1
Hepatitis Viruses
Thi-Qar University /College of Medicine/
Third stage
Virology / Theory
Dr. Entedar Alioy, PhD, MSc. Microbiology.
Hepatitis Viruses
Hepatitis is a clinical syndrome caused by many pathogens including viruses.
There are six medically important viruses that are called hepatitis viruses
because their main site of infection is liver. These viruses are hepatitis A virus
(HAV), hepatitis B virus (HBV), hepatitis C virus (HCV), hepatitis D virus
(HDV), hepatitis E virus (HEV).
Although these viruses infect the liver as common target organ, they however,
differ greatly in their morphology, replication pattern, and course of infection.
These viruses infect the liver and cause distinct clinical pathology by producing
characteristic symptoms of jaundice and production and release of liver enzymes
in the serum.
Hepatitis C virus

2
Hepatitis A Virus
Hepatitis A virus (HAV) is a picornavirus that is most commonly transmitted by
fecal–oral route. It has an incubation period of 3–4 weeks after which jaundice
starts suddenly. It is unique in that it does not cause chronic disease or fatal
disease. Human are only natural host. Only one serotype is known.
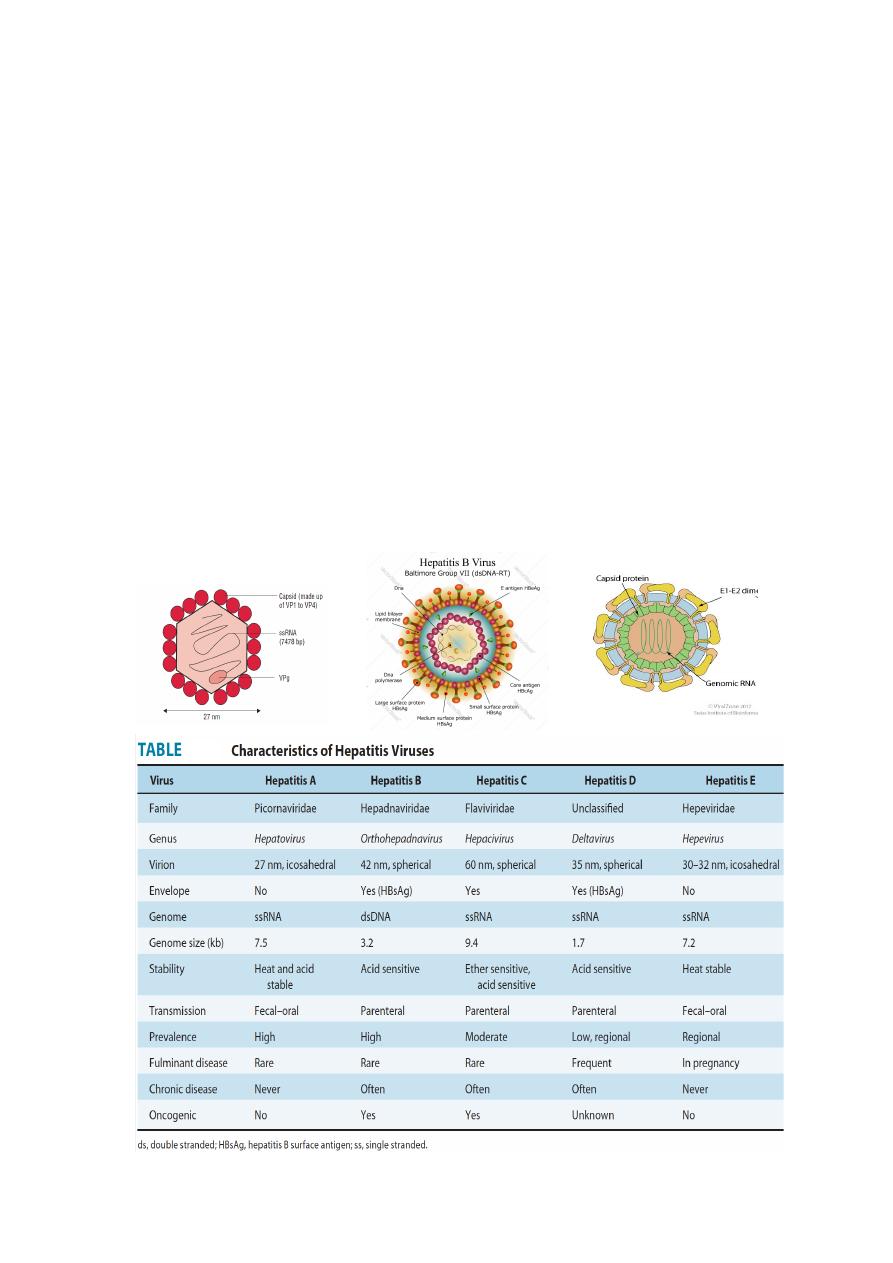
Morphology Is a typical enterovirus in the family Picornaviridae, a small, non
enveloped virus measuring 27 nm in diameter. It has a single-stranded positive-
sense RNA genome (See-Figure).
Viral replication
•
Hepatitis A virus replicates in the cytoplasm of the infected cell.
•
Briefly, it combines specifically with a receptor expressed on liver cells
and few other cells. However, unlike other picornaviruses, It is not
cytolytic and is released by exocytosis.
Clinical Syndrome
Acute hepatitis A
The incubation period of HAV is 15–45 days, with an average of 4 weeks.
Fatigue, nausea, vomiting, fever, hepatomegaly, jaundice, anorexia, and rash are
the most common signs and symptoms of the disease. The condition is also
associated with passing of dark-colored urine, pale feces, and elevated serum
transaminase levels.
HAV infection is usually a self-limiting mild disease and in most cases resolves
spontaneously in 2–4 weeks. HAV infection confers lifelong immunity to HAV.
²
Chronic hepatitis or chronic carrier state does not occur with HAV
infection.
²
Hepatitis A virus also never causes hepatocellular carcinoma.
Transmission of HAV infection
•
Humans are the reservoirs for HAV.
•
Contaminated food or water is the main source of infection.
•
Wide outbreak can occur from a single contaminated source, such as
uncooked vegetables and contaminated food and water.
•
Prevention
•
(a ) Vaccines.
•
(b ) Prophylaxis with immune serum globulin.
•
(c ) Measures to prevent feco-oral spread of infection.
Inactivation of HAV.
•
The virus is inactivated by formalin (0.35%) at 37°C during a period of 24
hours.
•
By treatment with peracetic acid (2%) for 4 hours.
•
Beta-propiolactone (0.25%) for 1 hour.
•
It is also inactivated by exposure to ultraviolet radiation.
•
The virus is inactivated by routine chlorine treatment of drinking water.
3
•
The virus is destroyed by autoclaving (121 ÅãC for 20 minutes) and
boiling in water for 5 minutes,
Hepatitis A virus is highly resistant to environmental factors.
•
It is stable at 60°C for 1 hour, 56°C for 30 minutes, and 4°C for weeks.
•
It is stable to acidic pH, at pH 1.
•
It is resistant to inactivation by lipid solvents, such as ether and
chloroform, to action of detergents, and to drying.
Laboratory Diagnosis: Specimens These include:
(a) Serum for antibody detection test. Serological tests demonstrating
these anti-HAV antibodies in the serum are the most widely used to
confirm the diagnosis of HAV infection.
Enzyme-linked immunosorbent assay (ELISA) is the method of choice for
detection of IgM and IgG antibodies in the serum.
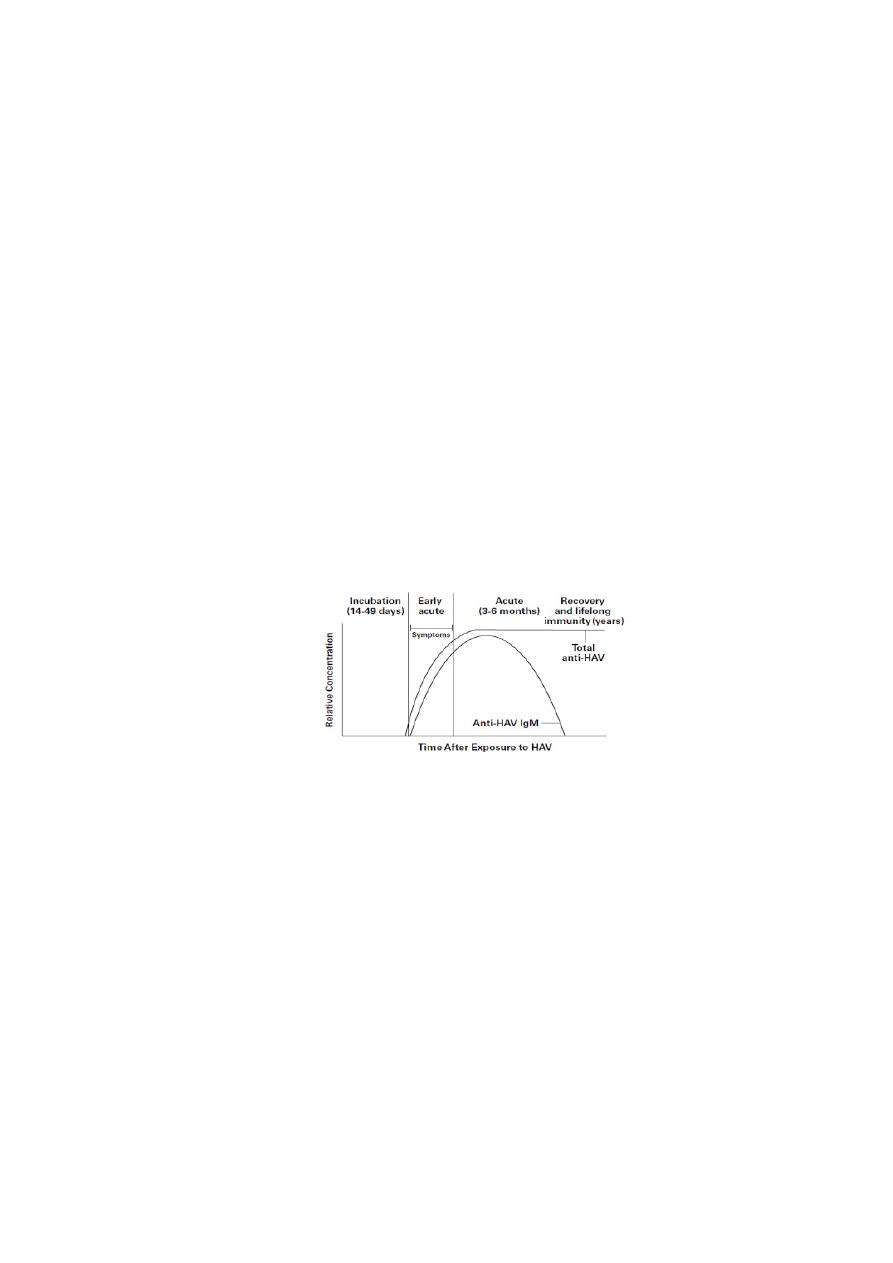
IgM antibody is the first antibody to appear at the onset of symptoms and
continues to persist at a high level for 1–2 months. It usually disappears by 4–6
months but occasionally persists longer. Hence, demonstration of IgM antibody
is diagnostic of a recent infection. IgG antibody appears in the serum shortly
after the appearance of IgM antibodies and usually increases as the IgM level
decreases. A fourfold rise in IgG antibody titers is also diagnostic of infection.
(b) Liver, bile, stool, and blood for HAV antigen and genome.
(c) Molecular Diagnosis : DNA probes and Polymerase chain reaction (PCR)
are used to demonstrate HAV genome in stool of infected patient.
Treatment : No antiviral therapy is available against HAV infection. Treatment
of the condition is always supportive.
Prevention
(a ) Vaccines.
(b ) Prophylaxis with immune serum globulin.
(c ) Measures to prevent feco-oral spread of infection.
***************************************************************************
Hepatitis B Virus (HBV)
Hepatitis B virus is a major cause of infectious hepatitis worldwide. It is a
hepadnavirus, which shows restricted host range and limited tissue tropism. The
virus usually causes chronic disease and is associated with hepatocellular
carcinoma.
Morphology

4
HBV shows following features: It is a small (3.2 kb), enveloped DNA virus. The
genome is a small, circular, partially double-stranded DNA. It is partially double
stranded, because its positive strand is incomplete. The complete negative
strand possesses four genes: genes S, C, P, and X. The gene S codes for HBsAg and
also for HBeAg (hepatitis B e antigen). The virion is a double-walled, spherical
structure and measures 42 nm in diameter .The HBV consists of nucleocapsid
which surrounds HBV DNA and DNA polymerase The nucleocapsid also encloses
a protein attached to genome, which is surrounded by hepatitis B core antigen
(HBcAg). The envelope which encloses the virus consists of HBsAg and also
HBeAg.
Hepatitis
B
virus replication
The virus replicates in the nucleus of the cell. The virus infects hepatocytes, the
attachment of which is mediated by HBsAg glycoprotein. The infection is
initiated by the binding of HBsAg to serum albumin and other serum proteins,
which subsequently causes the virus to infect the liver.
Inside hepatocytes, the partial DNA strand of the genome is converted to
covalently closed circular double-stranded DNA (ccc DNA). Later on, this genome
is transported to the nucleus of the cell In the nucleus, the partially double-
stranded viral genome is converted to covalently closed circular
Double- stranded DNA (cccDNA). The cccDNA serves as template for all viral
transcripts, including a pregenome RNA. The pregenome RNA becomes
encapsidated with newly synthesized HBcAg. The viral polymerase
synthesizes by reverse transcription a negative-strand DNA copy. The
polymerase starts to synthesize the positive DNA strand, but the process is not
completed. Cores bud from the pre-Golgi membranes, acquiring HBsAg-
containing envelopes, and may exit the cell.

5
Hepatitis B virus other properties
•
HBV is sensitive to higher temperature and is killed rapidly after heating
at 100°C for 1 minute and at 60°C for 10 hours.
•
HBsAg is also destroyed by treatment with 0.5% sodium hypochlorite
within 3 minutes.
•
The virus by itself does not cause any cytopathic effect in the infected
liver cells.
•
The injury or cytopathic effects most probably occur as a result of cell-
mediated injury.
•
The formation of antigen–antibody complexes is responsible for some of
the symptoms, such as arthralgia, arthritis seen during early stage of the
disease.
•
Hepatitis B virus natural infection induces a lifelong immunity.
•
A chronic carrier stage with HBV infection is an important event in the
pathogenesis of HBV infection. A person with chronic carrier stage has
HBsAg persisting in the blood for at least 6 months. This stage is caused
by a persistent infection of the hepatocytes that leads to the presence of
HBV and HBsAg in the blood. This chronic carrier stage occurs in about
5% of patients with HBV infection.
•
Approximately 90% of the infected neonates become chronic carriers.
•
Approximately 20% of HBsAg carriers, nearly 1% of all adult patients
infected with HBV, and high percentage of neonates infected with the
virus progress to develop hepatocellular carcinoma or cirrhosis.
•
The hepatocellular carcinoma appears to be the result of persistent
cellular regeneration that tends to replace the dead hepatocytes. Also it is
suggested that the integration of HBV DNA with hepatocytes DNA could
activate a cellular oncogene, resulting in loss of control of the growth of
hepatocytes. However, the HBV genome has no oncogene, which can be
responsible directly for causing hepatocellular carcinoma.
Clinical Syndromes of Hepatitis B virus

6
Hepatitis B virus is one of the most important causes of acute and chronic
hepatitis. The clinical manifestations vary from subclinical hepatitis to
symptomatic and icteric hepatitis. The incubation period varies from 6 weeks
to 6 months. The clinical manifestations of HBV infection depend on (a ) age of
infection, (b ) immune status of the host, and (c ) the level of HBV.
Acute hepatitis B virus infection Is characterized by:-
• Gradual onset of anorexia, malaise, and fatigue, Nausea, vomiting, and
pruritus with passing of dark-colored urine are the symptoms noted in
this stage.
• Clinical manifestations of acute hepatitis B are similar to that of hepatitis
A but with the difference that the symptoms tend to be more severe and
life threatening with HBV infection.
Chronic hepatitis B virus infection: Is one of the major complications of HBV
infection.The risk of chronic infection is also higher in
•
Those infected at birth (90%).
•
In patients who are immunocompromised.
•
Only 5–10% of older children or adults progress to develop chronic
infection.
Complications of Hepatitis B virus infection
•
Cirrhosis and hepatocellular carcinoma are the long-term but rare
complications of hepatitis B. The cancer that develops an average of 25–
30 years after initial infection is the leading cause of cancer-related
deaths in areas where HBV is endemic.
Transmission of HBV infection
•
Individuals with chronic HBV infection are the major reservoir of HBV
infections. These people with HBeAg in their serum tend to have high
viral titers and thus greater infectivity. HBV is present at a high level in
serum. The virions are also present at very low levels in semen, vaginal
mucosa, saliva, and tears, and all are infectious.
The hepatitis B virus can be transmitted in the following ways:

7
•
Parenteral transmission: This transmission occurs due to transfusion of
HBV-infected blood and blood products.
•
Sexual transmission of HBV: Hepatitis B virus is transmitted sexually
more easily than Hepatitis C virus (HCV) or Hepatitis D virus (HDV).
•
Perinatal transmission: The transmission occurs from infected mother to
child due to contact with mother’s infected blood during the time of
delivery.
Laboratory Diagnosis
•
Serodiagnosis: Diagnosis of acute infection is made by demonstration of
HBsAg as well as HBeAg in the serum. They indicate viral replication.
•
When viral replication slows, HBeAg disappears and anti-HBeAg is
detected.
•
Hepatitis B surface antibody (HBsAb) produced may persist for many
years. This antigen appears in blood during incubation period and is
detectable in most patients during acute phase of the disease.
•
Persistent presence of HBsAg in blood for at least 6 months indicates the
carrier state and also indicates the risk of chronic hepatitis and hepatic
carcinoma.
•
HBsAg and hepatitis B e antigen (HBeAg) are the first markers
identified in the serum of patients acutely infected with HBV. HBeAg is
generally considered to be a marker of HBV replication and infectivity.
Molecular Diagnosis
HBV PCR for demonstration of HBV DNA is highly valuable to monitor the
treatment of chronic HBV infection with antiviral therapy. This is also useful
to identify HBV as the cause of liver infection in HBsAg-negative patients. The
detection of viral DNA in the serum indicates acute infection.
Other biochemical tests
•
These tests include elevation of Alanine Aminotransferase (ALT) and
Aspartate aminotransferase (AST). High levels are found in acute
hepatitis (1000–2000 IU/mL).
•
Estimation of serum bilirubin indicates the intensity of jaundice.
Vaccines : WHO recommends that all infants should receive their first dose of
vaccine as soon as possible after birth, preferably within 24 hours.

8
******************************************************************************
Hepatitis C Virus
•
Morphology
•
Hepatitis C virus is the only member of the genus Hepacivirus in the
family Flaviviridae of RNA-containing virus.
•
Most patients infected with HCV have chronic liver disease, which
progresses to cirrhosis and hepatocellular carcinoma.
•
It is a spherical, enveloped, 9.4 kb, single-stranded RNA virus with a
diameter of 55 nm. The genome is approximately 9500 base pairs that
encode 10 structural and regulatory proteins.
•
Structural proteins include the core and two envelope proteins, namely,
E1 and E2.
•
The viruses are ether sensitive and acid sensitive.
Hepatitis C Virus replication
1. Attachment of the viral envelope protein E to host receptors mediates
internalization into the host cell by endocytosis.
2. The positive-sense genomic ssRNA is translated into a polyprotein, which
is cleaved into all structural and non structural proteins .
3. Replication takes place at the surface of endoplasmic reticulum in
cytoplasmic viral factories. A dsRNA genome is synthesized from the
genomic ssRNA(+).
4. 4.The dsRNA genome is transcribed thereby providing viral mRNAs/new
ssRNA(+) genomes.
5. 5.Virus assembly occurs at the endoplasmic reticulum.
6. 6.The virion buds at the ER and is transported to the Golgi apparatus.
7. Release of new virions by exocytosis.
Clinical Syndromes Hepatitis C virus can cause:
(a ) Acute HCV infection.
(b ) Chronic HCV infection.
(c ) Cirrhosis and other complications induced by hepatitis. The incubation
period of hepatitis C varies from 15 to 60 days with an average period of
approximately 8 weeks.
Pathogenesis and clinical picture

9
Hepatitis C resembles hepatitis B in many aspects. One major difference is that
a. It much more frequently produces a persistent infection (85 %) and, in
70% of cases, develops into a chronic hepatitis.
b. Resulting in cirrhosis of the liver within 20 years and a hepatocellular
carcinoma (HCC) in a further 10 years. The reason for the high level of
viral persistence is thought to be a pronounced mutability facilitating
evasion of the immune defenses.
Diagnosis
• Diagnosis of hepatitis C is done with antibody immunoassay (EIA) like
ELISA using genetically engineered viral proteins. Western blot can be
used to confirm the result.
• The RNA can be detected by means of RT-PCR and is the most specific test
for HCV infection and useful in diagnosing acute HCV infections before
antibodies are developed and the course of therapy can be monitored
with quantitative PCR.
Transmission and prevention: Transmission is by:
Blood and blood products. High-risk persons include dialysis patients, healthcare
staff, and needle-sharing drug consumers. Perinatal transmission is possible.