Body of uterus:-
Endometritis:-Inflammation of the endometrium is classified as acute or chronic depending on whether a neutrophilic or a lymphoplasmacytic infiltrate predominates, respectively. The diagnosis of chronic endometritis generally requires the presence of plasma cells, as lymphocytes are present even in the normal endometrium. Endometritis is a component of pelvic inflammatory disease (PID) and is frequently a result of N. gonorrhoeae or C. trachomatis infection.
Histologic examination: shows a neutrophilic infiltrate in the superficial endometrium coexisting with a stromal lymphoplasmacytic infiltrate. Tuberculosis causes granulomatous endometritis, frequently with associated tuberculous salpingitis and peritonitis. Although seen in the United States mainly in immunocompromised persons, tuberculous endometritis is common in countries in which tuberculosis is endemic . Endometritis also may be a result of retained products of conception subsequent to miscarriage or delivery or the presence of a foreign body such as an intrauterine device. Removal of the offending tissue or foreign body typically results in resolution.
Clinically: all forms of endometritis manifest with fever, abdominal pain, and menstrual abnormalities. In addition, there is an increased risk of infertility and ectopic pregnancy due to damage and scarring of the fallopian tubes.
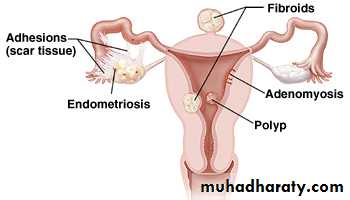
Adenomyosis:-
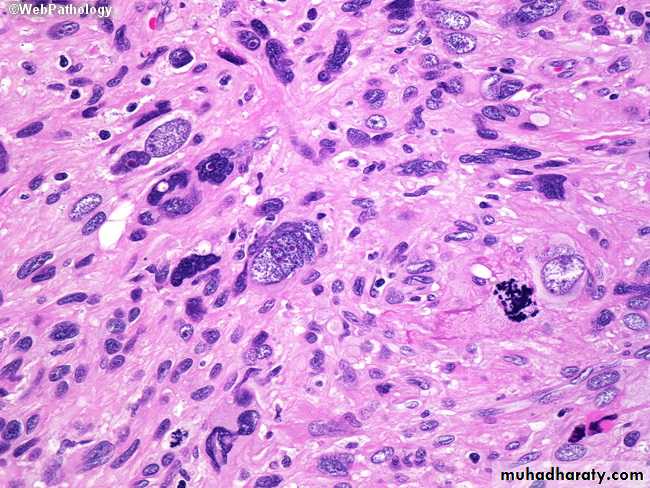
This condition is characterized by implantation of both endometrial glands and stroma from basal layer of endometrium between myometrial layers which cause reactive hypertrophy of myometrium, menorrhagia, dysmenorrhea and pelvic pain.


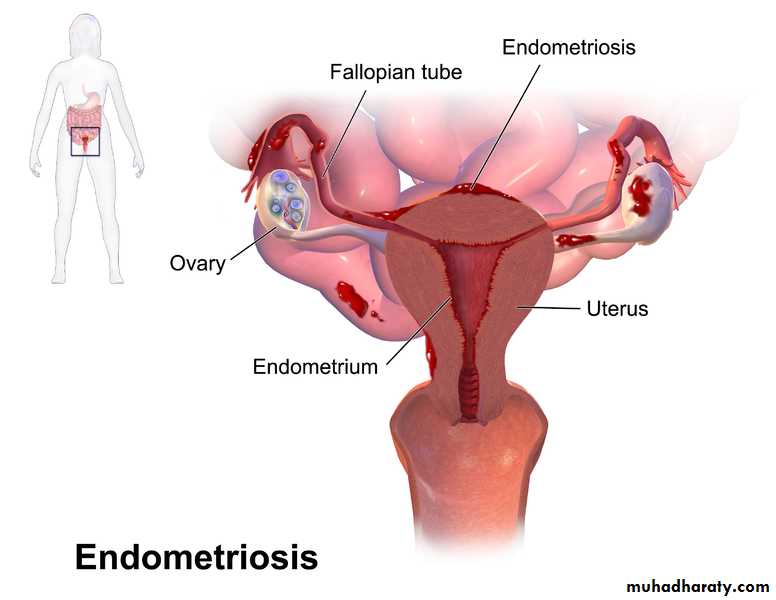
Endometriosis:-
endometriosis, it often causes infertility, dysmenorrhea and pelvic pain, this condition consist of functioning endometrial tissue in the pelvis ( ovaries, pouch of Douglas, uterine ligaments, tubes and rectovaginal septum also may be seen in peritoneal cavity, about the umbilicus also can be seen then in LN, lungs, heart and bone. It occurs in as many as 10% of women in their reproductive years and in nearly half of women with infertility.Four hypotheses have been put forth to explain the origin of dispersed endometriotic lesions, we take the most 2 important hypothesis:
• The regurgitation theory, which is currently favored, proposes that menstrual backflow through the fallopian tubes leads to implantation.
• The benign metastases: theory holds that endometrial tissue from the uterus can “spread” to distant sites via blood vessels and lymphatics.
So it's suffering from cyclic changes of menstrual cycle, in ovaries it will form large blood filled cysts which's called chocolate cyst as the blood ages, the organization of the blood leads to fibrosis and adherence of pelvis structure so cause infertility.
The microscopical diagnosis depend on finding 2 of following 3 features, endometrial glands, stroma and hemosiderin pigment.
Dysfunctional uterine bleeding
DUB:-Women commonly seek medical attention for abnormal uterine bleeding, such as menorrhagia (profuse or prolonged bleeding at the time of the period), metrorrhagia (irregular bleeding between the periods), or postmenopausal bleeding. Common causes include dysfunctional uterine bleeding, endometrial polyps, leiomyomas, endometrial hyperplasia, and endometrial carcinoma. Abnormal bleeding from the uterus in the absence of an organic uterine lesion is called dysfunctional uterine bleeding. The most common cause of dysfunctional uterine bleeding is anovulation (failure to ovulate). Anovulatory cycles result from hormonal imbalances and are most common at menarche and in the perimenopausal period because of fluctuations in the hypothalamus/pituitary/ovarian axis
PROLIFERATIVE LESIONS OF THE ENDOMETRIUM AND MYOMETRIUM
The most common proliferative lesions of the uterine corpus are endometrial hyperplasia, endometrial carcinomas, endometrial polyps, and smooth muscle tumors. All tend to produce abnormal uterine bleeding .
Endometrial hyperplasia:-
An excess of estrogen relative to progestron if prolonged and marked induce endometrial hyperplasia which is ranging from simple hyperplasia to moderate, complex hyperplasia and atypical hyperplasia these changes depend on level and duration of exposure to estrogen effect, the imporatance of hyperplasia especially complex and atypical which is caused abnormal uterine bleeding and it's a premalignant condition also called endometrial intraepithelial neoplasia (EIN) cause adenocarcinoma of endometrium.

Endometrial carcinoma:-
It's most frequent cancer of female genital tract after early detection and treatment of CIN.Pathogenesis:-
Endometrial carcinoma usually occur in post menopausal women, so it's uncommon below the age of 40 years.
The main risk factor is increased estrogen stimulation as in endometrial hyperplasia and this also depend on dosage and duration of estrogen stimulation.
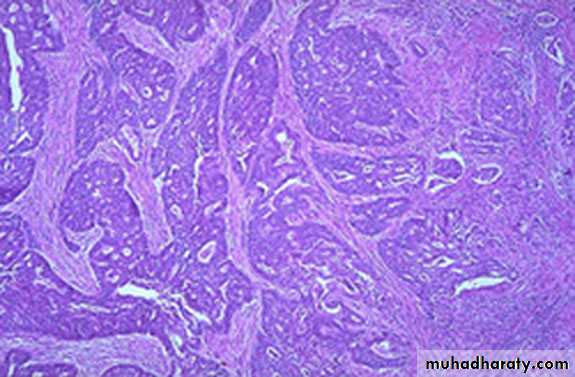
Morphology:-
Endometrial carcinoma occur on one of 2 forms either appear as infiltrative causing diffuse thickening of the affected uterine wall or appear as exophytic form.
Microscopiaclly: most of these tumors are adenocarcinomas with either well defined glands resembling the endometrial glands from which arose or less well differentiated tumors forming solid sheets of cells with nuclear a typia and mitotic activity.
So grading of carcinoma according to differentiation into grade I to III from well differentiated to undifferentiated.
While staging according to it's dissemination.
Endometrial polyps:-
Which is small sessile mass project from endometrium, Larger polyps may project from the endometrial mucosa into the uterine cavity and even from uterine cervix.Histologically seen as polyp lined by columnar epithelium and contain in stroma endo metrial glands which are sometimes showing cystically dilated glands on fibrosed stroma.
The clinical manifestation of endometrial polyps in producing uterine bleeding and rarely progress to adenocarcinoma.
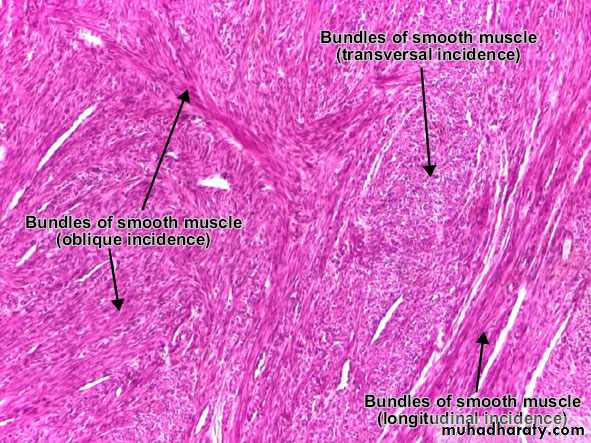
Leiomyoma:-
It's most common benign tumor occur in female during reproductive life, it's effected by estrogen and oral contraceptive, so that it's shrink in size in menopause, it's a benign tumor of smooth muscle cells of myometrium but because of firm consistency called fibroid, Leiomyomas of the uterus often are asymptomatic, being discovered incidentally on routine pelvic examination. The most frequent presenting sign is menorrhagia, with or without metrorrhagia. Leiomyomas rarely, if ever, transform into sarcomas.Morphology:-
Macroscopically: it appear as sharply circumscribed, firm, grey to white mass with whorled cut surface, it may occur singly but more often as multiple masses either "transmural" in wall or submucosal or subserosal.
Microscopically: appear as proliferated myocytes arranged in interlacing bundles forming whorles with no atypia of proliferated myocytes.

Leiomyosarcoma:-
It's a malignant tumor arise from leiomyocytes of uterus and not from leiomyoma, it's unlike leiomyoma usually arise as single mass.Histologically: It's represent a wide range of differentiaition, from those that closely resemble leiomyoma to anaplastic tumors, diagnostic features of leiomyosarcoma include relatively frequent mitoses with or without cellular atypia or less numerous mitoses with cellular atypia.
Fallopian tubes:-
Inflammations ( Salpingitis )Are almost always caused by bacteria and may be affected by T.B in combination with infection of endometrium.
The importance of chronic inflammation in causing of obstruction of tubal lumen and caused perminant infertility,
Other diseases of F.T are ectopic (tubal) pregnancy and endometriosis
Neoplasms: primary adenocarcinoma, it's rare neoplasm and usually can't discovered until spread.
Ovaries:-
Primary inflammation of ovary is very rare condition.
Follicular and luteal cysts:-
It's a common condition, that is physiologic in nature, it's caused by unruptured Graafian follicles, they are often multiple, may reached 4-5 cm in diameter filled by serous fluid and microscopically lined by granoulosa or luteal cells.
The clinical importance of this cyst, it's may be ruptured and producing intraperitoneal bleeding and acute abdominal symptom.
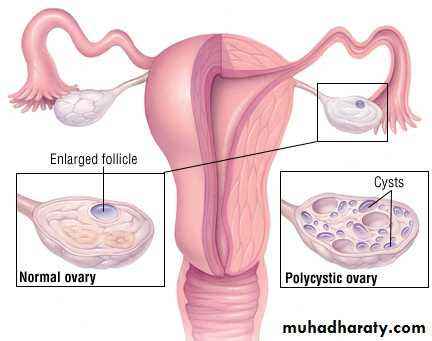
Polycystic ovaries:-
Polycystic ovarian syndrome (formerly called Stein-Leventhal syndrome) is a complex endocrine disorder characterized by hyperandrogenism because of multiple cysts in ovaries produced estrogens and androgen, so the patient present with menstrual abnormalities, polycystic ovaries, chronic anovulation, and decreased fertility. It usually comes to attention after menarche in teenage girls or young adults who present with oligomenorrhea, hirsutism, infertility, and sometimes with obesity.
This appear in ovary as multiple subcortical cysts measured 0.5 to 1.5 cm and appear microscopically as cyst lined by granulosa cells.