: There are two morphological
types in human tissues, Viz., unilocular and osseous. The unilocular cyst has a
central, fluid-filled cavity lined with a germinative layer, surrounded by an intact
but a friable laminated membrane covered with a host-tissue capsule. A majority of
human hydatids are unilocular, but if the embryo is filtered out of blood vessels in
bony tissues, no limiting membranes are produced and the organism proceeds to

3
grow as a protoplasmic stream which erodes the cancellous structure, particularly
of long bones and pelvic arch (osseous hydatid).
The size and contour of the unilocular hydatid are depended on the site of
implantation and on its age. It may be 15 cm or more in diameter, containing a liter
or more of clear, sterile hydatid fluid, typically with numerous scolices and
daughter hydatids.
The amount of systemic intoxication or sensitization resulting from a unilocular
hydatid depends on how well it is insulated from the surrounding host tissues. If a
large abdominal cyst bursts, either spontaneously or following a blow on the
abdomen, anaphylaxis may be precipitated by the sudden liberation of hydatid
fluid into the peritoneal cavity. Moreover, scolices spilled out of the cystic cavity
will become implanted on the peritoneum and produce multiple secondary
growths. Rupture of a pulmonary cyst into a bronchus results in coughing up the
contents, with a possible spontaneous clearance of the infection. Hydatid of the
brain produces increasing symptomatic evidence of an intracranial tumor. Osseous
hydatid is insidious, gradually eroding the bone to a stage where fracture or
crumbling suddenly occurs.
Rupture of Hydatid Cyst
Rupture of hydatid cyst may occur naturally, or in process of obtaining a biopsy for
microscopic examination, due to coughing, muscle strain or surgical procedures.
Such patients may suffer from anaphylactic shock, eosinophilia and allergic
reactions or even death. The escape cyst fluid with protoscolices has the capacity
of spreading to other sites and forming a new cyst (secondary hydatidosis).
Rupture of the cyst is most important than the mass effect of the cyst, except in the
brain where the mass effect has severe consequences.
Diagnosis
In endemic areas, experienced clinicians may obtain strong suspicion of hydatid
disease from the patient's history, presenting symptoms and X-ray
picture. Noninvasive imaging techniques such as CT scans, MRI, and ultrasound
imaging are all used for detecting and defining the extent and condition of
avascular fluid-filled cysts in most organs. These techniques have proved valuable
for diagnosis and preoperative evaluation by staging the condition of the lesion. A
specific diagnosis can be obtained by intradermal test, employing a known amount
of hydatid antigen.. Serologic tests, such as enzyme-linked immunosorbent assay
(ELISA) and indirect hemagglutination test, are highly sensitive methods for
detecting infection. Final diagnosis consists in demonstration of free scolices or

4
daughter cysts from aspirated hydatid fluid, or of the histologic structure of the
cyst wall, with its laminated membrane.
Treatment
Echinococcosis (hydatid disease) is often expensive and complicated to treat,
sometimes requiring extensive surgery and/or prolonged drug therapy. There are
3 options for the treatment of cystic echinococcosis:
1- Percutaneous treatment of the hydatid cysts with the PAIR (Puncture,
Aspiration, Injection of protoscolicidal chemicals, Re-aspiration)
technique; This option is indicated for patients with relapse after surgery,
failure of chemotherapy alone, or who refuse surgery.
2- Surgery
3- Anti-infective drug treatment
The choice must primarily be based on the ultrasound images of the cyst,
following a stage-specific approach, and also on the medical infrastructure and
human resources available.
For some patients, chemotherapy with benzimidazoles is the preferred treatment.
Patients with small cysts or multiple cysts in several organs can be treated
successfully with albendazole. Approximately one third of patients treated with
chemotherapy with benzimidazole drugs have been cured of the disease and
even higher proportions, between 30-50%, have responded with significant
regression of the cyst size and alleviation of symptoms.
Epidemiology
Human infection with the hydatid cyst of E.granulosus is apt to occur where dogs
harbor the adult worms and sheep or hogs serve as common reservoirs of larval
stage. Exposure most commonly takes place in childhood, particularly among boys
who play with infected dogs.
Control
Control must be directed against the dog, the carrier of the adult Echinococcus
granulosus, and sheep and hogs, the common reservoirs of the viable hydatid, all
infected carcasses should be deeply buried. Stray dogs should be destroyed.
Domestic dogs should be periodically de-wormed. Personal hygiene in endemic
areas includes care to avoid contamination of food and drink with the feces of
dogs.