
Mycobacterium

Introduction
• Grow slowly
• Acid fast bacteria
• Have mycolic acids
• Virulence factor → complex, lipid-rich cell wall
– Is responsible for many of the characteristic prope
rties of the bacteria (e.g. acid fastness, slow growt
h, resistance to detergents, resistance to common
antibacterial agents and antigencity)

Mycobacterium Tuberculosis
• Infection is acquired through the inhalation of
aerosolized infectious particles, which then tra
vel to the terminal airways

Mycobacterium Tuberculosis
• At this site, the bacteria penetrate into un activated a
lveolar macrophages (phagocytized and prevents fusi
on of phagosome with lysosomes) and replicate freel
y
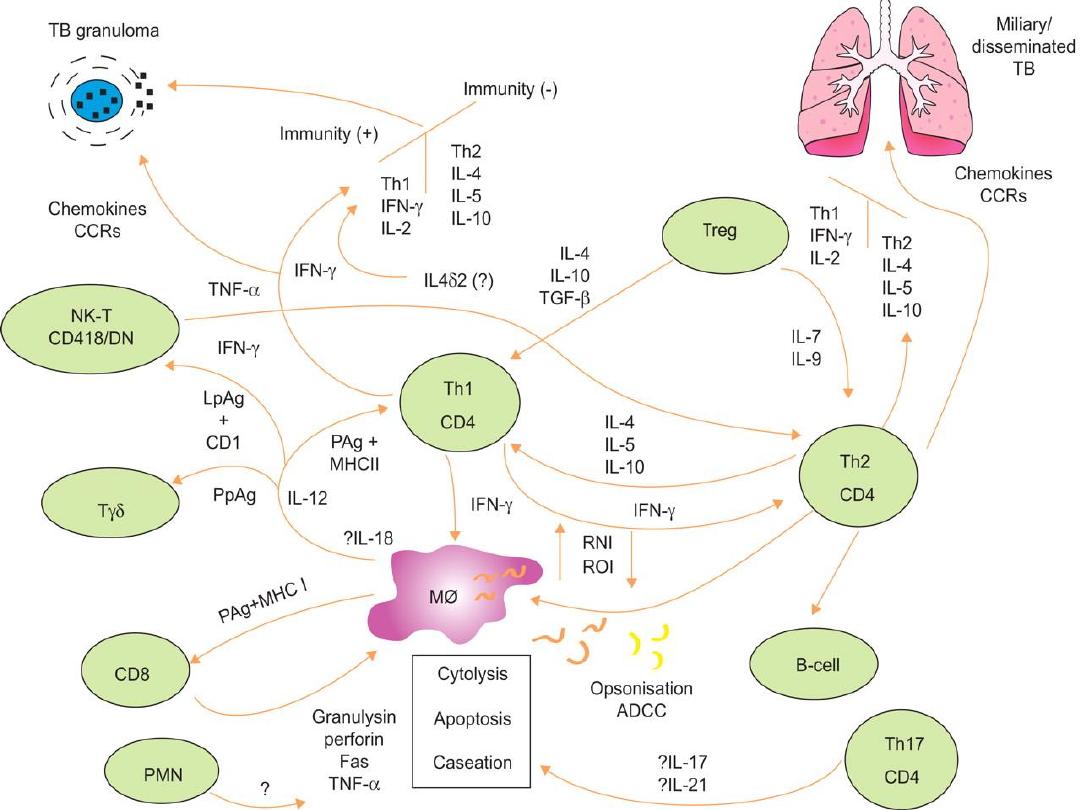
• The organism then elicit a cell-mediated response
• The intracellular replication of mycobacteria stimulat
es both helper (CD4+) and cytotoxic (CD8+) T cells to
form granuloma.

Mycobacterium Tuberculosis
• Virulence factors
– Organism able to replicate in nonactivated macrop
hages
– Can survive for years in dormant state
– Pathology depends on host’s response to infection
rather than produced by bacterial toxins or enzym
es (no toxins associated)
Mycobacterium Tuberculosis
• Disease can come on suddenly with patients h
aving nonspecific complaints of malaise, weig
ht loss, cough and night sweats

Constituents of Tubercle Bacilli
Mycobacterial cell contents only elicit delayed hypersensitivity reactions in pre
viously sensitized animals.
Lipids
Mycobacteria are rich in lipids. These include mycolic acids , waxes, and phosp
hatides. In the cell, the lipids are largely bound to proteins and polysaccharides
. Lipids are to some extent responsible for acid-fastness.
Proteins
Each type of mycobacterium contains several proteins that elicit the tuberculin
reaction. Proteins bound to a wax fraction can, upon injection, induce tuberculi
n sensitivity such as purified protein derivative (PPD). They can also elicit the fo
rmation of a variety of antibodies.
Polysaccharides
Mycobacteria contain a variety of polysaccharides. Their role in the pathogene
sis of disease is uncertain. They can induce the immediate type of hypersensiti
vity and can serve as antigens in reactions with sera of infected persons.

Mycobacterium Leprae
• Causes leprosy (also called Hansen’s disease)
• Endemic disease found in armadillos
• Spread by person-to-person contact by inhalation of i
nfectious aerosols or direct contact with lesions
• Clinical manifestation depend on the patient’s immu
ne reaction to bacilli
Mycobacterium Leprae
• Tuberculoid leprosy
– Low infectivity
– Strong cellular immune response but a weak humoral anti
body reponse
– Infected tissues typically have many lymphocytes and gran
ulomas but relatively few bacilli
• Lepromatous leprosy
– Most infectious form
– Strong antibody response but a specific defect in their cell
ular response to M. leprae antigens
– An abundance of bacilli are typically observed in dermal m
acrophages and the Schwann cells of peripheral nerves

Mycobacterium Avium Complex
• M. avium and M. intracellulare
• Invades the gut
• Found in AIDS patients
• Acquired through ingestion of contaminated f
ood or water
Laboratory Diagnosis of Mycobacterial Dise
ases
• Skin Test (subcutaneous)
–Use purified protein derivative (PPD) of
cell wall
–If the person was exposed, it will swell
–After positive test, use chest X-ray to lo
ok lesions

Laboratory Diagnosis of Mycobacterial Dise
ases
• Acid Fast Stained Bacilli
–Stained with carbol-fuschin and de
colorized with acid-alcohol and stai
ned with counterstained

• Culture
• The media for primary culture of mycobacteria
should include a nonselective medium and a s
elective medium. Selective media contain anti
biotics to prevent the overgrowth of contamin
ating bacteria and fungi. There are three gene
ral formulations that can be used for both the
nonselective and selective media.

• Semisynthetic Agar Media
• These media (eg, Middlebrook 7H10 and 7H11) c
ontain defined salts, vitamins, cofactors, oleic aci
d, albumin, catalase, glycerol, glucose, and malac
hite green; the 7H11 medium contains casein hyd
rolysate also, these media may be less sensitive t
han other media for primary isolation of mycobac
teria.
• The semisynthetic agar media are used for observ
ing colony morphology, for susceptibility testing,
and, with added antibiotics, as selective media.

• Inspissated Egg Media
• These media (eg, Löwenstein-Jensen) contain
defined salts, glycerol, and complex organic su
bstances (eg, fresh eggs or egg yolks, potato fl
our, and other ingredients in various combinat
ions). Malachite green is included to inhibit ot
her bacteria. Small inocula in specimens from
patients will grow on these media in 3–6 week
s.These media with added antibiotics are used
as selective media.

• Broth Media
• Broth media (eg, Middlebrook 7H9 a
nd 7H12) support the proliferation of
small inocula. Growth is often more r
apid than on complex media.

• Mycobacteria tend to be more resistant to che
mical agents than other bacteria because of th
e hydrophobic nature of the cell surface and t
heir clumped growth. Dyes (eg, malachite gree
n) can be incorporated into media without inh
ibiting the growth of tubercle bacilli. Acids and
alkalis permit the survival of some exposed tu
bercle bacilli . Tubercle bacilli are resistant to d
rying and survive for long periods in dried sput
um.

• Pathology
• The production and development of l
esions and their healing or progressi
on are determined chiefly by (1) the
number of mycobacteria in the inocu
lum and their subsequent multiplicat
ion, and (2) the resistance and hyper
sensitivity of the host.

• Two Principal Lesions
• Exudative Type
• This consists of an acute inflammatory re
action, with edema fluid, polymorphonuc
lear leukocytes, and, later, monocytes aro
und the tubercle bacilli. This type is seen
particularly in lung tissue, where it resem
bles bacterial pneumonia

• Productive Type
• When fully developed, this lesion, a chronic gr
anuloma, consists of three zones: (1) a central
area of large, multinucleated giant cells contai
ning tubercle bacilli; (2) a mid zone of pale epi
thelioid cells, often arranged radially; and (3) a
peripheral zone of fibroblasts, lymphocytes, a
nd monocytes. Later, peripheral fibrous tissue
develops, and the central area undergoes case
ation necrosis. Such a lesion is called a tubercl
e.

Treatment
• Chemoprophylaxis
– 6 months
– Isoniazid (INH) for 6 months
– 4 months of rifampin
– 2 months of Pyrazinamide

Epidemiology
The most frequent source of infection is the human who excr
etes, large numbers of tubercle bacilli. Close contact (eg, in th
e family) and massive exposure (eg, in medical personnel) ma
ke transmission by droplet nuclei most likely. Susceptibility t
o tuberculosis is a function of the risk of acquiring the infectio
n and the risk of clinical disease after infection has occurred. F
or the tuberculin-negative person, the risk of acquiring tuberc
le bacilli depends on exposure to sources of infectious bacilli
—principally sputum-positive patients. This risk is proportiona
te to the rate of active infection in the population, crowding, s
ocioeconomic disadvantage, and inadequacy of medical care.

Mycobacterium leprae

The onset of leprosy is insidious. The lesions involve the
cooler tissue of the body: skin, superficial nerves, nose,
pharynx, larynx, eyes, and testicles. The skin lesions ma
y occur as pale, anesthetic macular lesions 1–10 cm in
diameter; diffuse or discrete erythematous, infiltrated
nodules 1–5 cm in diameter; or a diffuse skin infiltratio
n. Neurologic disturbances are manifested by nerve infil
tration and thickening, with resultant anesthesia, neurit
is, paresthesia, trophic ulcers, and bone resorption and
shortening of digits. The disfigurement due to the skin i
nfiltration and nerve involvement in untreated cases m
ay be extreme.

The disease is divided into two major types, lepromatous an
d tuberculoid, with several intermediate stages. In the lepro
matous type, the course is progressive and malign, with no
dular skin lesions; slow symmetric nerve involvement; abun
dant acid-fast bacilli in the skin lesions; continuous bactere
mia; and a negative lepromin (extract of lepromatous tissue
) skin test. In lepromatous leprosy, cell-mediated immunity i
s markedly deficient and the skin is infiltrated with suppress
or T cells. In the tuberculoid type, the course is benign and
nonprogressive, with macular skin lesions, severe asymmetr
ic nerve involvement of sudden onset with few bacilli prese
nt in the lesions, and a positive lepromin skin test. In tuberc
uloid leprosy, cell-mediated immunity is intact and the skin i
s infiltrated with helper T cells.

Scrapings with a scalpel blade from skin or nasal
mucosa or from a biopsy of earlobe skin are s
meared on a slide and stained by the Ziehl-Ne
elsen technique. Biopsy of skin or of a thicken
ed nerve gives a typical histologic picture. No s
erologic tests are of value. Non-treponemal se
rologic tests for syphilis frequently yield false-
positive results in leprosy.

• Treatment
• Sulfones such as dapsone are first-line th
erapy for both tuberculoid and lepromat
ous leprosy. Rifampin or clofazimine gene
rally is included in the initial treatment re
gimens. Other drugs active against M lep
rae include minocycline, clarithromycin, a
nd some fluoroquinolones.

• Epidemiology
• Transmission of leprosy is most likely to o
ccur when small children are exposed for
prolonged periods to heavy shedders of b
acilli. Nasal secretions are the most likely
infectious material for family contacts. Th
e incubation period is probably 2–10 year
s. Without prophylaxis, about 10% of exp
osed children may acquire the disease.

• Prevention & Control
• Identification and treatment of patients with leprosy
are the keys to control. Children of presumably conta
gious parents are given chemoprophylactic drugs unt
il treatment of the parents has made them noninfecti
ous. If any member of a domestic group has leproma
tous leprosy, such prophylaxis is required for children
in the group. Experimental BCG vaccination and an M
leprae vaccine are also being explored for family cont
acts and possibly for community contacts in endemic
areas.

THANKS