Cardiovascular system
Objective:• What is the action potential?
2. What is differences between the membrane properties of cardiac and skeletal muscle account for the prolonged action potential and the plateau in cardiac muscle?
cardiac action potential
is a brief change in voltage membrane potential across the cell membrane of heart cells.[1] This is caused by the movement of charged atoms (called ions) between the inside and outside of the cell, through protiens called ion channels.The cardiac action potential differs to action potentials found in other types of electrically excitable cells, such as nerves, as well as varying within the heart also, this is due to the presence of different ion channels in different cells
Unlike the action potential in skeletel muscle cell, the cardiac action potential is not initiated by nervous activity. Instead, it arises from a group of specialized cells, that have automatic action potential generation. In healthy hearts, these cells are found in the right atrium and are called the sinoatrial node .
They produce roughly 60-100 action potentials every minute. This action potential passes along the cell membrane causing the cell to contract, therefore the activity of the SAN results in a resting heart rate of roughly 60-100 beats per minute.
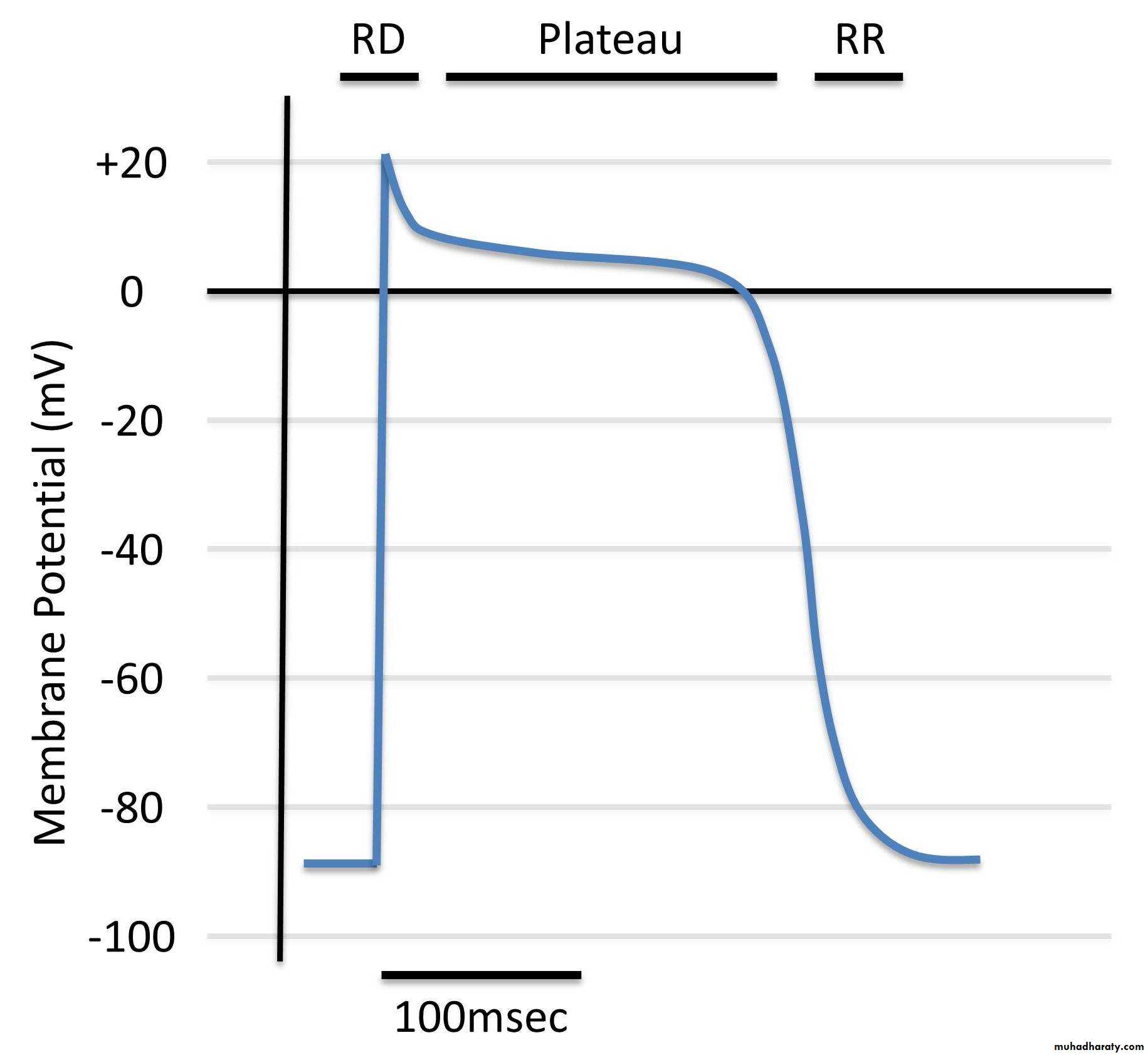
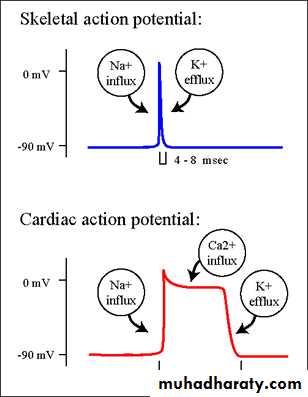
The action potential recorded in a ventricular muscle fiber averages about 105 millivolts, which means that the intracellular potential rises from a very negative value, about −85 millivolts, between beats to a slightly positive value, about +20 millivolts, during each beat.
After the initial spike, the membrane remains depolarized for about 0.2 second, exhibiting a plateau, followed at the end of the plateau by abrupt repolarization.
The presence of this plateau in the action potential causes ventricular contraction to last as much as 15 times as long in cardiac muscle as in skeletal muscle.
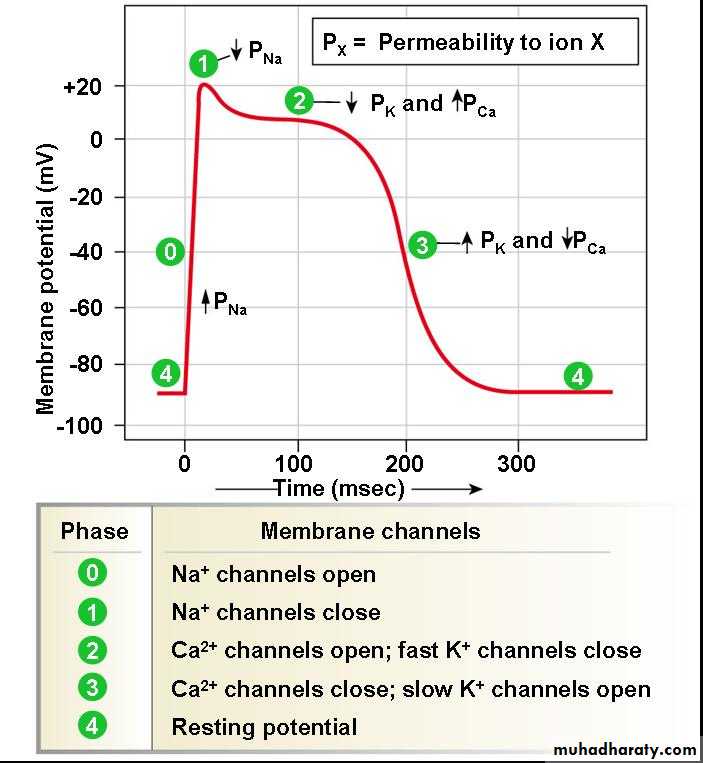
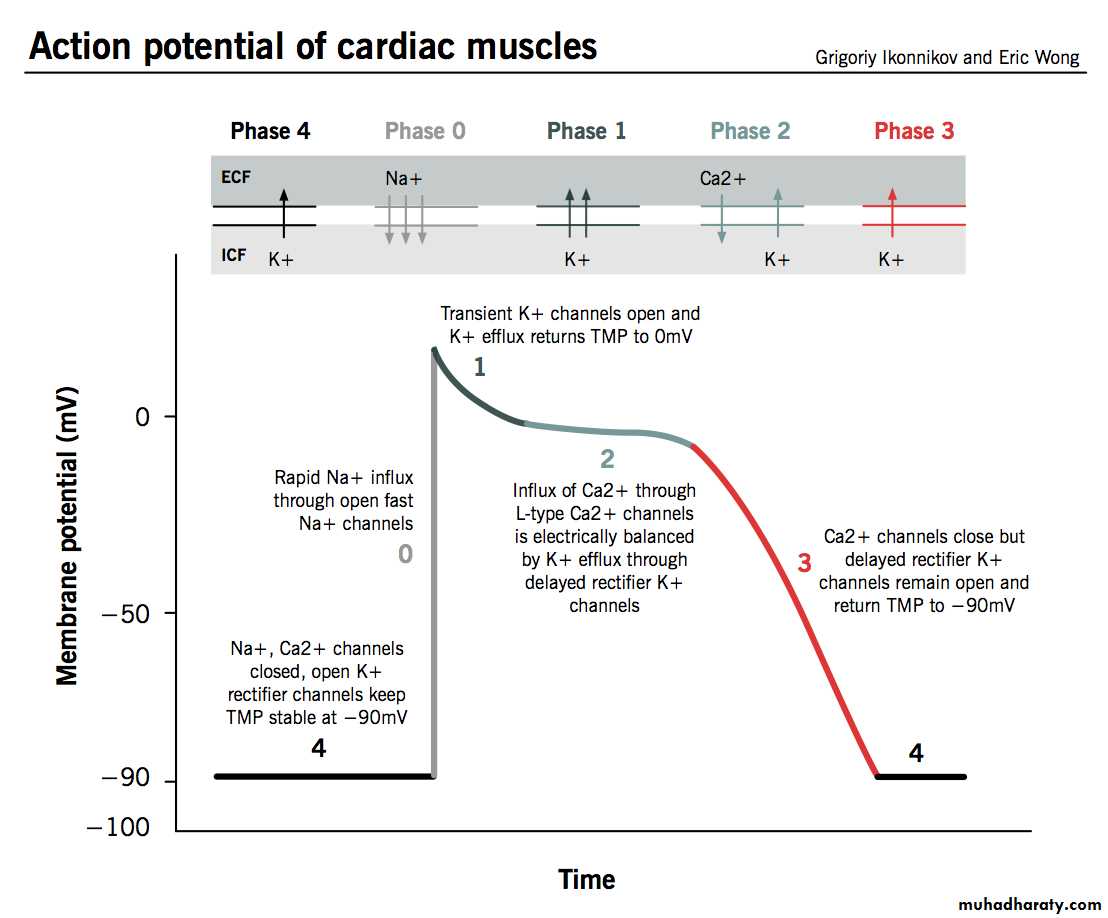
Phases of Cardiac Muscle Action Potential
Phase 0 (depolarization), fast sodium channels membrane potential becomes more positive. Voltage-gated sodium channels (fast sodium channels) open and permit sodium to rapidly flow into the cell and depolarize it. The membrane potential reaches about +20 millivolts before the sodium channels close.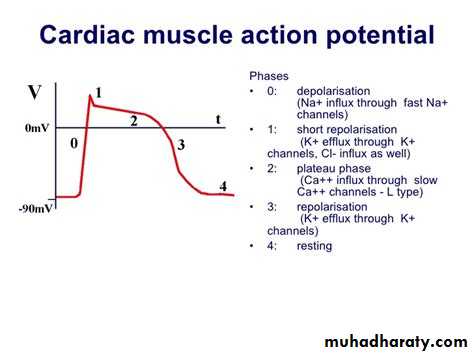
Phase 1 (initial repolarization), fast sodium channels close. The sodium channels close, the cell begins to repolarize, and potassium ions leave the cell through open potassium channels.
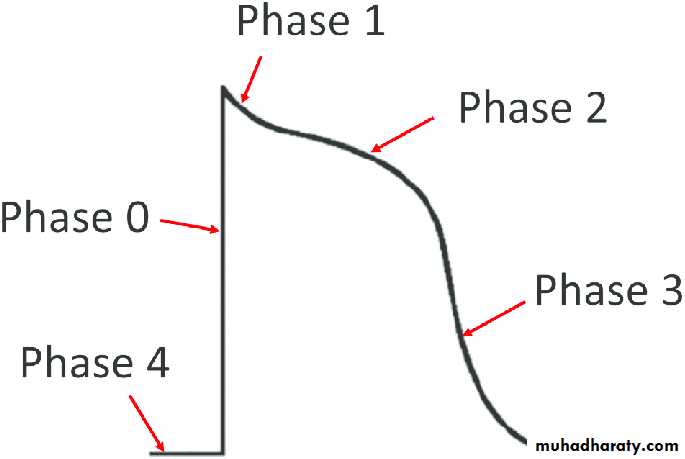
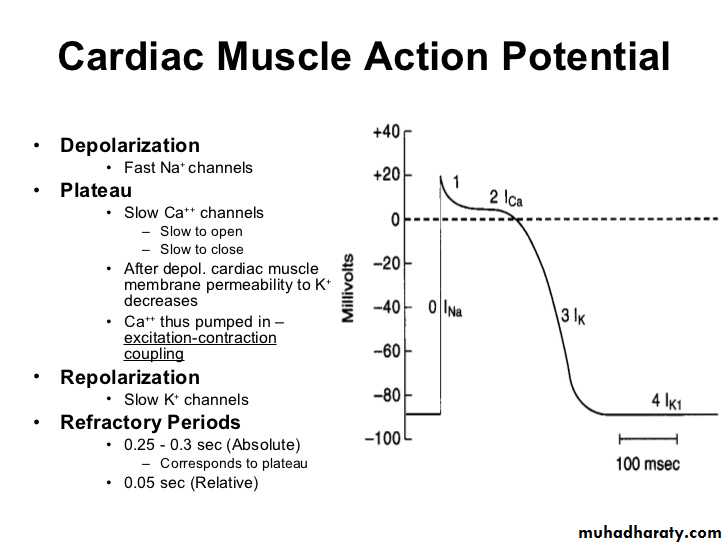
Phase 2 (plateau), calcium channels open and fast potassium channels close.
A brief initial repolarization occurs and the action potential then plateaus as a result of (1) increased calcium ion permeability and (2) decreased potassium ion permeability.
The voltage-gated calcium ion channels open slowly during phases 1 and 0.Potassium channels then close, and the combination of decreased potassium ion efflux and increased calcium ion influx causes the action potential to plateau.
Phase 3 (rapid repolarization), calcium channels close and slow potassium channels open. The closure of calcium ion channels and increased potassium ion permeability, permitting potassium ions to rapidly exit the cell, ends the plateau and returns the cell membrane potential to its resting level.
Phase 4 (resting membrane potential) averages about −90 millivolts.
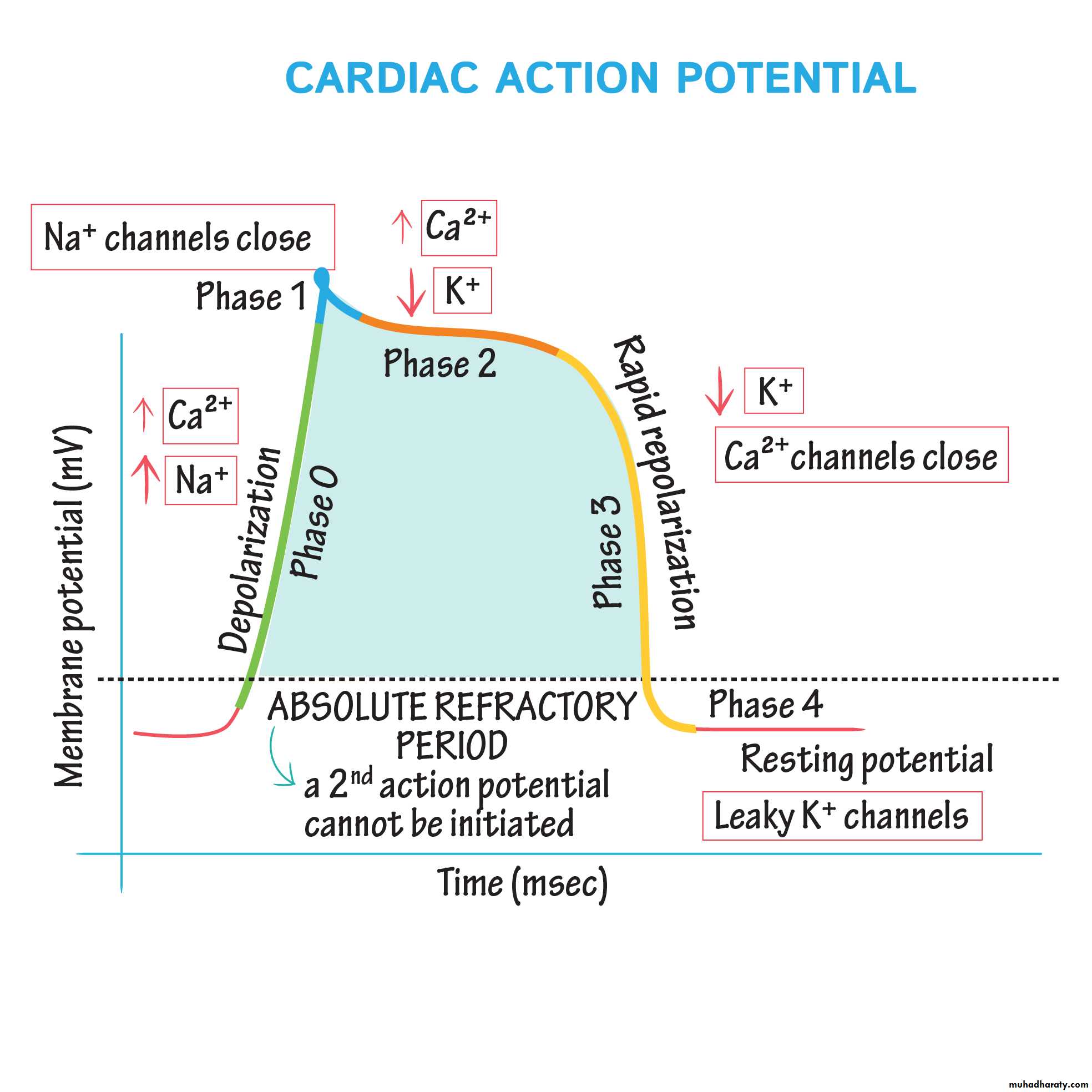
Refractory Period of Cardiac Muscle.
Cardiac muscle, like all excitable tissue, is refractory to restimulation during the action potential. Therefore, the refractory period of the heart is the interval of time during which a normal cardiac impulse cannot re-excite an already excited area of cardiac muscle.The normal refractory period of the ventricle is 0.25 to 0.30 second, which is about the duration of the prolonged plateau action potential. The refractory period of atrial muscle is much shorter than that for the ventricles (about 0.15 second for the atria compared with 0.25 to 0.30 second for the ventricles).
What is differences between the membrane properties of cardiac and skeletal muscle account for the prolonged action potential and the plateau in cardiac muscle?
At least two major differences between the membrane properties of cardiac and skeletal muscle account for the prolonged action potential and the plateau in cardiac muscle.
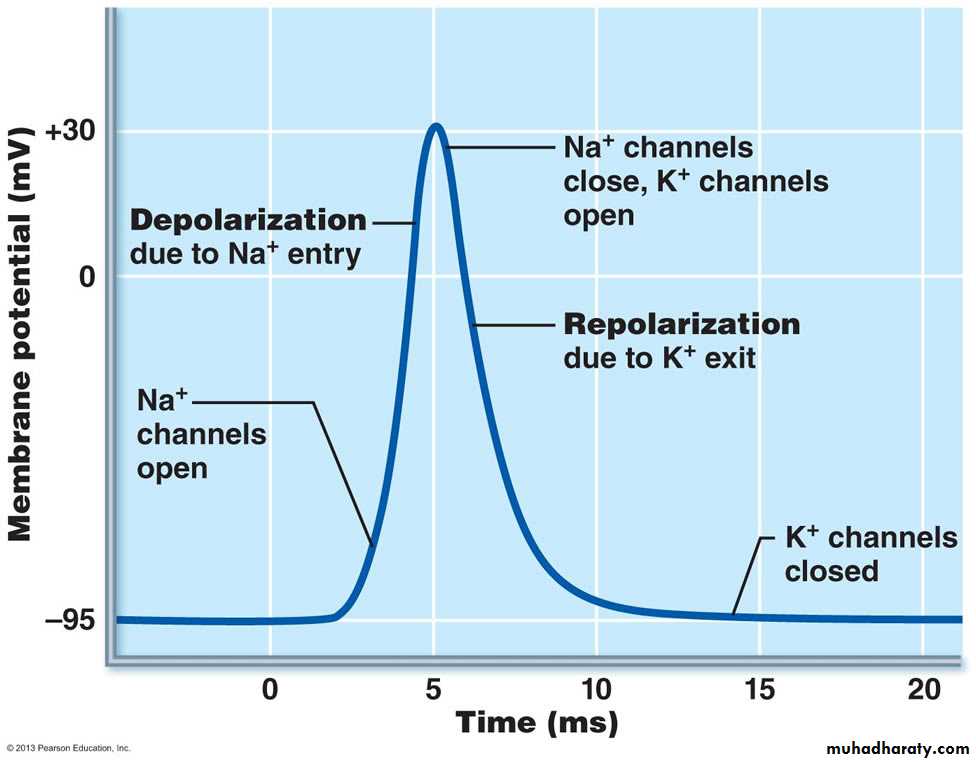
First, the action potential of skeletal muscle is caused almost entirely by the sudden opening of large numbers of fast sodium channels that allow tremendous numbers of sodium ions to enter the skeletal muscle fiber from the extracellular fluid. These channels are called “fast” channels because they remain open for only a few thousandths of a second and then abruptly close. . At the end of this closure, repolarization occurs, and the action potential is over within another thousandth of a second or so.
In cardiac muscle, the action potential is caused by opening of two types of channels: (1) the same voltage-activated fast sodium channels as those in skeletal muscle and (2) another entirely different population of L-type calcium channels (slow calcium channels), which are also called calcium-sodium channels. This second population of channels differs from the fast sodium channels in that they are slower to open and, even more important, remain open for several tenths of a second.
During this time, a large quantity of both calcium and sodium ions flows through these channels to the interior of the cardiac muscle fiber, and this activity maintains a prolonged period of depolarization, causing the plateau in the action potential.
The second major functional difference between cardiac muscle and skeletal muscle that helps account for both the prolonged action potential and its plateau is this: Immediately after the onset of the action potential, the permeability of the cardiac muscle membrane for potassium ions decreases about fivefold, an effect that does not occur in skeletal muscle.
This decreased potassium permeability may result from the excess calcium influx through the calcium channels just noted.
Regardless of the cause, the decreased potassium permeability greatly decreases the outflux of positively charged potassium ions during the action potential plateau and thereby prevents early return of the action potential voltage to its resting level..
When the slow calcium-sodium channels do close at the end of 0.2 to 0.3 second and the influx of calcium and sodium ions ceases, the membrane permeability for potassium ions also increases rapidly; this rapid loss of potassium from the fiber immediately returns the membrane potential to its resting level, thus ending the action potential

• What is the correct pathway for the heart's conducting system?
• SA node → AV node → Bundle branches → Bundle of His → Purkinje• SA node → AV node → Bundle of His → Bundle branches → Purkinje fibers
• SA node → AV node → Bundle of His → Purkinje fibers → Bundle branches
• SA node → AV node → Purkinje fibers → Bundle of His → Bundle
• branches AV node → SA node → Bundle of His → Bundle branches → Purkinje fibers
In a cardiac muscle cell, the membrane potential increases rapidly...
• when potassium gates open and potassium diffuses into the cardiac muscle fiber.• when potassium gates open and potassium diffuses out of the cardiac muscle fiber.
• when the sodium gates open and sodium diffuses into the cardiac muscle fiber
• when the sodium gates open and sodium diffuses out of the cardiac muscle fiber.
