1
Community Medicine / Fourth Stage / Dr. Ali
Leishmaniasis
◼ Leishmaniasis is a vector-borne disease that is transmitted by sand flies and caused by
obligate intracellular protozoa of the genus Leishmania
◼ Human infection is caused by about 21 of 30 species that infect mammals.
Mode of transmission
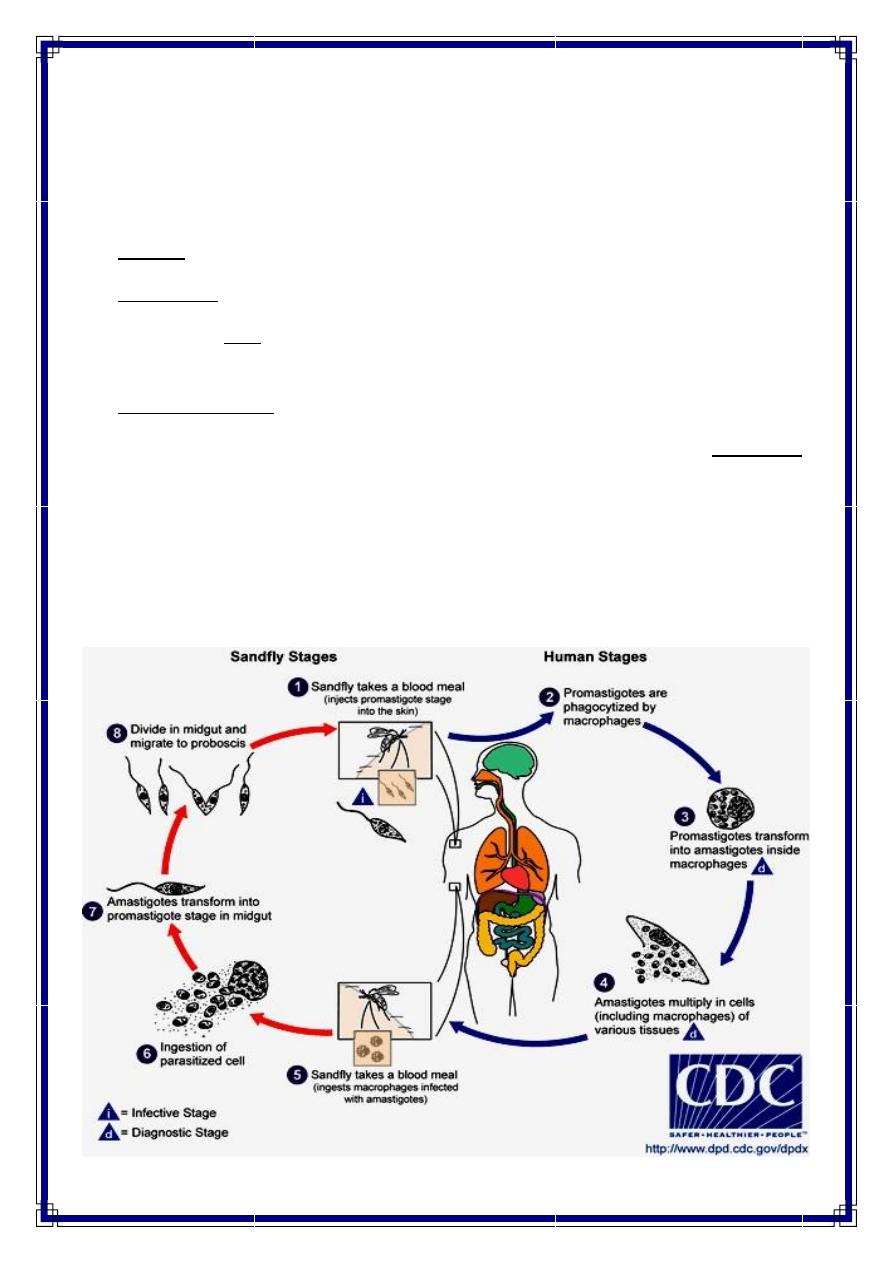
◼ Leishmaniasis is transmitted by the bite of infected female phlebotomine sand flies
◼ The sand flies inject the infective stage (promastigotes) during blood meals.
Distribution
◼ Age distribution:
A fatal type of visceral leishmaniasis, which is found along the Mediterranean, specifically
affects infants.
Although occurrence is proportional to sand fly exposure, children younger than 15 years
represent a large proportion of cases in endemic areas.
- Untreated visceral leishmaniasis in a pregnant mother can also have consequences on the
fetus or result in congenital visceral leishmaniasis.
- Certain types of visceral leishmaniasis affect certain pediatric age groups more than others
(eg, visceral leishmaniasis in the Mediterranean Basin caused by Leishmania infantum mainly
affects children aged 1-4 y).
◼ Sex distribution
Males are more commonly infected than females, most likely because of their increased
exposure to sand flies.
Visceral leishmaniasis, in particular, has been shown to be twice as common in males
than in females.
◼ Geographic Distribution:
Leishmaniasis is found in parts of about 88 countries.
Most of the affected countries are in the tropics and subtropics.
The settings in which leishmaniasis is found range from rain forests in Central and South
America to deserts in West Asia.
2
- More than 90 percent of the world's cases of visceral leishmaniasis are in India, Bangladesh,
Nepal, Sudan, and Brazil.
- Australia and the South Pacific are not considered regions where leishmaniasis is present as an
endemic illness.
- In the Middle East L. major and L. tropica are the most common species
Types of leishmaniasis
There are several ways to classify leishmaniasis (e.g. by geography or taxonomy ) are
available.
◼ Clinically, it can present itself in various ways, and is more easily classified as:
1. Cutaneous
2. Mucocutaneous
3. Visceral leishmaniasis
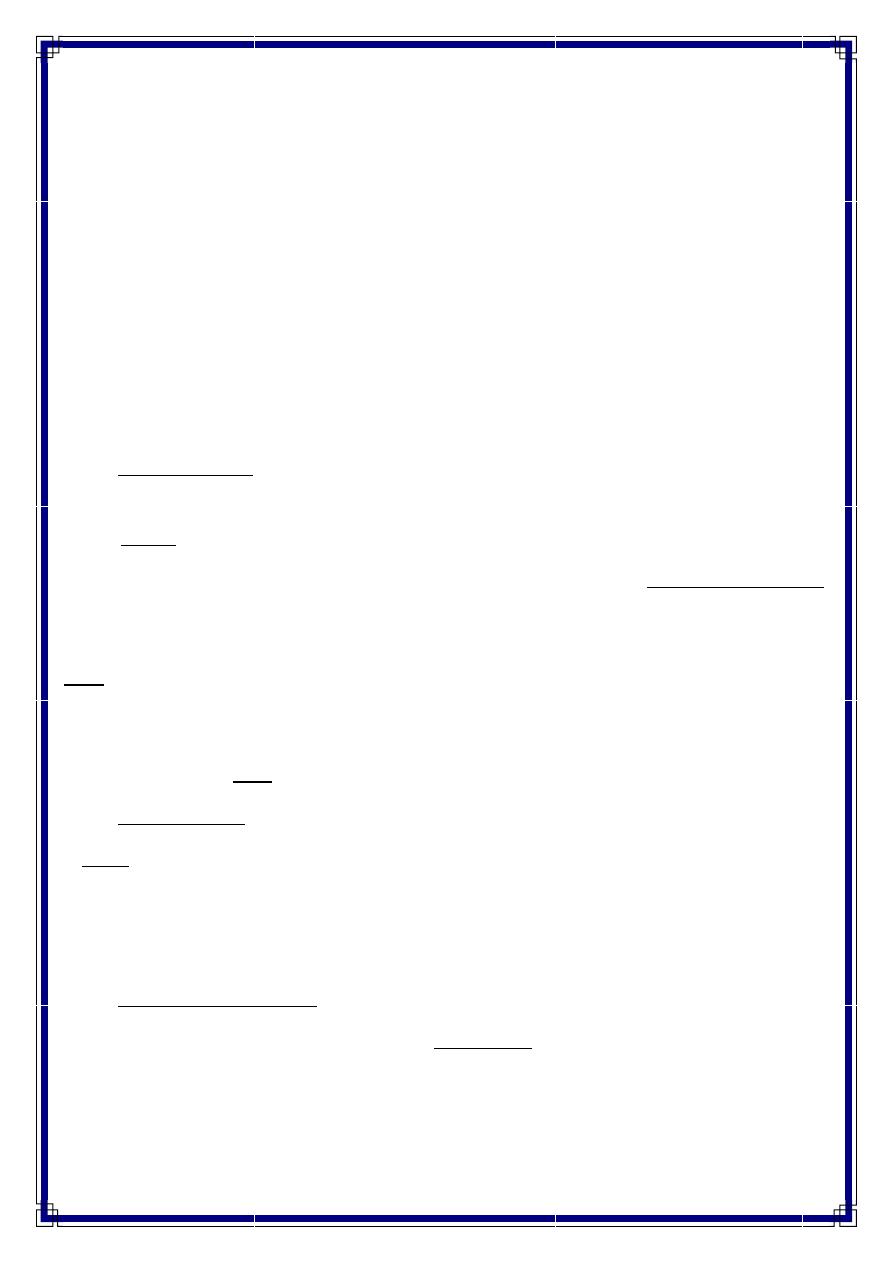
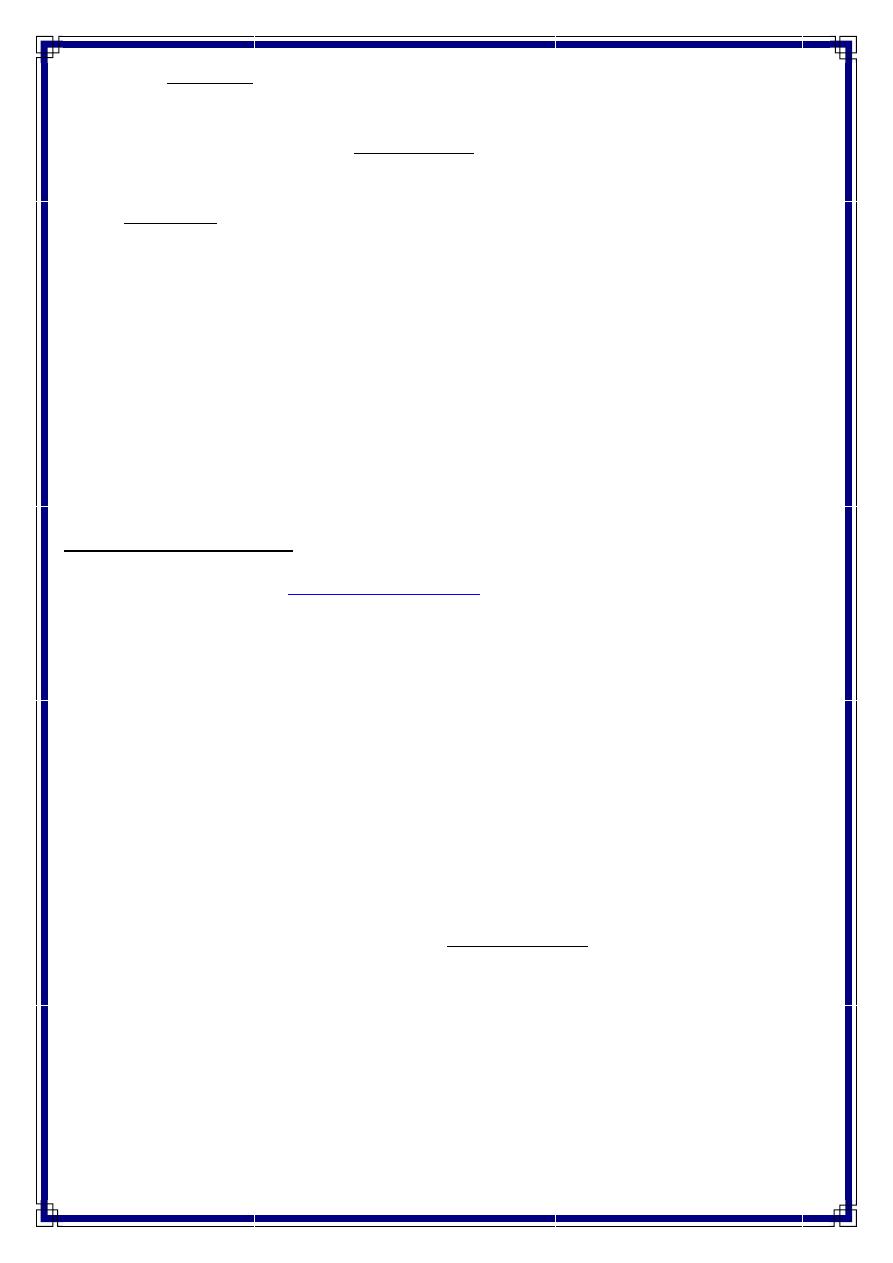
Cutaneous leishmaniasis
◼ The typical lesions of
were described as early as 900 BC and have
been referred to as:
➢ the "Balkan sore" in the Balkans,
➢ the "Delhi boil" in India,
➢ the "Baghdad boil" in Iraq, and
➢ “Saldana" in Afghanistan.
◼ Cutaneous leishmaniasis can be simple or diffuse.
◼ Different species, as well as host factors, can also affect the clinical picture, where some
species cause "wet" ulcers and others "dry" ulcers.
◼ After the bite of an infective sand fly, the incubation period is usually several weeks after
inoculation, but this incubation period is variable.
◼ Initial lesions can appear immediately after a bite, or the incubation period may last for
several months.
◼ These lesions are usually painless.
◼ Skin trauma can result in activation of seemingly latent cutaneous infection long after the
initial bite.
3
◼ Over a period of weeks to years, some lesions may resolve spontaneously without
treatment.
◼ Characterized by one or more sores, papules, or nodules on the skin.
◼ Often described as looking somewhat like a volcano with a raised edge and central crater
◼ Sores are usually painless but can become painful if secondarily infected
◼ Sores can heal & may leave significant scars and be disfiguring if they occur on the face
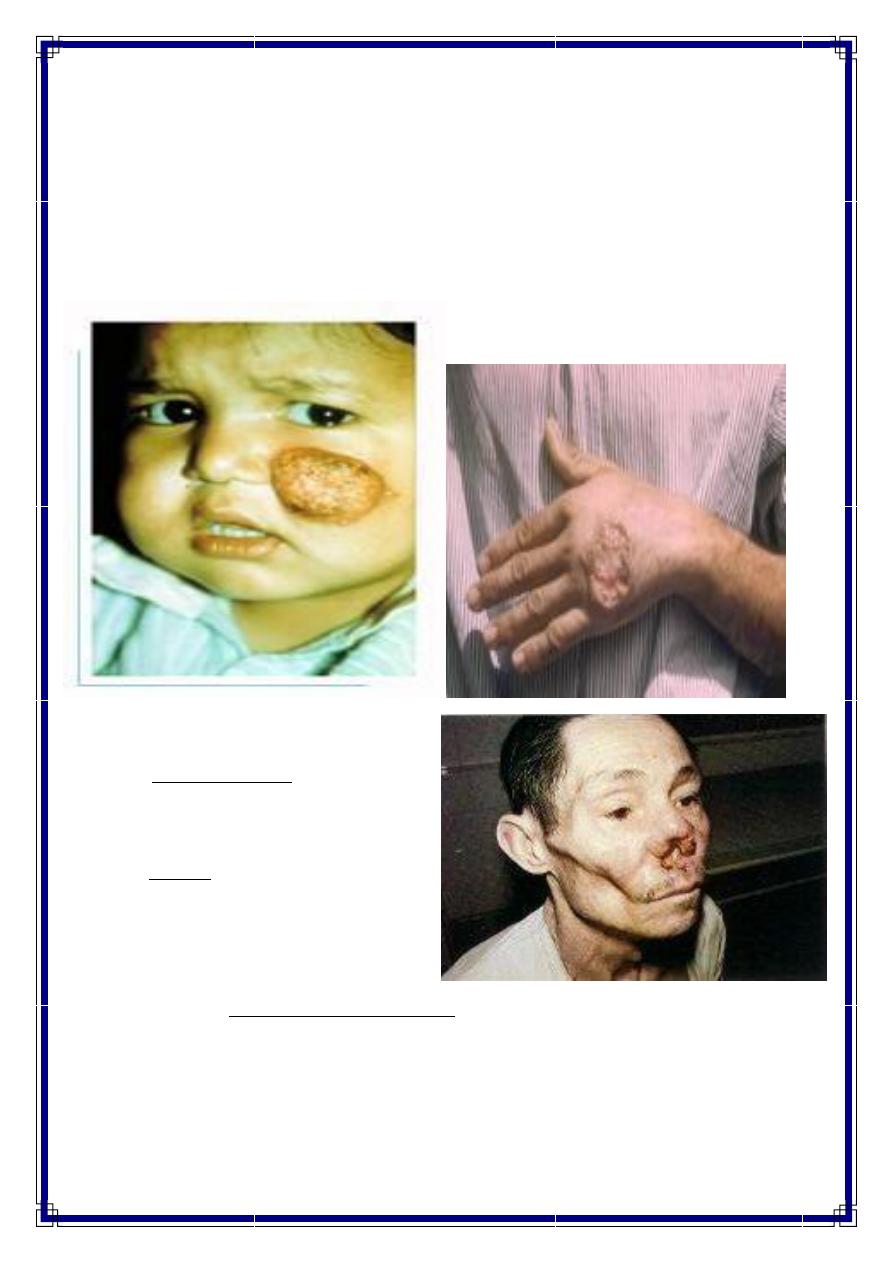
Mucocutaneous leishmaniasis
◼ The incubation period is from 1-3
months.
◼ Mucocutaneous leishmaniasis can be
the primary manifestation of the
disease, but the primary lesions may
also be limited to cutaneous
manifestations, with mucosal lesions
appearing only later in the course of
disease when untreated cutaneous lesions progress to involve the oral and nasal
surfaces.
◼ Initial symptoms related to mucosal lesions may include nasal obstruction and bleeding.
◼ Mucosal lesions become painful gradually and can become sites of infection, sometimes
leading to sepsis.
4
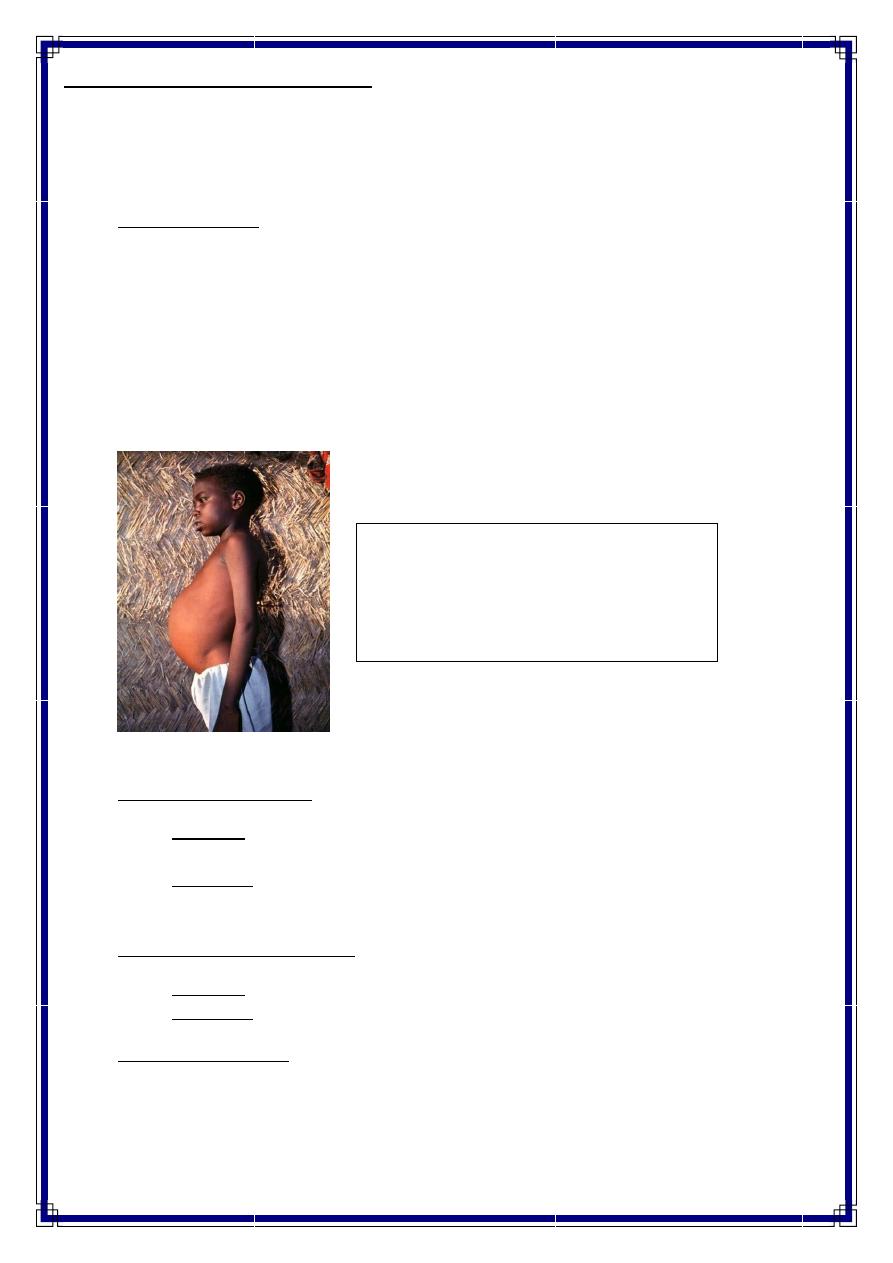
Profile view of a teenage boy suffering
from visceral leishmaniasis.
The boy exhibits splenomegaly, distended
abdomen and severe muscle wasting.
Visceral leishmaniasis (Kala-azar)
◼ Kala azar is the Indian name for visceral leishmaniasis.
◼ The term means "black disease“, which is a reference to the characteristic darkening of
the skin that is seen in patients with the disease.
◼ Incubation Period of visceral leishmaniasis ranges from 2 weeks to more than 1 year or
longer
◼ Visceral leishmaniasis can take different forms ranging from asymptomatic or self-
resolving disease.
◼ Bouts of fever, hepatosplenomegaly, diarrhea, anemia, and lymphadenopathy.
◼ In ~ 75-90%, it is lethal if untreated & 30% lethal if treated
◼ Post kala-azar dermal leishmaniasis occurs as a sequel of visceral leishmaniasis
Causative agents
◼ Cutaneous leishmaniasis
Americas -Leishmania tropica mexicana, Leishmania braziliensis, and Leishmania
amazonensis
Old World -Leishmania tropica, Leishmania major, L infantum, and Leishmania
aethiopica
◼ Mucocutaneous leishmaniasis
Americas -L braziliensis
Old World -L aethiopica
◼ Visceral leishmaniasis
India, Kenya -Leishmania donovani
South Europe, North Africa, & Middle East -L infantum
Americas -Leishmania chagasi
5
Reservoir
◼ Cutaneous Leishmaniasis:
Humans, rodents, & dogs
◼ Muco-cutaneous leishmaniasis: Rodents
◼ Visceral leishmaniasis:
Humans, rodents, & dogs
Risk factors
◼ Children are at greater risk than adults in endemic areas
◼ Malnutrition
◼ Persons with AIDS are at 100-1000 times greater risk of developing visceral leishmaniasis
in certain areas
◼ Incomplete therapy of initial disease is a risk factor for recurrence of leishmaniasis.
◼ Some studies have shown protection against cutaneous leishmaniasis with vaccination of
killed Leishmania promastigotes and (BCG).
◼ However, this does not seem to be protective against visceral leishmaniasis.
◼ The bite of one infected sand fly is sufficient to cause the disease, since a sand fly can
egest more than 1000 parasites per bite.
Life cycle
6
Prevention & control
◼ Most cases of Cutaneous leishmaniasi heal without treatment, leaving the person
immune to further infection.
◼ Other forms of leishmaniasis are extremely difficult to treat, often requiring a long course
of pentavalent antimony or sodium stibogluconate.
◼ Infection can be prevented by avoidance of sand fly bites through use of repellents or
insecticides.
The World Health Organization Response
WHO has set the following measures:
1. provide early diagnosis and prompt treatment.
2. control the sand fly population through residual insecticide spraying of houses and through
the use of insecticide-impregnated bed nets.
3. provide health education and produce training materials.
4. detect and contain epidemics in the early stages.
5. provide early diagnosis and effective management for Leishmania/HIV co- infections.
,,, Thank You ,,,