
1
Enterobius vermicularis (Pinworm)
The pinworm of man, Enterobius vermicularis (Linnaeus, 1758) Leach, 1853, has
been known since ancient times. It has a cosmopolitan distribution, but it is more
common in persons living in a cool temperate zones than in strictly tropical areas.
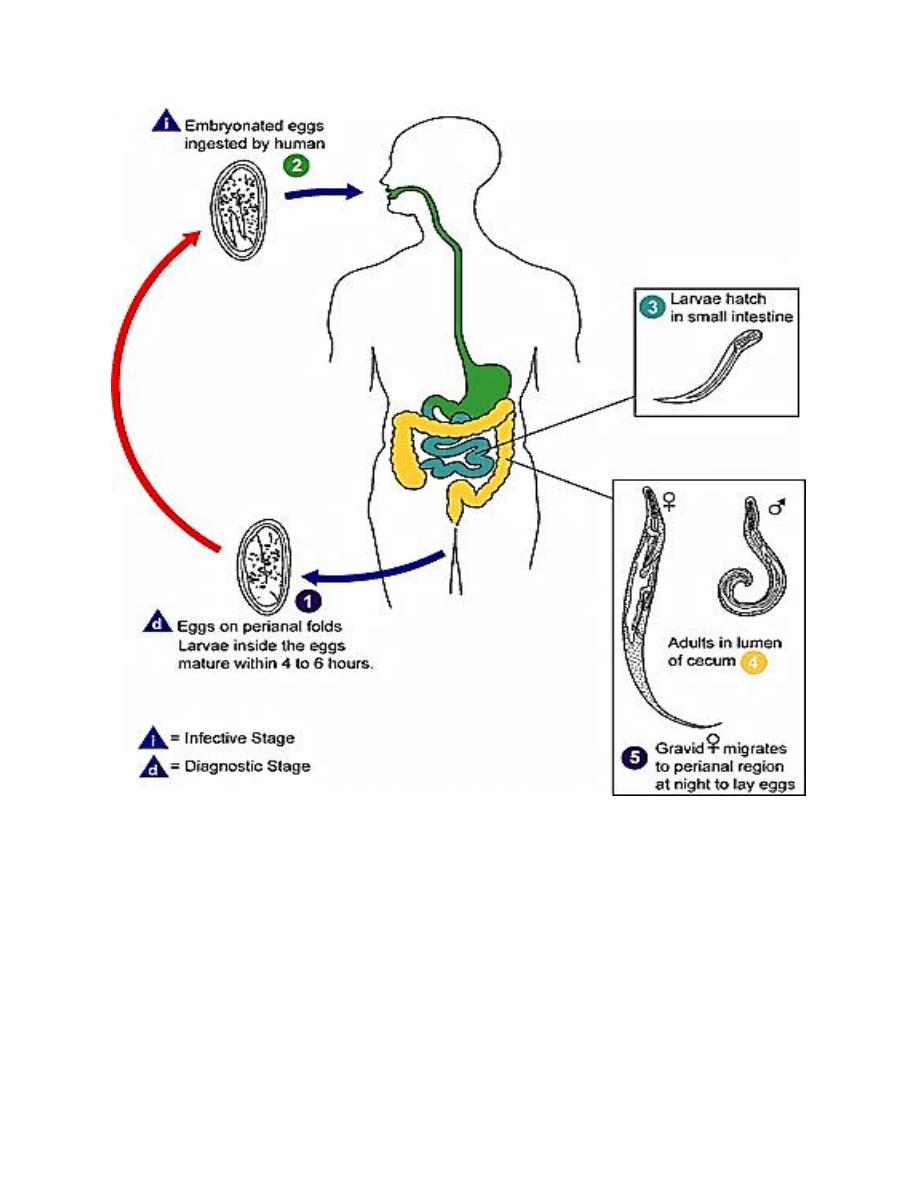
Morphology, Biology and Life Cycle
The adult male worm of E. vermicularis measures up to 5 mm long and has a
maximum width of 0.1 to 0.2 mm with its strongly curved posterior end, the lateral
view of the worm forms an inverted question mark. The female worm is
considerably larger than the male, having a length of up to 13 mm and a maximum
width of 0.3 to 0.5 mm.
The characteristic habitat of these worms is the cecum and appendix. Gravid
female migrate down the bowel and out of the anus onto the perianal and perineal
skin; in female subjects they may reach the vulva and wander up the genital tract.
Eggs in utero are not fully embryonated when the female worms migrate to the

2
lower levels of the colon. Eggs laid within the bowel are relatively immature. Each
female discharges about 10000 eggs.
The eggs discharged on the skin are essentially mature and within a few hours
contain a fully developed infective-stage larva. The eggs are flattened on one side,
measure 50 to 60 by 20 to 30 microns, and have an outer albuminous layer which
causes them to stick to each other and to clothing and other subjects. Thus, some of
the eggs almost invariably are swallowed by persons in the contaminated
environment. When swallowed the eggs hatch and the larva, which measure 140 to
150 by 10 microns, mature in the cecal area, and complete the life cycle in 15 to 28
days.
Pathogenesis and Symptomatology
Commonly the first recognizable symptom is pruritus as the worms emerge from
the rectum and crawl over the perianal and perineal skin. Itching is followed by
scratching with adds to the irritation, with scarification or weeping eczema of the
areas, allowing bacteria to enter the lesion. As worm in various stages of
development frequently are seen in the appendix, and occasionally are found deep
in the inflamed mucosa, pinworms often are suspected of causing appendicitis.
Infection of the female genital tract has been well reported. At times worms enter
the female genital tract and become encapsulated within the uterus or fallopian
tubules, or wander into the peritoneal cavity and become encapsulated on the
peritoneum.
The common symptoms in children, in addition to pruritus, consist of restless
sleep, and tiredness during the daytime. Often the patient will complain insomnia
due to disturbed sleep, or even abdominal pain or appendicitis.
The blood picture in pinworm infection is not remarkably altered. There may be
low-grade eosinophilia.
Diagnosis
The specific diagnosis may be made on the recovery of the worms from the
perianal area, more frequently on demonstration of the eggs. Only occasionally are
eggs found in the feces.

3
Treatment
The medications used for the treatment of pinworm are either Mebendazole, or
Albendazole. Any of these drugs are given in one dose initially, and then another
single dose of the same drug two weeks later. The medication does not reliably kill
pinworm eggs. Therefore, the second dose is to prevent re-infection by adult
worms that hatch from any eggs not killed by the first treatment. Patients and
parents must be made aware of the probability of recurrent infection, which should
not be regarded as a treatment failure.
Repeated infections should be treated by the same method as the first infection. In
households where more than one member is infected or where repeated,
symptomatic infections occur, it is recommended that all household members be
treated at the same time. In institutions, mass and simultaneous treatment, repeated
in 2 weeks, can be effective (CDC).
4