208
DIVISIONS OF THE GUT TUBE
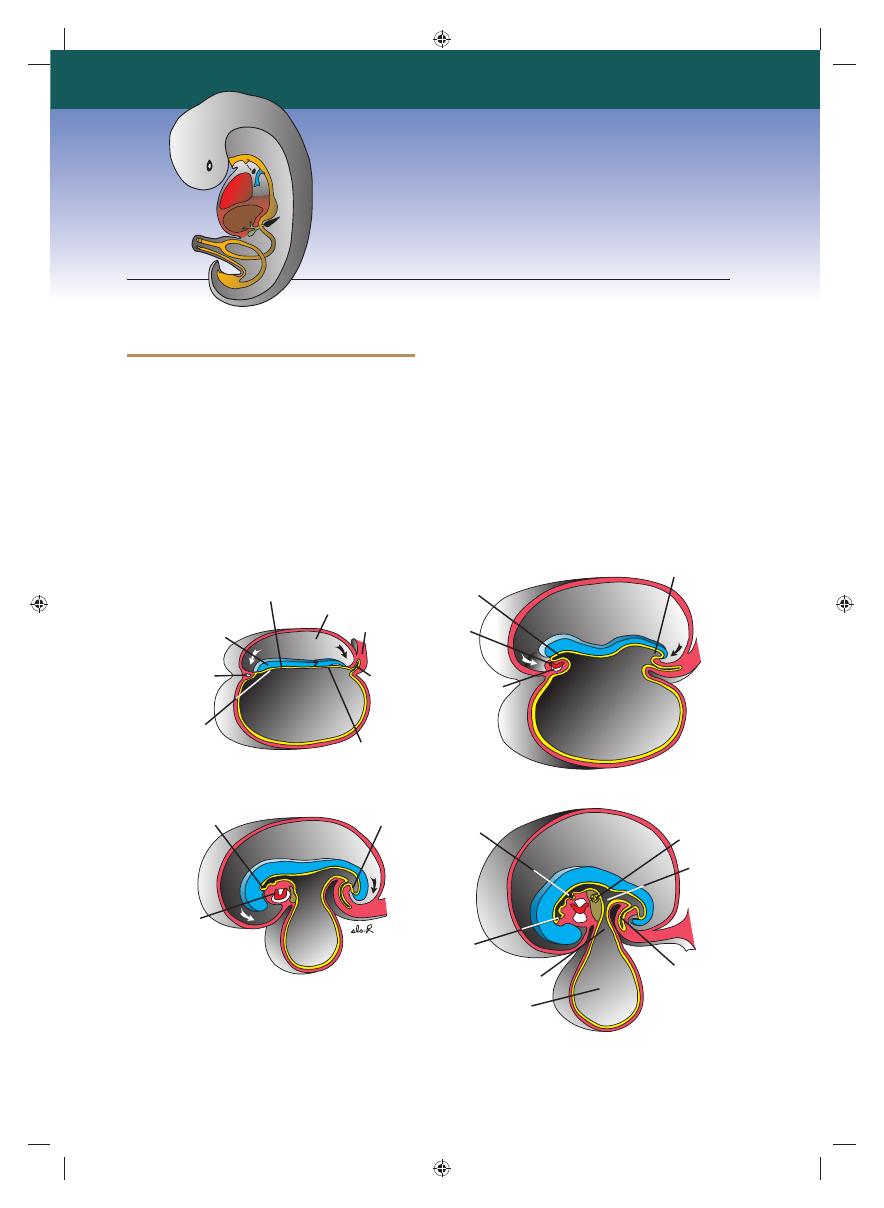
As a result of cephalocaudal and lateral folding
of the embryo, a portion of the endoderm-lined
yolk sac cavity is incorporated into the embryo
to form the primitive gut. Two other por-
tions of the endoderm-lined cavity, the yolk sac
and the allantois, remain outside the embryo
(Fig. 15.1A–D).
In the cephalic and caudal parts of the embryo,
the primitive gut forms a blind-ending tube, the
foregut
and hindgut, respectively. The middle
part, the midgut, remains temporally connected
to the yolk sac by means of the vitelline duct, or
yolk stalk
(Fig. 15.1D).
Development of the primitive gut and its
derivatives is usually discussed in four sections: (a)
The pharyngeal gut, or pharynx, extends from
the oropharyngeal membrane to the respiratory
diverticulum and is part of the foregut; this sec-
tion is particularly important for development of
the head and neck and is discussed in Chapter 17.
(b) The remainder of the foregut lies caudal to
the pharyngeal tube and extends as far caudally as
the liver outgrowth. (c) The midgut begins cau-
dal to the liver bud and extends to the junction
Chapter
15
Digestive System
Ectoderm
Angiogenic
cell cluster
Amniotic cavity
Endoderm
Connecting
stalk
Allantois
Cloacal
membrane
Foregut
Pericardial
cavity
Heart
tube
Hindgut
Remnant
of the
oropharyngeal
membrane
Cloacal
membrane
Heart
tube
Oropharyngeal
membrane
Vitelline duct
Lung bud
Liver
bud
Midgut
Allantois
Yolk sac
A
C
B
D
Oropharyngeal
membrane
Figure 15.1
Sagittal sections through embryos at various stages of development demonstrating the effect of cephalocau-
dal and lateral folding on the position of the endoderm-lined cavity. Note formation of the foregut, midgut, and hindgut.
A. Presomite embryo. B. Embryo with seven somites. C. Embryo with 14 somites. D. At the end of the fi rst month.
Sadler_Chap15.indd 208
Sadler_Chap15.indd 208
8/26/2011 7:21:25 AM
8/26/2011 7:21:25 AM
Chapter 15 Digestive System
209
of the right two-thirds and left third of the trans-
verse colon in the adult. (d) The hindgut extends
from the left third of the transverse colon to the
cloacal membrane (Fig. 15.1). Endoderm forms
the epithelial lining of the digestive tract and
gives rise to the specifi c cells (the parenchyma)
of glands, such as hepatocytes and the exocrine
and endocrine cells of the pancreas. The stroma
(connective tissue) for the glands is derived from
visceral mesoderm. Muscle, connective tissue,
and peritoneal components of the wall of the gut
also are derived from visceral mesoderm.
MOLECULAR REGULATION OF
GUT TUBE DEVELOPMENT
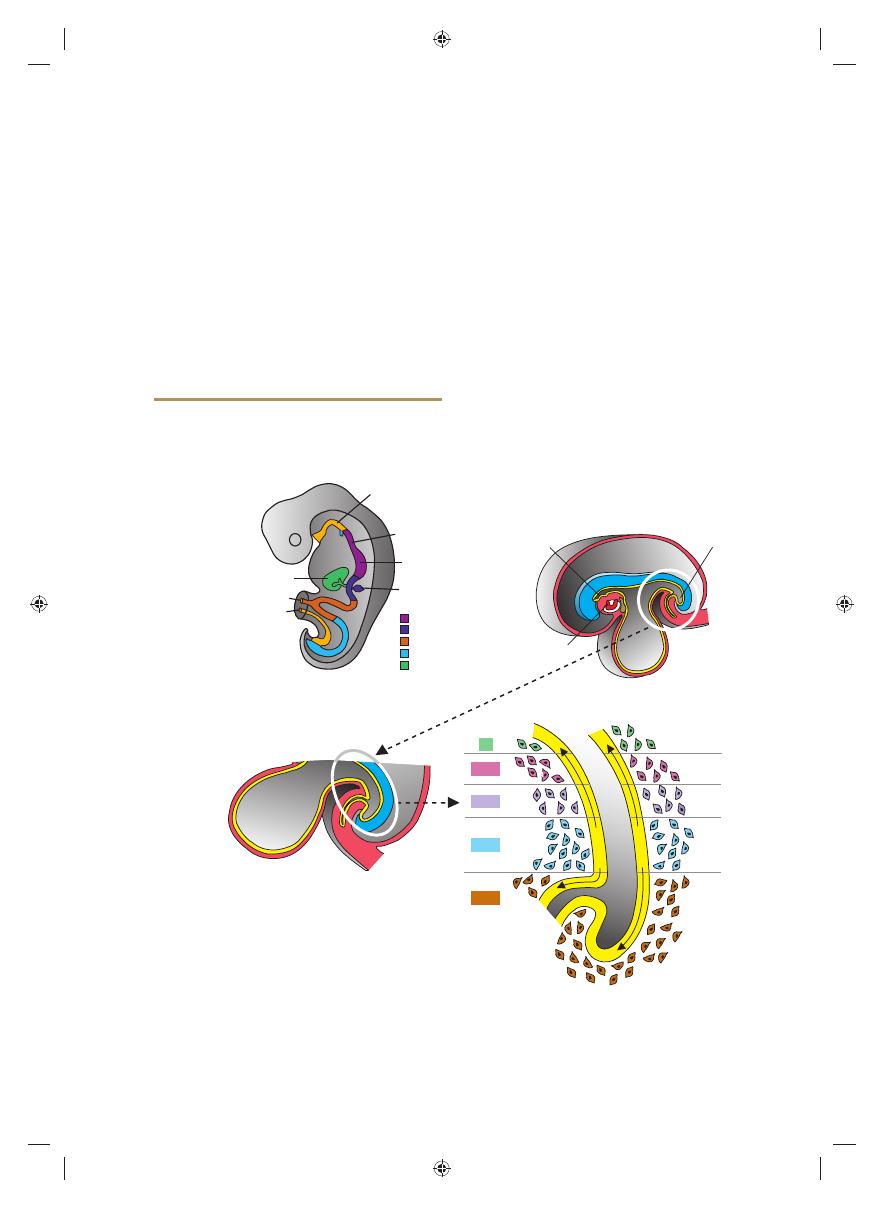
Regional specifi cation of the gut tube into differ-
ent components occurs during the time that the
lateral body folds are bringing the two sides of the
tube together (Figs. 15.2 and 15.3). Specifi cation
is initiated by a concentration gradient of retinoic
acid (RA) from the pharynx, that is exposed to
little or no RA, to the colon, that sees the highest
concentration of RA. This RA gradient causes
transcription factors to be expressed in different
regions of the gut tube. Thus, SOX2 “specifi es”
the esophagus and stomach; PDX1, the duode-
num; CDXC, the small intestine; and CDXA,
the large intestine and rectum (Fig. 15.2A).
This initial patterning is stabilized by reciprocal
interactions between the endoderm and visceral
mesoderm adjacent to the gut tube (Fig. 15.2B–
D). This epithelial–mesenchymal interaction
is initiated by sonic hedgehog (SHH) expres-
sion throughout the gut tube. SHH expression
upregulates factors in the mesoderm that then
determine the type of structure that forms from
the gut tube, such as the stomach, duodenum,
9-10
9
9-11
9-12
9-13
S
H
H
S
H
H
Hindgut
Heart
tube
Foregut
small
intestine
cecum
large
intestine
cloaca
HOX
Allantois
A
C
D
B
Vitelline duct
Liver
Pancreas
CSOX2
PDX1
CDXC
CDXA
HOX
Stomach
Esophagus
Pharyngeal gut
Figure 15.2
Diagrams showing molecular regulation of gut development. A. Color-coded diagram that indicates genes
responsible for initiating regional specifi cation of the gut into esophagus, stomach, duodenum, etc. B-D. Drawings showing
an example from the midgut and hindgut regions indicating how early gut specifi cation is stabilized. Stabilization is effected
by epithelial–mesenchymal interactions between gut endoderm and surrounding visceral (splanchnic) mesoderm. Endoderm
cells initiate the stabilization process by secreting SHH, which establishes a nested expression of HOX genes in the meso-
derm. This interaction results in a genetic cascade that regulates specifi cation of each gut region as is shown for the small
and large intestine regions in these diagrams.
Sadler_Chap15.indd 209
Sadler_Chap15.indd 209
8/26/2011 7:21:25 AM
8/26/2011 7:21:25 AM
210
Part II Systems-Based Embryology
enclose an organ and connect it to the body wall.
Such organs are called intraperitoneal, whereas
organs that lie against the posterior body wall and
are covered by peritoneum on their anterior sur-
face only (e.g., the kidneys) are considered retro-
peritoneal. Peritoneal ligaments
are double
layers of peritoneum (mesenteries) that pass from
one organ to another or from an organ to the
body wall. Mesenteries and ligaments provide
pathways for vessels, nerves, and lymphatics to
and from abdominal viscera (Figs. 15.3 and 15.4).
Initially the foregut, midgut, and hindgut are
in broad contact with the mesenchyme of the
posterior abdominal wall (Fig. 15.3). By the fi fth
week, however, the connecting tissue bridge has
small intestine, etc. For example, in the region
of the caudal limit of the midgut and all of the
hindgut, SHH expression establishes a nested
expression of the HOX genes in the mesoderm
(Fig. 15.2D). Once the mesoderm is specifi ed by
this code, then it instructs the endoderm to form
the various components of the mid- and hindgut
regions, including part of the small intestine,
cecum, colon, and cloaca (Fig. 15.2).
MESENTERIES
Portions of the gut tube and its derivatives are sus-
pended from the dorsal and ventral body wall by
mesenteries
, double layers of peritoneum that
Amnionic cavity
Surface ectoderm
Gut
Dorsal
mesentery
Intra-
embryonic
body cavity
Connection
between
gut and yolk sac
Visceral
mesoderm
Parietal
mesoderm
Yolk sac
A
B
C
Figure 15.3
Transverse sections through embryos at various stages of development. A. The intraembryonic cavity,
bordered by visceral and somatic layers of lateral plate mesoderm, is in open communication with the extraembryonic cavity.
B. The intraembryonic cavity is losing its wide connection with the extraembryonic cavity. C. At the end of the fourth week,
visceral mesoderm layers are fused in the midline and form a double-layered membrane (dorsal mesentery) between right
and left halves of the body cavity. Ventral mesentery exists only in the region of the septum transversum (not shown).
Celiac artery
Dorsal mesogastrium
Bare area of liver
Diaphragm
Falciform ligament
Vitelline duct
Allantois
Cloaca
Umbilical artery
Lesser
omentum
Dorsal mesocolon
Dorsal mesoduodenum
Superior mesenteric artery
Inferior mesenteric artery
Mesentery proper
Figure 15.4
Primitive dorsal and ventral mesenteries. The liver is connected to the ventral abdominal wall and to the
stomach by the falciform ligament and lesser omentum, respectively. The superior mesenteric artery runs through the mes-
entery proper and continues toward the yolk sac as the vitelline artery.
Sadler_Chap15.indd 210
Sadler_Chap15.indd 210
8/26/2011 7:21:26 AM
8/26/2011 7:21:26 AM
Chapter 15 Digestive System
211
ventral mesentery into (a) the lesser omentum,
extending from the lower portion of the esopha-
gus, the stomach, and the upper portion of the
duodenum to the liver and (b) the falciform
ligament
, extending from the liver to the ventral
body wall (Fig. 15.4; see Chapter 7).
FOREGUT
Esophagus
When the embryo is approximately 4 weeks old,
the respiratory diverticulum (lung bud)
appears at the ventral wall of the foregut at the
border with the pharyngeal gut (Fig. 15.5). The
tracheoesophageal septum
gradually parti-
tions this diverticulum from the dorsal part of
the foregut (Fig. 15.6). In this manner, the foregut
narrowed, and the caudal part of the foregut,
the midgut, and a major part of the hindgut are
suspended from the abdominal wall by the dor-
sal mesentery
(Figs. 15.3C and 15.4), which
extends from the lower end of the esophagus to
the cloacal region of the hindgut. In the region of
the stomach, it forms the dorsal mesogastrium
or greater omentum; in the region of the duo-
denum, it forms the dorsal mesoduodenum;
and in the region of the colon, it forms the dor-
sal mesocolon.
Dorsal mesentery of the jejunal
and ileal loops forms the mesentery proper.
Ventral mesentery
, which exists only in the
region of the terminal part of the esophagus, the
stomach, and the upper part of the duodenum
(Fig. 15.4), is derived from the septum trans-
versum.
Growth of the liver into the mesen-
chyme of the septum transversum divides the
A
B
Hindgut
Cloaca
Proctodeum
Allantois
Vitelline duct
Gallbladder
Liver
Stomodeum
Cloacal
membrane
Urinary
bladder
Heart
bulge
Pharyngeal
pouches
Esophagus
Pancreas
Stomach
Esophagus
Tracheo-
bronchial
diverticulum
Pharyngeal gut
Primitive
intestinal
loop
Figure 15.5
Embryos during the fourth A and fi fth B weeks of development showing formation of the gastrointesti-
nal tract and the various derivatives originating from the endodermal germ layer.
Tracheoesophageal
septum
Foregut
A
B
C
Pharynx
Trachea
Lung buds
Esophagus
Respiratory
diverticulum
Figure 15.6
Successive stages in development of the respiratory diverticulum and esophagus through partitioning of the
foregut. A. At the end of the third week (lateral view). B,C. During the fourth week (ventral view).
Sadler_Chap15.indd 211
Sadler_Chap15.indd 211
8/26/2011 7:21:26 AM
8/26/2011 7:21:26 AM
A
E
B
D
C
Trachea
Bifurcation
Bronchi
Tracheoesophageal
fistula
Distal part of
esophagus
Proximal blind-
end part of
esophagus
Communication
of esophagus
with trachea
Sadler_Chap15.indd 212
Sadler_Chap15.indd 212
8/26/2011 7:21:27 AM
8/26/2011 7:21:27 AM
Chapter 15 Digestive System
213
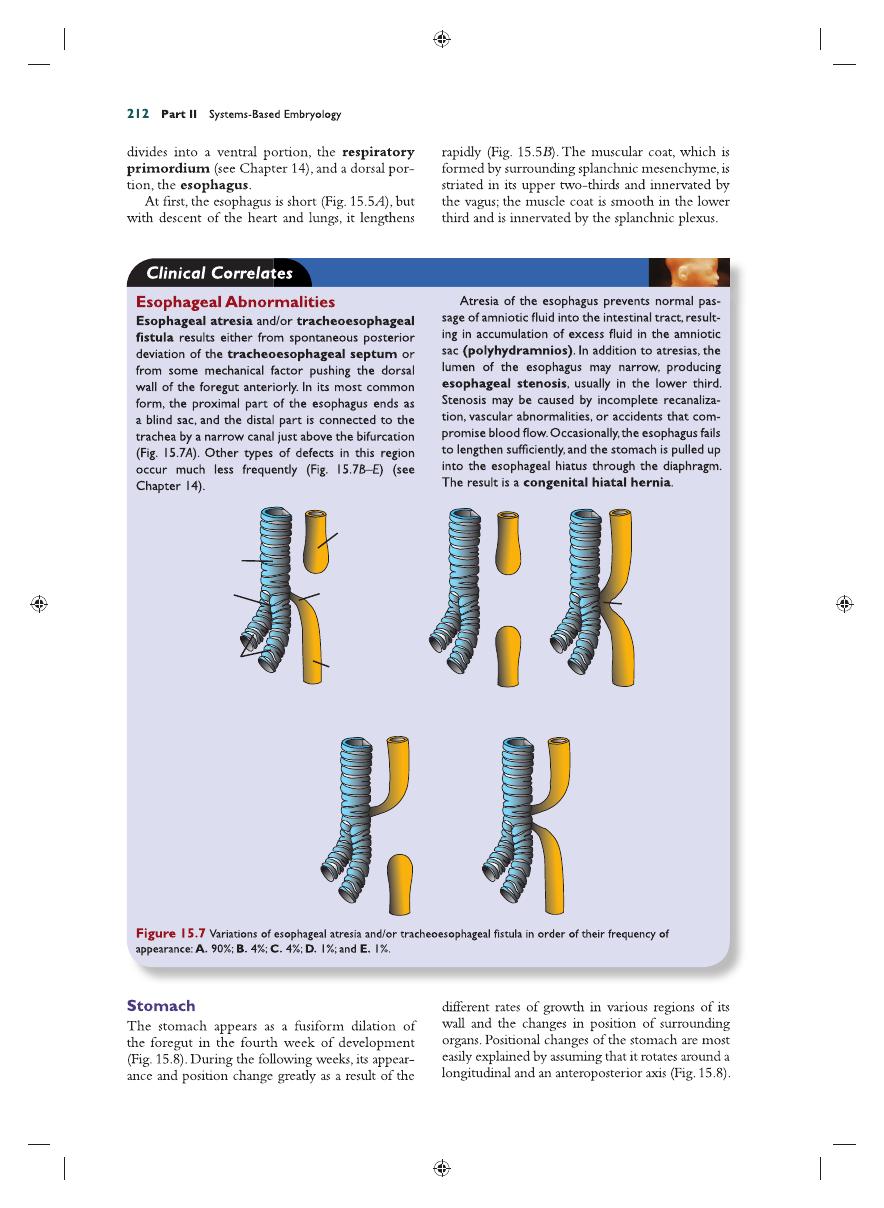
The stomach rotates 90° clockwise around its
longitudinal axis, causing its left side to face ante-
riorly and its right side to face posteriorly (Fig.
15.8A–C). Hence, the left vagus nerve, initially
innervating the left side of the stomach, now
innervates the anterior wall; similarly, the right
nerve innervates the posterior wall. During this
rotation, the original posterior wall of the stomach
grows faster than the anterior portion, forming
the greater and lesser curvatures (Fig. 15.8C).
The cephalic and caudal ends of the stomach
originally lie in the midline, but during further
growth, the stomach rotates around an antero-
posterior axis, such that the caudal or pyloric
part
moves to the right and upward, and the
cephalic or cardiac portion moves to the left
and slightly downward (Fig. 15.8D,E). The stom-
ach thus assumes its fi nal position, its axis running
from above left to below right.
Since the stomach is attached to the dorsal
body wall by the dorsal mesogastrium and
to the ventral body wall by the ventral meso-
gastrium
(Figs. 15.4 and 15.9A), its rotation
and disproportionate growth alter the position
of these mesenteries. Rotation about the lon-
gitudinal axis pulls the dorsal mesogastrium to
the left, creating a space behind the stomach
called the omental bursa (lesser peritoneal
sac)
(Figs. 15.9 and 15.10). This rotation also
pulls the ventral mesogastrium to the right.
As this process continues in the fi fth week of
development, the spleen primordium appears
as a mesodermal proliferation between the
two leaves of the dorsal mesogastrium (Figs.
15.10 and 15.11). With continued rotation of
the stomach, the dorsal mesogastrium length-
ens, and the portion between the spleen and
dorsal midline swings to the left and fuses with
the peritoneum of the posterior abdominal
wall (Figs. 15.10 and 15.11). The posterior leaf
of the dorsal mesogastrium and the perito-
neum along this line of fusion degenerate. The
spleen, which remains intraperitoneal, is then
connected to the body wall in the region of
the left kidney by the lienorenal ligament
and to the stomach by the gastrolienal liga-
ment
(Figs. 15.10 and 15.11). Lengthening and
fusion of the dorsal mesogastrium to the poste-
rior body wall also determine the fi nal position
of the pancreas. Initially, the organ grows into
the dorsal mesoduodenum, but eventually its
tail extends into the dorsal mesogastrium (Fig.
15.10A). Since this portion of the dorsal meso-
gastrium fuses with the dorsal body wall, the
B
A
C
Longitudinal
rotation axis
Stomach
Lesser
curvature
Greater
curvature
Duodenum
Esophagus
D
E
Anteroposterior
axis
Lesser
curvature
Greater
curvature
Greater
curvature
Pylorus
Figure 15.8
A–C. Rotation of the stomach along its longitudinal axis as seen anteriorly. D,E. Rotation of the stomach
around the anteroposterior axis. Note the change in position of the pylorus and cardia.
Sadler_Chap15.indd 213
Sadler_Chap15.indd 213
8/26/2011 7:21:29 AM
8/26/2011 7:21:29 AM
214
Part II Systems-Based Embryology
Stomach
Dorsal mesogastrium
Small
vacuoles
Lesser
omentum
A
B
C
Omental
bursa
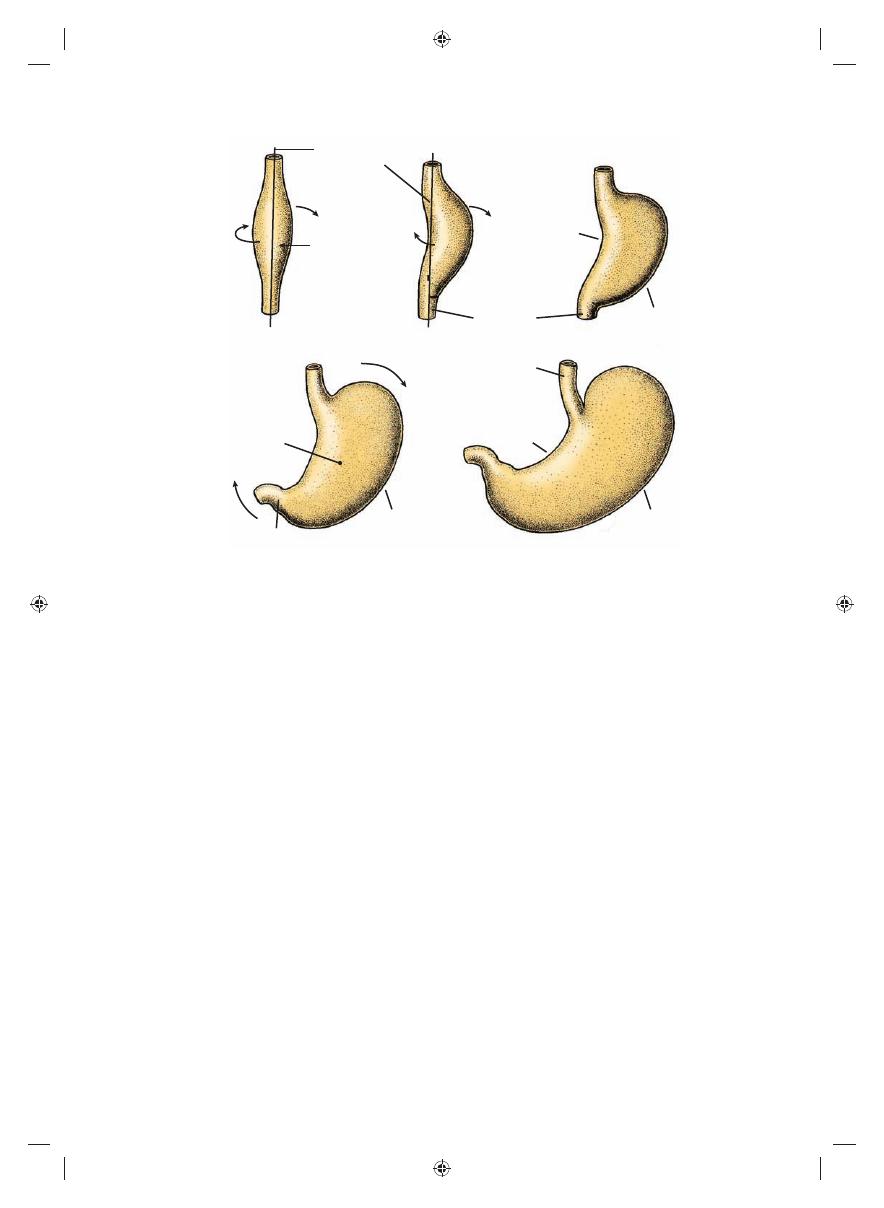
Figure 15.9
A. Transverse section through a 4-week embryo showing intercellular clefts appearing in the dorsal mesogas-
trium. B,C. The clefts have fused, and the omental bursa is formed as an extension of the right side of the intraembryonic
cavity behind the stomach.
Umbilical
vein
Gastrolienal
ligament
Omental
bursa
Lienorenal
ligament
Lesser
omentum
Liver
Falciform
ligament
Dorsal
pancreas
Dorsal
mesogastrium
Spleen
Stomach
Lesser omentum
Liver
Falciform ligament
A
B
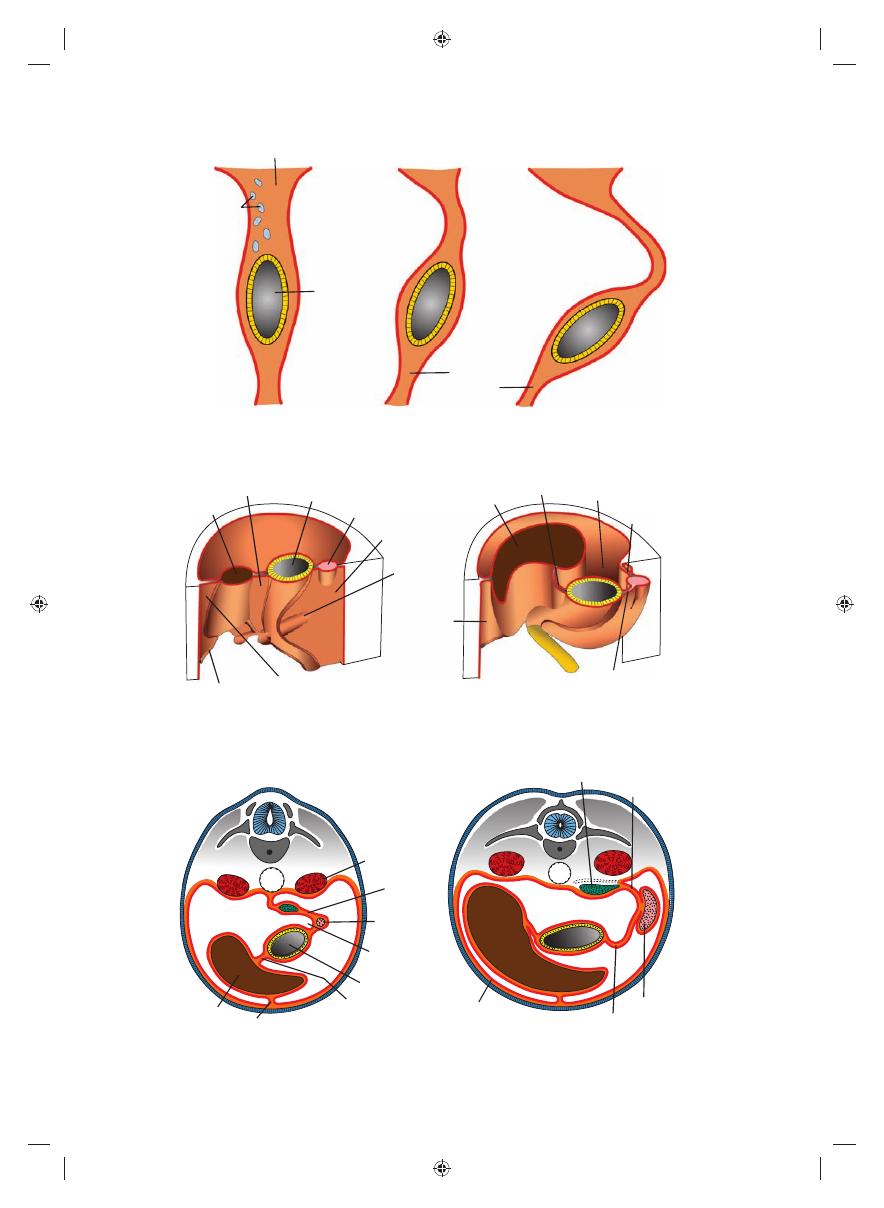
Figure 15.10
A. The positions of the spleen, stomach, and pancreas at the end of the fi fth week. Note the position of the
spleen and pancreas in the dorsal mesogastrium. B. Position of spleen and stomach at the 11th week. Note formation of the
omental bursa (lesser peritoneal sac).
Liver
Spleen
Gastrolienal ligament
Parietal
peritoneum
of body wall
Lienorenal
ligament
Pancreas
Kidney
Dorsal
mesogastrium
Spleen
Omental
bursa
Stomach
Lesser omentum
Falciform ligament
A
B
Figure 15.11
Transverse sections through the region of the stomach, liver, and spleen, showing formation of the omental
bursa (lesser peritoneal sac), rotation of the stomach, and position of the spleen and tail of the pancreas between the two
leaves of the dorsal mesogastrium. With further development, the pancreas assumes a retroperitoneal position.
Sadler_Chap15.indd 214
Sadler_Chap15.indd 214
8/26/2011 7:21:30 AM
8/26/2011 7:21:30 AM
Chapter 15 Digestive System
215
down and forms a double-layered sac extend-
ing over the transverse colon and small intestinal
loops like an apron (Fig. 15.13A). This double-
leafed apron is the greater omentum; later, its
layers fuse to form a single sheet hanging from the
greater curvature of the stomach (Fig. 15.13B).
The posterior layer of the greater omentum also
fuses with the mesentery of the transverse colon
(Fig. 15.13B).
The lesser omentum and falciform liga-
ment
form from the ventral mesogastrium,
which itself is derived from mesoderm of the
septum transversum. When liver cords grow into
the septum, it thins to form (a) the peritoneum
tail of the pancreas lies against this region (Fig.
15.11). Once the posterior leaf of the dorsal
mesogastrium and the peritoneum of the pos-
terior body wall degenerate along the line of
fusion, the tail of the pancreas is covered by
peritoneum on its anterior surface only and
therefore lies in a retroperitoneal position.
(Organs, such as the pancreas, that are originally
covered by peritoneum, but later fuse with the
posterior body wall to become retroperitoneal,
are said to be secondarily retroperitoneal.)
As a result of rotation of the stomach about
its anteroposterior axis, the dorsal mesogastrium
bulges down (Fig. 15.12). It continues to grow
Greater curvature
of stomach
Greater
omentum
Descending
colon
Ascending
colon
Sigmoid
Duodenum
Esophagus
Dorsal
mesogastrium
Omental
bursa
Mesoduodenum
Mesocolon
Mesentery
proper
Appendix
A
B
Figure 15.12
A. Derivatives of the dorsal mesentery at the end of the third month. The dorsal mesogastrium bulges out
on the left side of the stomach, where it forms part of the border of the omental bursa. B. The greater omentum hangs
down from the greater curvature of the stomach in front of the transverse colon.
Greater
omentum
Omental
bursa
Greater omentum
Small intestinal loop
Mesentery
of transverse
colon
Duodenum
Pancreas
Peritoneum
of posterior
abdominal wall
Stomach
Omental
bursa
B
A
Figure 15.13
A. Sagittal section showing the relation of the greater omentum, stomach, transverse colon, and small intes-
tinal loops at 4 months. The pancreas and duodenum have already acquired a retroperitoneal position. B. Similar section as in
A in the newborn. The leaves of the greater omentum have fused with each other and with the transverse mesocolon. The
transverse mesocolon covers the duodenum, which fuses with the posterior body wall to assume a retroperitoneal position.
Sadler_Chap15.indd 215
Sadler_Chap15.indd 215
8/26/2011 7:21:31 AM
8/26/2011 7:21:31 AM
216
Part II Systems-Based Embryology
free margin of the lesser omentum connecting
the duodenum and liver (hepatoduodenal
ligament)
contains the bile duct, portal vein,
and hepatic artery (portal triad). This free
margin also forms the roof of the epiploic
foramen of Winslow
, which is the opening
connecting the omental bursa (lesser sac) with
the rest of the peritoneal cavity (greater sac)
(Fig. 15.16).
of the liver; (b) the falciform ligament,
extending from the liver to the ventral body
wall; and (c) the lesser omentum, extending
from the stomach and upper duodenum to the
liver (Figs. 15.14 and 15.15). The free margin
of the falciform ligament contains the umbili-
cal vein (Fig. 15.10A), which is obliterated
after birth to form the round ligament of
the liver (ligamentum teres hepatis)
. The
Respiratory
diverticulum
Heart
Vitelline
duct
Allantois
Cloacal
membrane
A
B
Hindgut
Liver bud
Duodenum
Midgut
Stomach
Septum
transversum
Liver
Cloaca
Duodenum
Stomach
Esophagus
Larynx
Primary
intestinal
loop
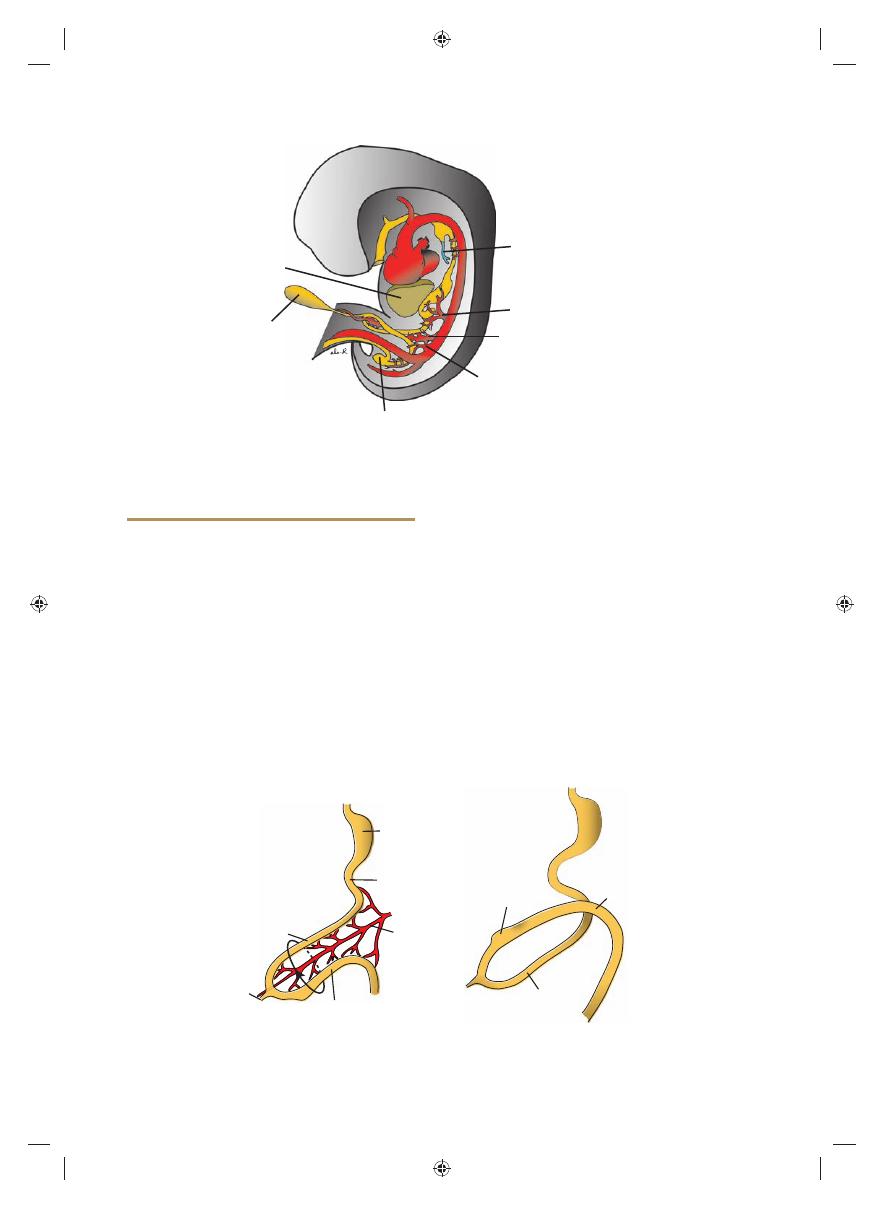
Figure 15.14
A. A 3-mm embryo (approximately 25 days) showing the primitive gastrointestinal tract and formation of
the liver bud. The bud is formed by endoderm lining the foregut. B. A 5-mm embryo (approximately 32 days). Epithelial liver
cords penetrate the mesenchyme of the septum transversum.
A
B
Hindgut
Vitelline
duct
Allantois
Liver
Cloacal membrane
Septum
transversum
Pericardial
cavity
Stomach
Gallbladder
Pancreas
Dorsal
mesogastrium
Lesser
omentum
Bare area of liver
Esophagus
Tracheobronchial
diverticulum
Thyroid
Diaphragm
Falciform
ligament
Gallbladder
Tongue
Pancreas
Duodenum
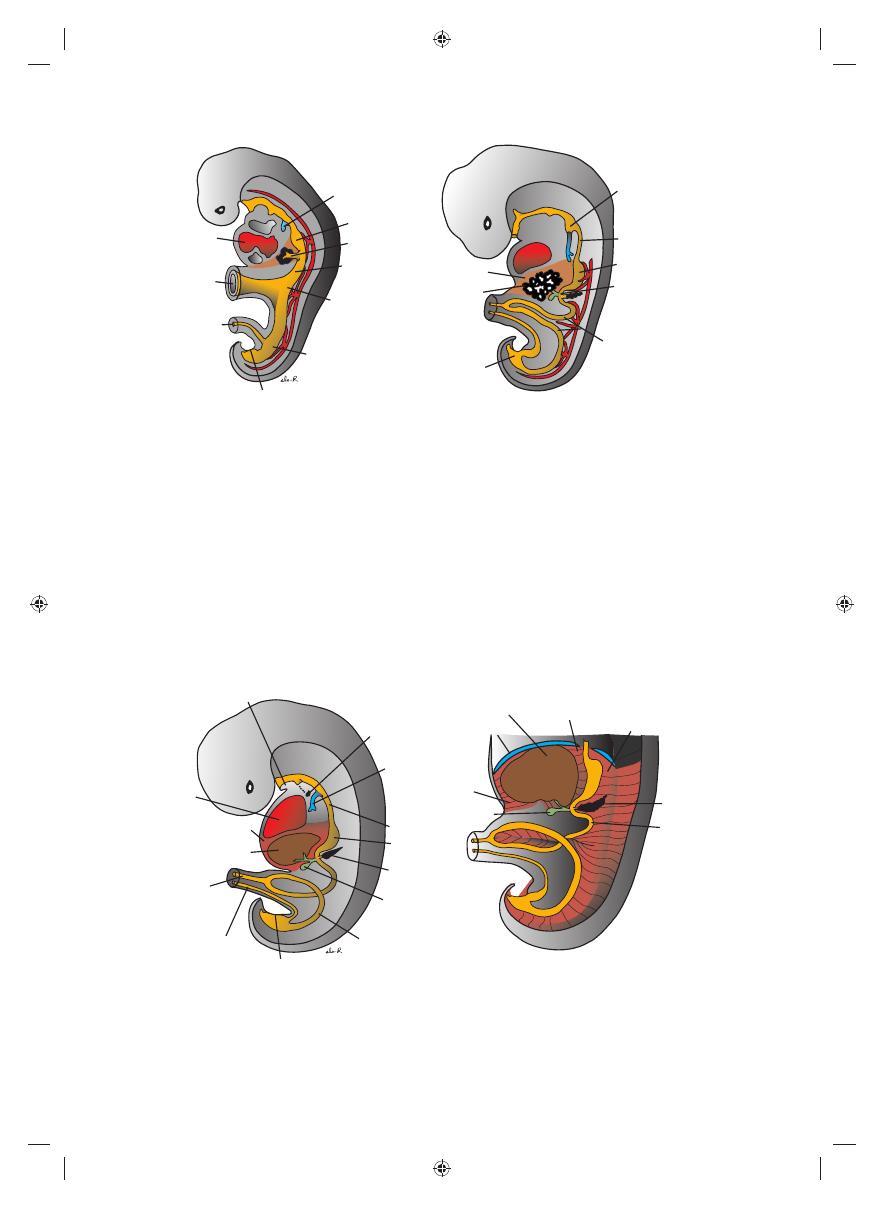
Figure 15.15
A. A 9-mm embryo (approximately 36 days). The liver expands caudally into the abdominal cavity. Note
condensation of mesenchyme in the area between the liver and the pericardial cavity, foreshadowing formation of the
diaphragm from part of the septum transversum. B. A slightly older embryo. Note the falciform ligament extending between
the liver and the anterior abdominal wall and the lesser omentum extending between the liver and the foregut (stomach
and duodenum). The liver is entirely surrounded by peritoneum except in its contact area with the diaphragm. This is the
bare area of the liver.
Sadler_Chap15.indd 216
Sadler_Chap15.indd 216
8/26/2011 7:21:31 AM
8/26/2011 7:21:31 AM
Lesser
omentum
Esophagus
Stomach
Diaphragm
Greater omentum,
gastrocolic portion
Anastomosis between
right and left gastro-
omental (epiploic)
arteries
Transverse colon appearing
in an unusual gap in the
greater omentum
Transversus
abdominis
11th costal
cartilage
10th rib
Costodiaphragmatic
recess
Gallbladder
Duodenum
Omental (epiploic)
foramen
Porta hepatis
7th rib
Liver Falciform ligament
Sadler_Chap15.indd 217
Sadler_Chap15.indd 217
8/26/2011 7:21:32 AM
8/26/2011 7:21:32 AM
218
Part II Systems-Based Embryology
with the vitelline and umbilical veins, which
form hepatic sinusoids. Liver cords differentiate
into the parenchyma (liver cells) and form
the lining of the biliary ducts. Hematopoietic
cells, Kupffer cells
, and connective tissue
cells
are derived from mesoderm of the septum
transversum.
When liver cells have invaded the entire sep-
tum transversum, so that the organ bulges cau-
dally into the abdominal cavity, mesoderm of
the septum transversum lying between the liver
and the foregut and the liver and the ventral
abdominal wall becomes membranous, forming
the lesser omentum and falciform ligament,
respectively. Together, having formed the peri-
toneal connection between the foregut and the
ventral abdominal wall, they are known as the
ventral mesentery
(Fig. 15.15).
Mesoderm on the surface of the liver dif-
ferentiates into visceral peritoneum except on
its cranial surface (Fig. 15.15B). In this region,
the liver remains in contact with the rest of the
original septum transversum. This portion of
the septum, which consists of densely packed
mesoderm, will form the central tendon of the
diaphragm
. The surface of the liver that is in
contact with the future diaphragm is never cov-
ered by peritoneum; it is the bare area of the
liver
(Fig. 15.15).
In the 10th week of development, the
weight of the liver is approximately 10% of the
total body weight. Although this may be attrib-
uted partly to the large numbers of sinusoids,
another important factor is its hematopoietic
function
. Large nests of proliferating cells,
which produce red and white blood cells, lie
between hepatic cells and walls of the vessels.
This activity gradually subsides during the last
(Figs. 15.14 and 15.15). This outgrowth, the
hepatic diverticulum
, or liver bud, consists
of rapidly proliferating cells that penetrate the
septum transversum
, that is, the mesodermal
plate between the pericardial cavity and the
stalk of the yolk sac (Figs. 15.14 and 15.15).
While hepatic cells continue to penetrate the
septum, the connection between the hepatic
diverticulum and the foregut (duodenum) nar-
rows, forming the bile duct. A small ventral
outgrowth is formed by the bile duct, and this
outgrowth gives rise to the gallbladder and
the cystic duct (Figs. 15.15). During further
development, epithelial liver cords intermingle
Parietal
peritoneum
Duodenum
Dorsal
mesoduodenum
Kidney
B
A
Pancreas
Pancreas and
duodenum in
retroperitoneal
position
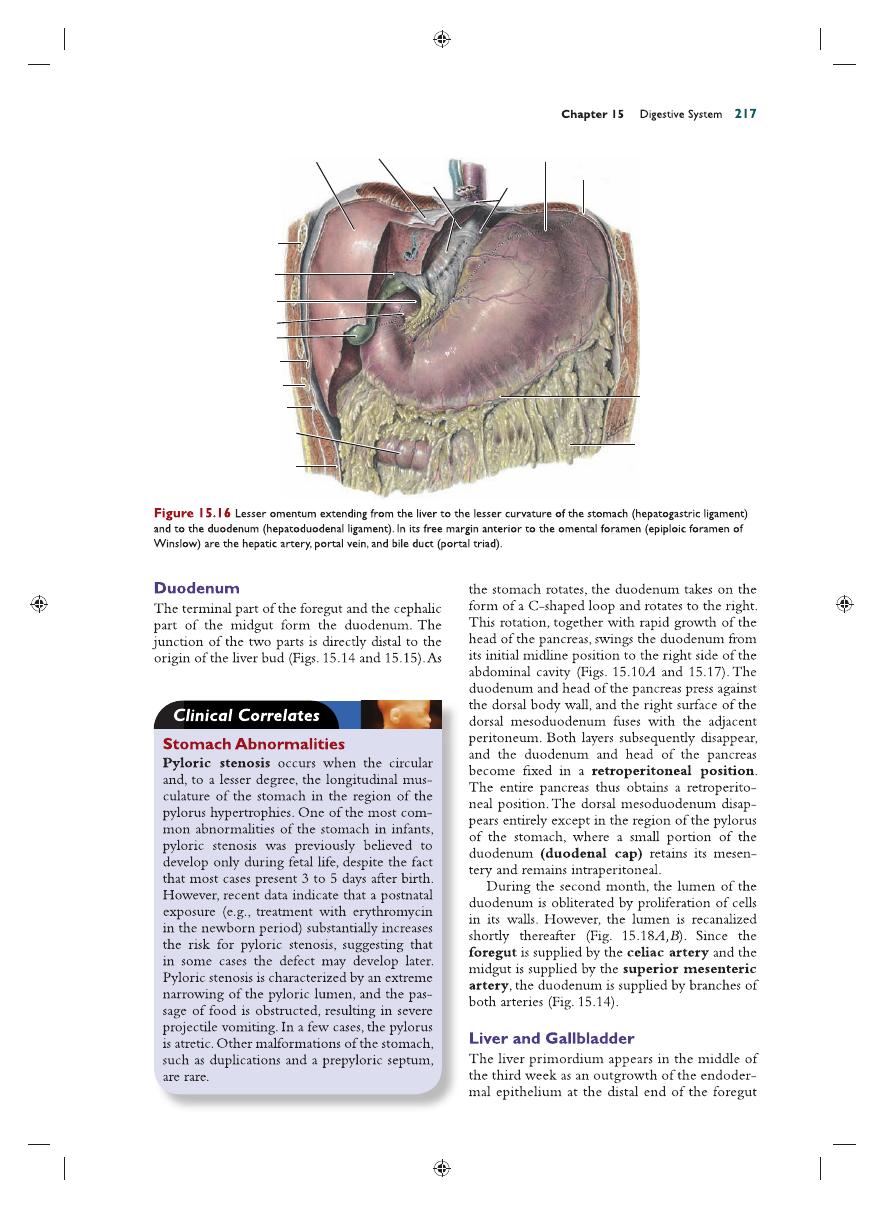
Figure 15.17
Transverse sections through the region of the duodenum at various stages of development. At fi rst, the
duodenum and head of the pancreas are located in the median plane. A, but later, they swing to the right and acquire a
retroperitoneal position. B.
Cavity
formation
Recanalization
Solid stage
A
B
Figure 15.18
Upper portion of the duodenum showing
the solid stage. A and cavity formation. B produced by
recanalization.
Sadler_Chap15.indd 218
Sadler_Chap15.indd 218
8/26/2011 7:21:37 AM
8/26/2011 7:21:37 AM
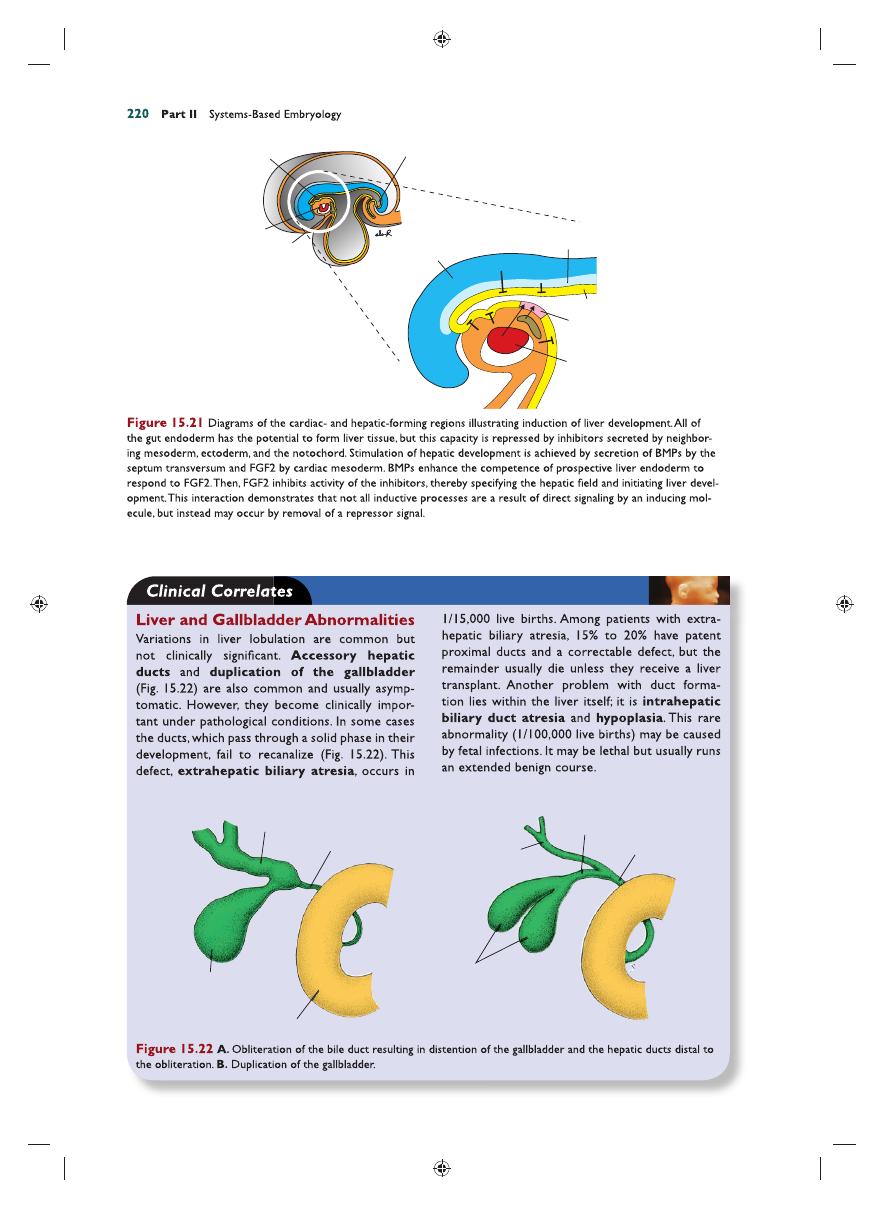
Chapter 15 Digestive System
219
blocked by factors produced by surrounding tis-
sues, including ectoderm, noncardiac mesoderm,
and particularly the notochord (Fig. 15.21).
The action of these inhibitors is blocked in
the prospective hepatic region by fi broblast
growth factors (FGF2)
secreted by cardiac
mesoderm and by blood vessel-forming endo-
thelial cells adjacent to the gut tube at the site
of liver bud outgrowth. Thus, the cardiac meso-
derm together with neighboring vascular endo-
thelial cells “instructs” gut endoderm to express
liver-specifi c genes by inhibiting an inhibitory
factor of these same genes. Other factors par-
ticipating in this “instruction” are bone mor-
phogenetic proteins (BMPs)
secreted by the
septum transversum. BMPs appear to enhance
the competence of prospective liver endoderm
to respond to FGF2. Once this “instruction”
is received, cells in the liver fi eld differentiate
into both hepatocytes and biliary cell lineages,
a process that is at least partially regulated
by hepatocyte nuclear transcription factors
(HNF3 and
4).
2 months of intrauterine life, and only small
hematopoietic islands remain at birth. The
weight of the liver is then only 5% of the total
body weight.
Another important function of the liver
begins at approximately the 12th week, when
bile is formed by hepatic cells. Meanwhile, since
the gallbladder and cystic duct have developed
and the cystic duct has joined the hepatic duct to
form the bile duct (Fig. 15.15), bile can enter
the gastrointestinal tract. As a result, its contents
take on a dark green color. Because of positional
changes of the duodenum, the entrance of the
bile duct gradually shifts from its initial anterior
position to a posterior one, and consequently,
the bile duct passes behind the duodenum
(Figs. 15.19 and 15.20).
MOLECULAR REGULATION OF
LIVER INDUCTION
All of the foregut endoderm has the potential
to express liver-specifi c genes and to differenti-
ate into liver tissue. However, this expression is
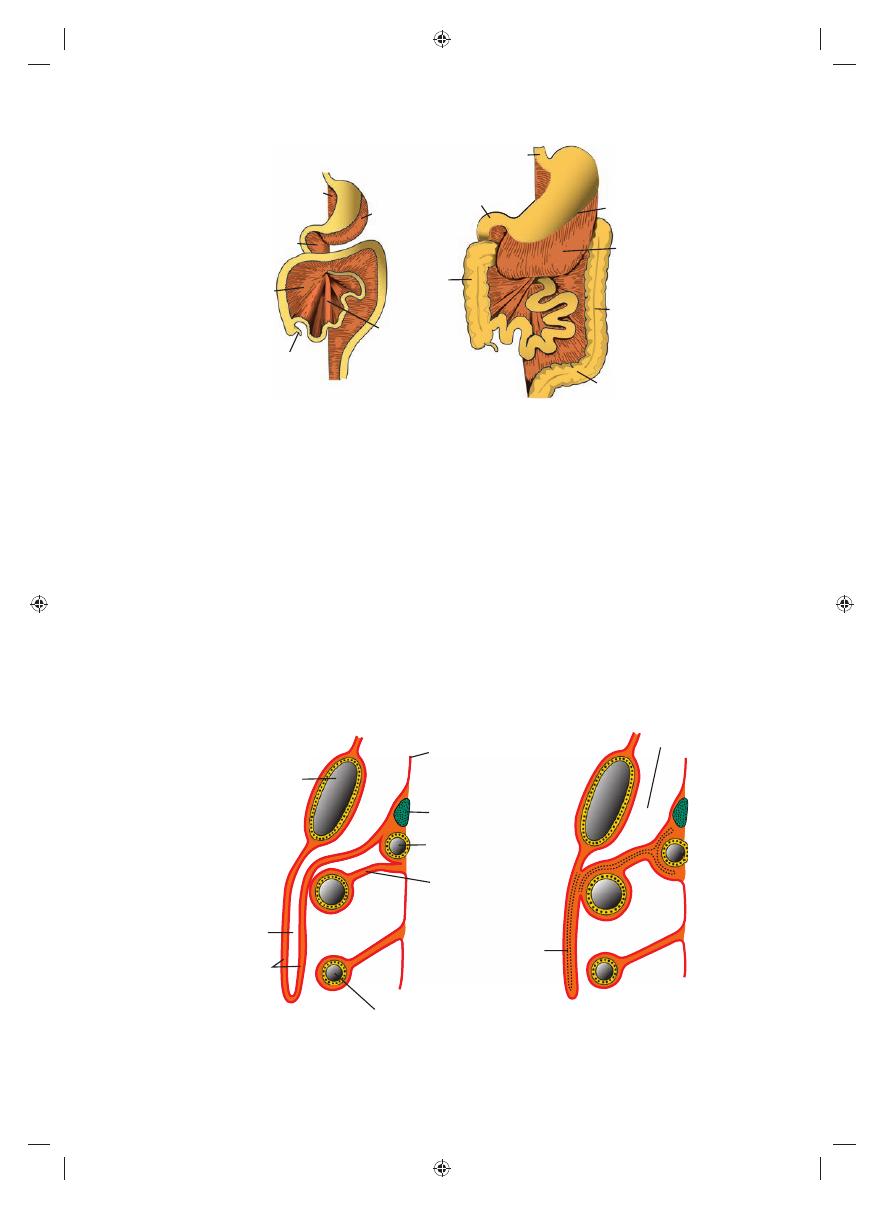
Liver bud
Gallbladder
Ventral
pancreatic bud
A
B
Ventral
pancreas
Dorsal
pancreas
Dorsal
pancreatic bud
Hepatic
duct
Cystic
duct
Bile
duct
Stomach
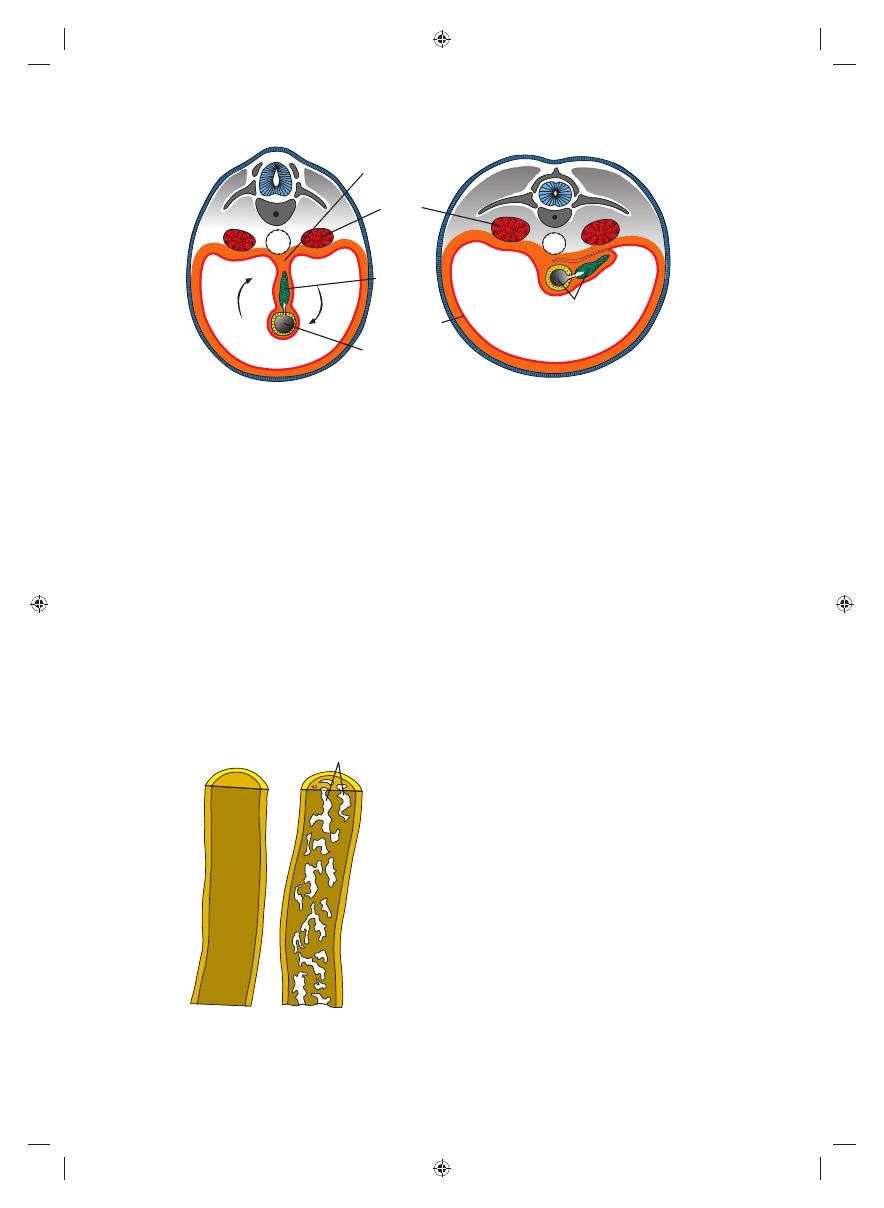
Figure 15.19
Stages in development of the pancreas. A. 30 days (approximately 5 mm). B. 35 days (approximately 7 mm).
Initially, the ventral pancreatic bud lies close to the liver bud, but later, it moves posteriorly around the duodenum toward
the dorsal pancreatic bud.
Bile duct
Bile
duct
Minor papilla
Major papilla
A
B
Ventral
pancreatic duct
Ventral
pancreatic duct
Accessory
pancreatic duct
Main pancreatic duct
Uncinate process
Dorsal
pancreatic duct
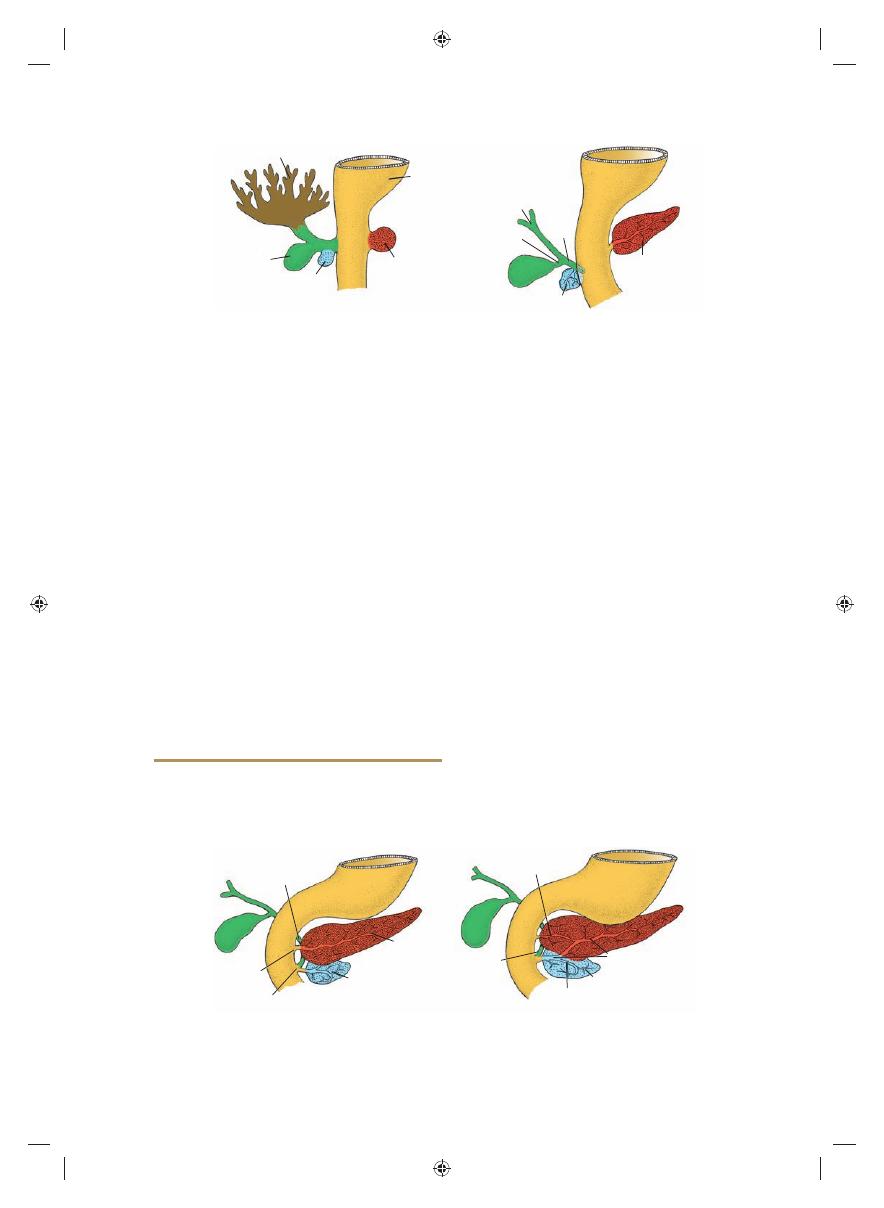
Figure 15.20
A. Pancreas during the sixth week of development. The ventral pancreatic bud is in close contact with the
dorsal pancreatic bud. B. Fusion of the pancreatic ducts. The main pancreatic duct enters the duodenum in combination with
the bile duct at the major papilla. The accessory pancreatic duct (when present) enters the duodenum at the minor papilla.
Sadler_Chap15.indd 219
Sadler_Chap15.indd 219
8/26/2011 7:21:37 AM
8/26/2011 7:21:37 AM
Endoderm
Hepatic
field
Cardiac
mesoderm
FGF
Notochord
Ectoderm
Hindgut
Heart
tube
Foregut
Septum
transversum
BMPs
Distended
hepatic duct
Bile duct,
obliterated
Duodenal loop
Duplication of
gallbladder
Hepatic duct
Cystic duct
Bile duct
A
B
Gallbladder
Sadler_Chap15.indd 220
Sadler_Chap15.indd 220
8/26/2011 7:21:38 AM
8/26/2011 7:21:38 AM

Bile duct
Hepatic duct
Gallbladder
Ventral
pancreas
Main
pancreatic duct
Accessory pancreatic duct
Dorsal
pancreas
Stomach
Sadler_Chap15.indd 221
Sadler_Chap15.indd 221
8/26/2011 7:21:40 AM
8/26/2011 7:21:40 AM
222
Part II Systems-Based Embryology
loop
(Figs. 15.24 and 15.25). At its apex, the loop
remains in open connection with the yolk sac by
way of the narrow vitelline duct (Fig. 15.24).
The cephalic limb of the loop develops into the
distal part of the duodenum, the jejunum, and
part of the ileum. The caudal limb becomes
the lower portion of the ileum, the cecum, the
appendix, the ascending colon, and the proximal
two-thirds of the transverse colon.
Physiological Herniation
Development of the primary intestinal loop is
characterized by rapid elongation, particularly of
the cephalic limb. As a result of the rapid growth
and expansion of the liver, the abdominal cavity
temporarily becomes too small to contain all the
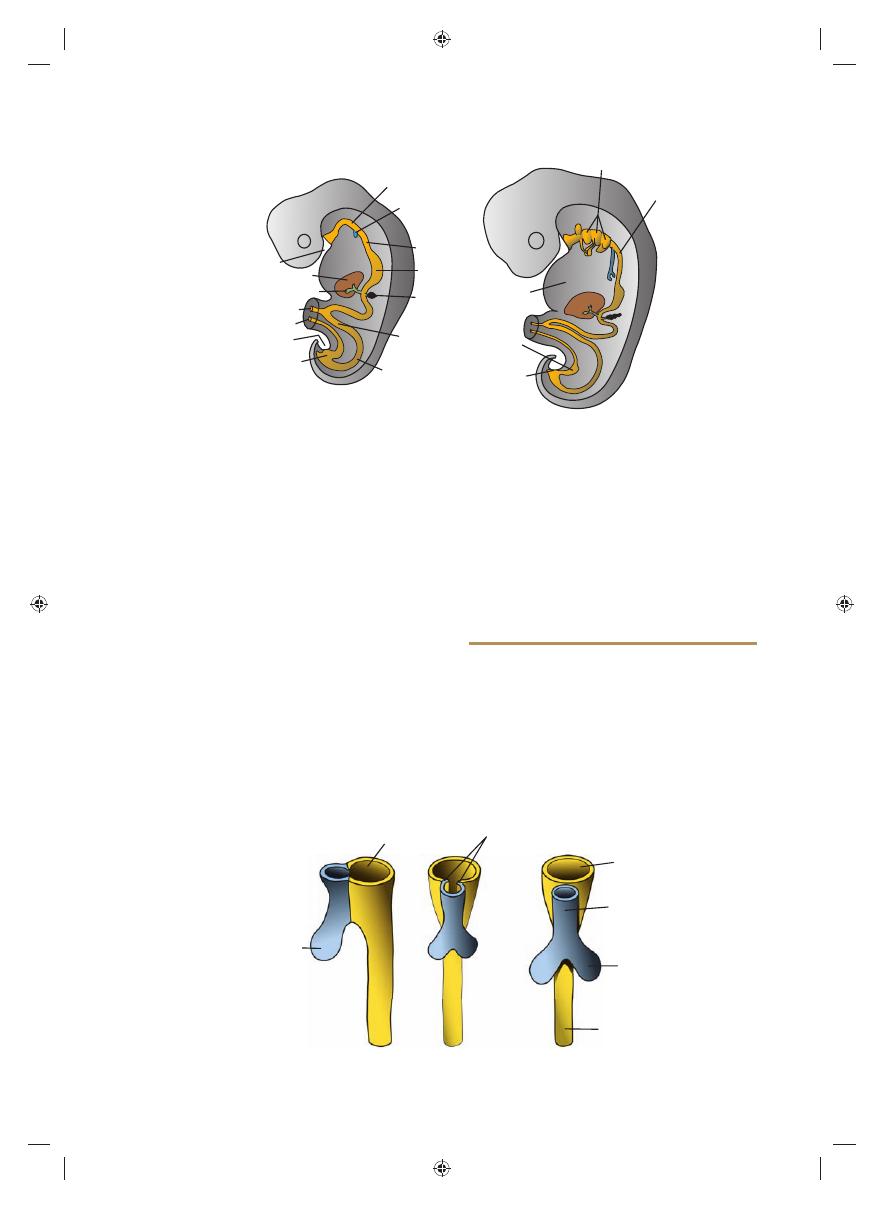
MIDGUT
In the 5-week embryo, the midgut is suspended
from the dorsal abdominal wall by a short mes-
entery and communicates with the yolk sac
by way of the vitelline duct or yolk stalk
(Figs. 15.1 and 15.24). In the adult, the midgut
begins immediately distal to the entrance of the
bile duct into the duodenum (Fig. 15.15) and
terminates at the junction of the proximal two-
thirds of the transverse colon with the distal third.
Over its entire length, the midgut is supplied by
the superior mesenteric artery (Fig. 15.24).
Development of the midgut is characterized
by rapid elongation of the gut and its mesentery,
resulting in formation of the primary intestinal
Celiac artery
Superior mesenteric
artery
Inferior mesenteric
artery
Cloaca
Yolk sac
Liver
Lung bud
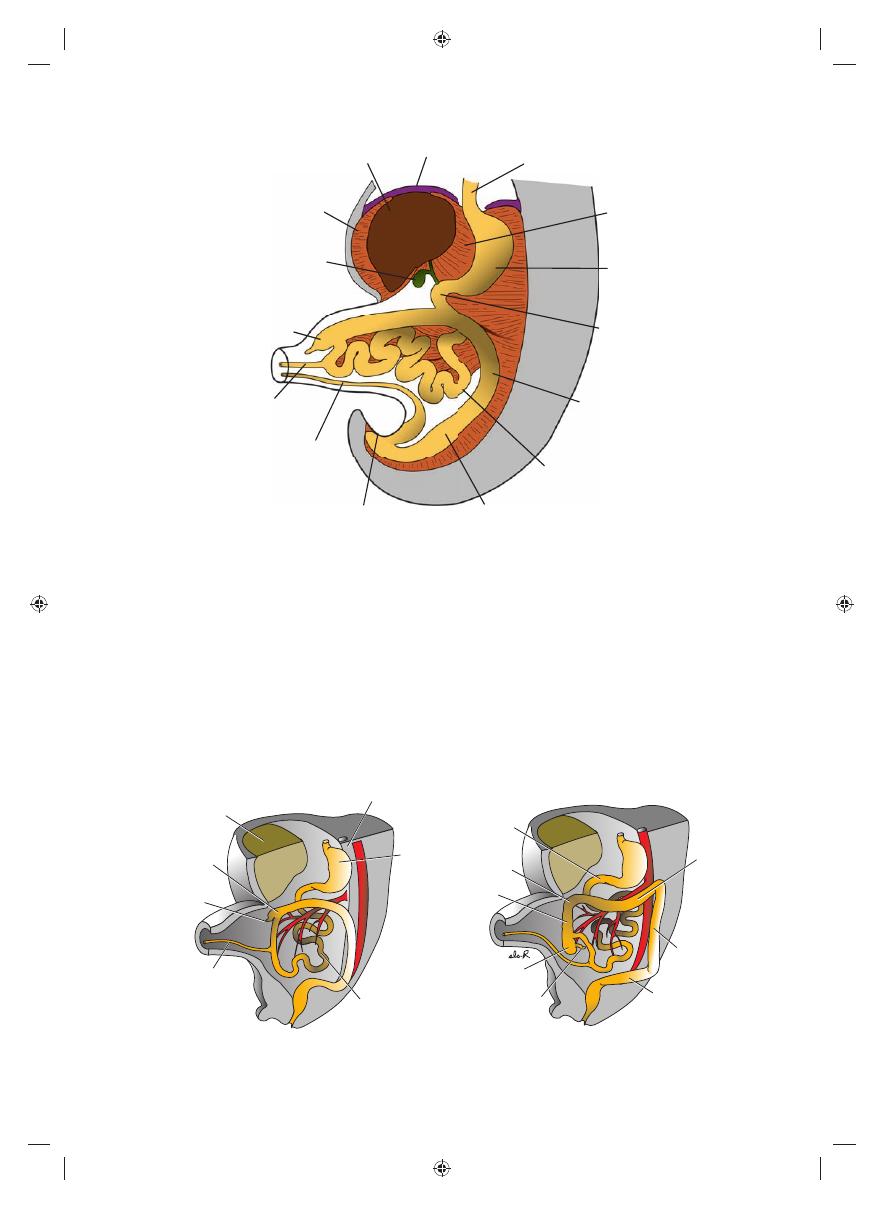
Figure 15.24
Embryo during the sixth week of development, showing blood supply to the segments of the gut and
formation and rotation of the primary intestinal loop. The superior mesenteric artery forms the axis of this rotation and
supplies the midgut. The celiac and inferior mesenteric arteries supply the foregut and hindgut, respectively.
Transverse
colon
Small intestine
Cecal bud
Duodenum
Stomach
Superior
mesenteric
artery
Caudal limb of primary
intestinal loop
Cephalic limb
of primary
intestinal loop
Vitelline
duct
B
A
Figure 15.25
A. Primary intestinal loop before rotation (lateral view). The superior mesenteric artery forms the axis of
the loop. Arrow, counterclockwise rotation. B. Similar view as in A showing the primary intestinal loop after 180° counter-
clockwise rotation. The transverse colon passes in front of the duodenum.
Sadler_Chap15.indd 222
Sadler_Chap15.indd 222
8/26/2011 7:21:42 AM
8/26/2011 7:21:42 AM
Chapter 15 Digestive System
223
counterclockwise, and it amounts to approximately
270° when it is complete (Figs. 15.24 and 15.25).
Even during rotation, elongation of the small intes-
tinal loop continues, and the jejunum and ileum
form a number of coiled loops (Fig. 15.26). The
large intestine likewise lengthens considerably but
does not participate in the coiling phenomenon.
Rotation occurs during herniation (about 90°), as
well as during return of the intestinal loops into
the abdominal cavity (remaining 180°) (Fig. 15.27).
intestinal loops, and they enter the extraembry-
onic cavity in the umbilical cord during the sixth
week of development (physiological umbili-
cal herniation)
(Fig. 15.26).
Rotation of the Midgut
Coincident with growth in length, the primary
intestinal loop rotates around an axis formed by
the superior mesenteric artery (Fig. 15.25).
When viewed from the front, this rotation is
Liver
Diaphragm
Falciform ligament
Vitelline duct
Cecum
Gallbladder
Esophagus
Allantois
Cloacal membrane
Rectum
Lesser omentum
Stomach
Duodenum
Descending color
Jejunoileal loops
Figure 15.26
Umbilical herniation of the intestinal loops in an embryo of approximately 8 weeks (crown-rump length, 35
mm). Coiling of the small intestinal loops and formation of the cecum occur during the herniation. The fi rst 90° of rotation
occurs during herniation; the remaining 180° occurs during the return of the gut to the abdominal cavity in the third month.
Stomach
Jejunoileal
loops
Vitelline
duct
Cecal
bud
Ascending
colon
Aorta
Liver
Duodenum
Transverse
colon
Descending
colon
Ascending
colon
Hepatic
flexure
Sigmoid
Appendix
Cecum
B
A
Figure 15.27
A. Anterior view of the intestinal loops after 270° counterclockwise rotation. Note the coiling of the small
intestinal loops and the position of the cecal bud in the right upper quadrant of the abdomen. B. Similar view as in A with
the intestinal loops in their fi nal position. Displacement of the cecum and appendix caudally places them in the right lower
quadrant of the abdomen.
Sadler_Chap15.indd 223
Sadler_Chap15.indd 223
8/26/2011 7:21:44 AM
8/26/2011 7:21:44 AM
224
Part II Systems-Based Embryology
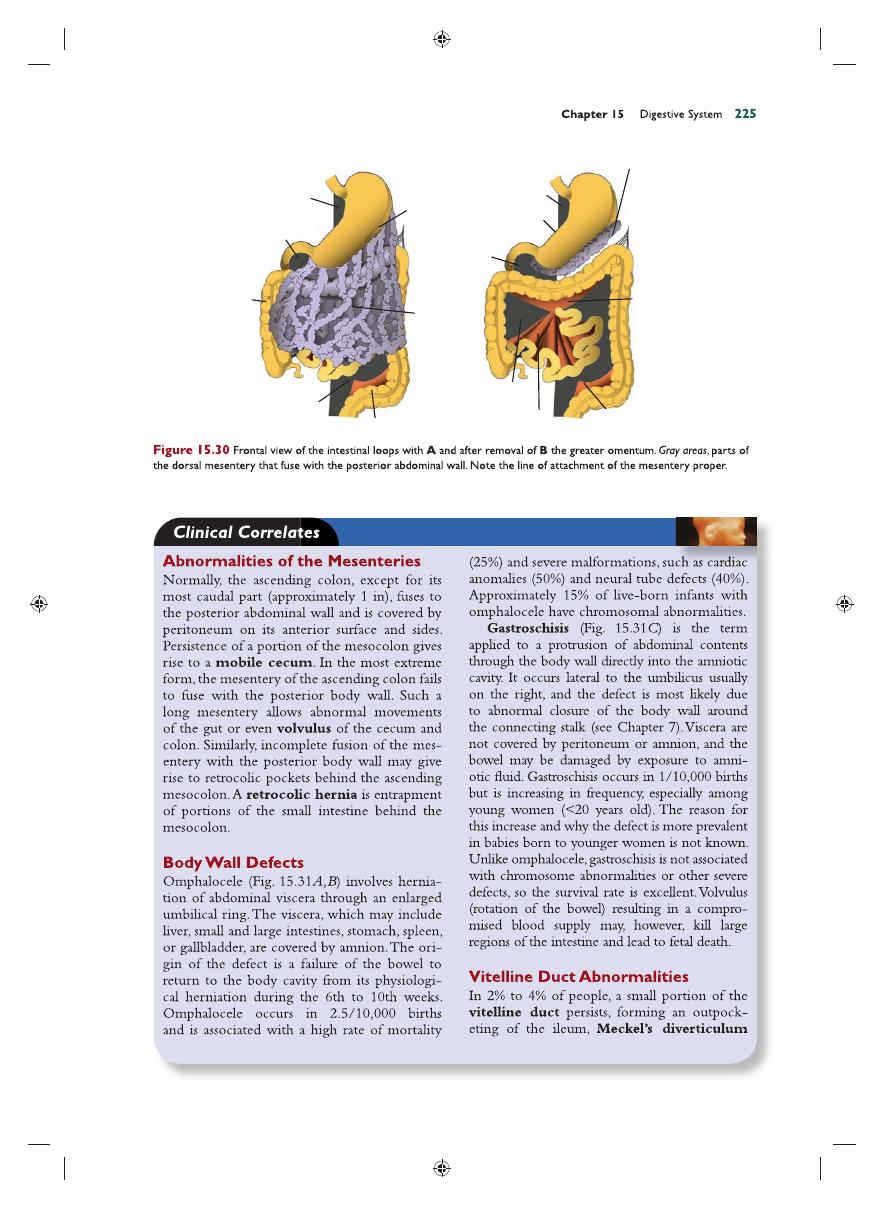
peritoneum of the posterior abdominal wall
(Fig. 15.30). After fusion of these layers, the
ascending and descending colons are perma-
nently anchored in a retroperitoneal position.
The appendix, lower end of the cecum, and
sigmoid colon, however, retain their free mes-
enteries (Fig. 15.30B).
The fate of the transverse mesocolon is dif-
ferent. It fuses with the posterior wall of the
greater omentum (Fig. 15.30) but maintains its
mobility. Its line of attachment fi nally extends
from the hepatic fl exure of the ascending colon
to the splenic fl exure of the descending colon
(Fig. 15.30B).
The mesentery of the jejunoileal loops is
at fi rst continuous with that of the ascending
colon (Fig. 15.30A). When the mesentery of
the ascending mesocolon fuses with the poste-
rior abdominal wall, the mesentery of the jeju-
noileal loops obtains a new line of attachment
that extends from the area where the duodenum
becomes intraperitoneal to the ileocecal junction
(Fig. 15.30B).
Retraction of Herniated Loops
During the 10th week, herniated intestinal
loops begin to return to the abdominal cavity.
Although the factors responsible for this return
are not precisely known, it is thought that regres-
sion of the mesonephric kidney, reduced growth
of the liver, and expansion of the abdominal cav-
ity play important roles.
The proximal portion of the jejunum, the
fi rst part to reenter the abdominal cavity, comes
to lie on the left side (Fig. 15.27A). The later
returning loops gradually settle more and more
to the right. The cecal bud, which appears at
about the sixth week as a small conical dila-
tion of the caudal limb of the primary intes-
tinal loop, is the last part of the gut to reenter
the abdominal cavity. Temporarily, it lies in the
right upper quadrant directly below the right
lobe of the liver (Fig. 15.27A). From here, it
descends into the right iliac fossa, placing the
ascending colon
and hepatic fl exure on the
right side of the abdominal cavity (Fig. 15.27B).
During this process, the distal end of the cecal
bud forms a narrow diverticulum, the appen-
dix
(Fig. 15.28).
Since the appendix develops during descent
of the colon, its fi nal position frequently is pos-
terior to the cecum or colon. These positions of
the appendix are called retrocecal or retrocolic,
respectively (Fig. 15.29).
Mesenteries of the Intestinal Loops
The mesentery of the primary intestinal loop,
the mesentery proper, undergoes profound
changes with rotation and coiling of the bowel.
When the caudal limb of the loop moves to
the right side of the abdominal cavity, the dor-
sal mesentery twists around the origin of the
superior mesenteric artery
(Fig. 15.24).
Later, when the ascending and descending
portions of the colon obtain their defi nitive
positions, their mesenteries press against the
Ascending colon
Ileum
Appendix
Appendix
Cecal bud
A
B
C
Vitelline duct
Cecum
Cecum
Tenia
Jejunoileal loops
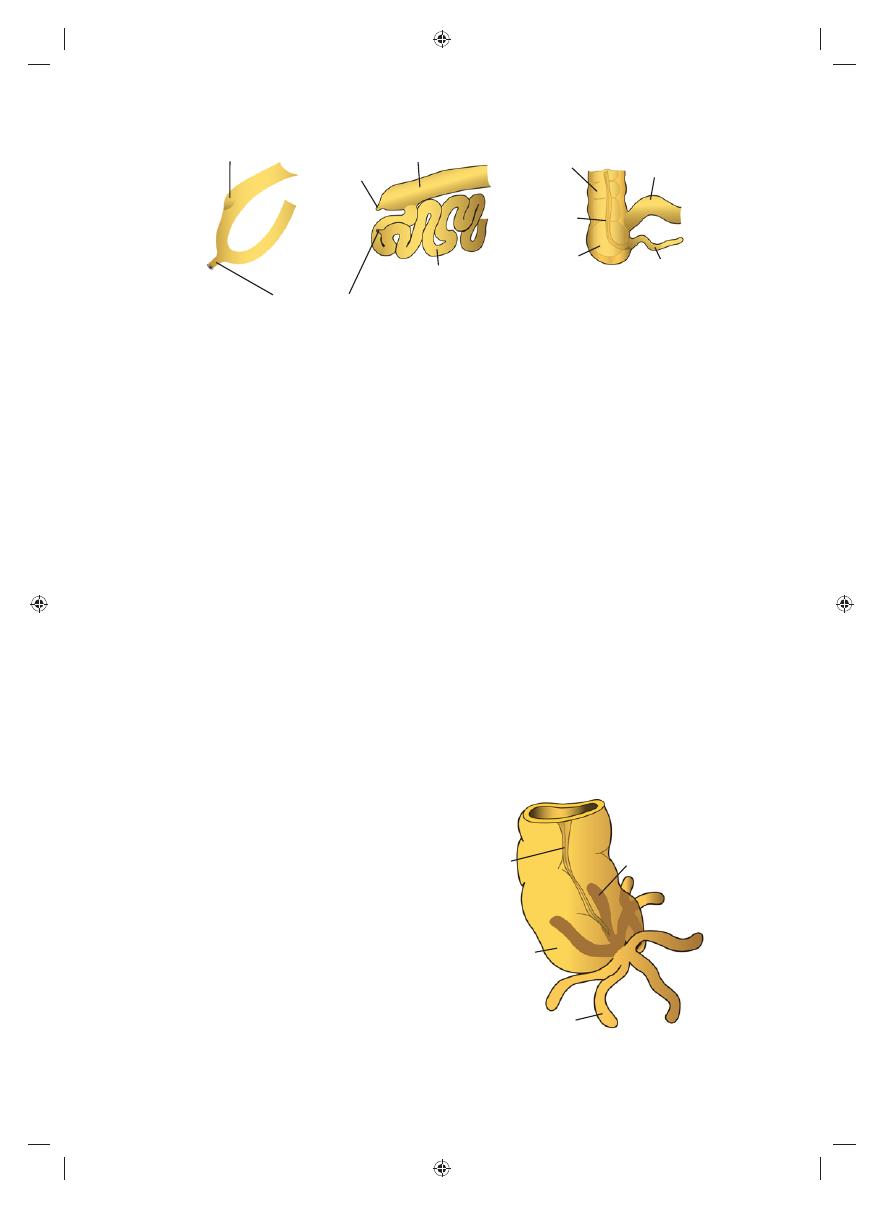
Figure 15.28
Successive stages in development of the cecum and appendix. A. 7 weeks. B. 8 weeks. C. Newborn.
Retrocecal
position of
vermiform
appendix
Tenia
libera
Cecum
Vermiform appendix
Figure 15.29
Various positions of the appendix. In about
50% of cases, the appendix is retrocecal or retrocolic.
Sadler_Chap15.indd 224
Sadler_Chap15.indd 224
8/26/2011 7:21:44 AM
8/26/2011 7:21:44 AM
Dorsal mesoduodenum
fused with
abdominal
wall
Dorsal
mesoduodenum
fused with
posterior
abdominal
wall
Mesocolon fused with
abdominal wall
Mesocolon fused with
abdominal wall
Dorsal mesogastruim
fused with
abdominal
wall
Dorsal mesogastruim
fused with
posterior
abdominal wall
Ascending
colon
Greater
curvature
Lesser curvature
Greater
omentum
Sigmoid
Sigmoid
mesocolon
Transverse
mesocolon
Cut edge of
greater omentum
Mesentery proper
B
A
Sadler_Chap15.indd 225
Sadler_Chap15.indd 225
8/26/2011 7:21:45 AM
8/26/2011 7:21:45 AM
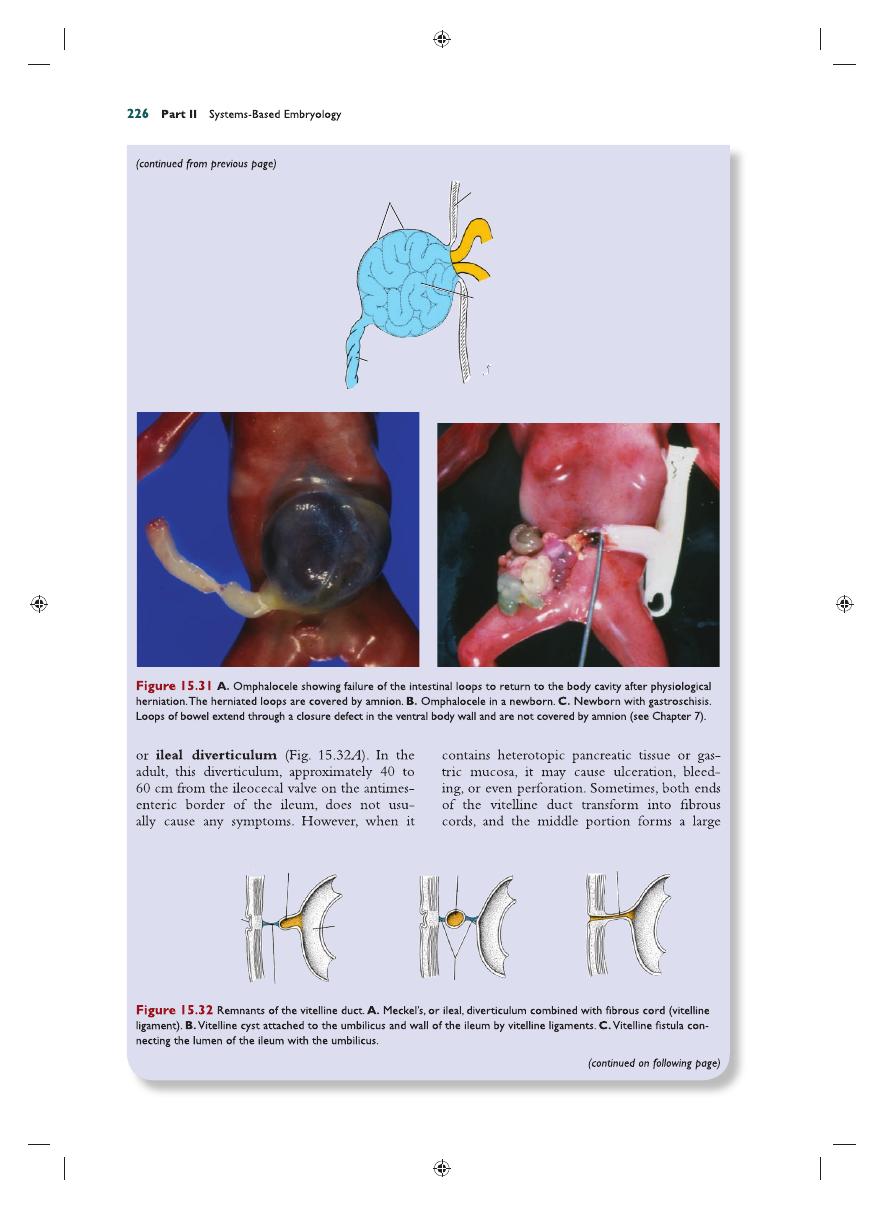
A
B
C
Vitelline ligaments
Vitelline ligaments
Vitelline cyst
Vitelline fistula
Meckel’s diverticulum
Umbilicus
Ileum
Amnion
Abdominal
wall
Intestinal
loops
Umbilical
cord
A
B
C
Sadler_Chap15.indd 226
Sadler_Chap15.indd 226
8/26/2011 7:21:47 AM
8/26/2011 7:21:47 AM
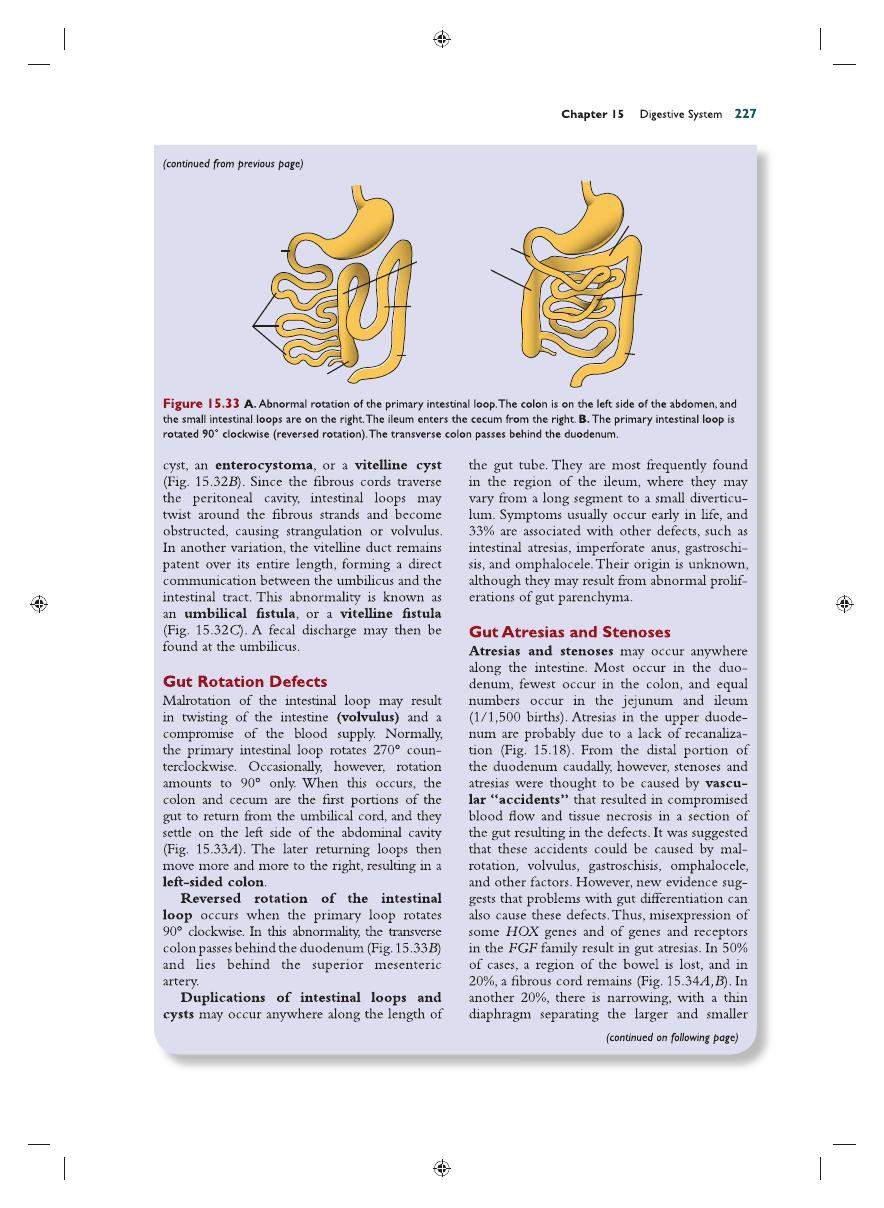
Transverse
colon
Transverse
colon
Ascending colon
Duodenum
Duodenum
Cecum
B
A
Descending
colon
Descending
colon
Jejunoileal
loops
Jejunoileal
loops
Sadler_Chap15.indd 227
Sadler_Chap15.indd 227
8/26/2011 7:21:50 AM
8/26/2011 7:21:50 AM
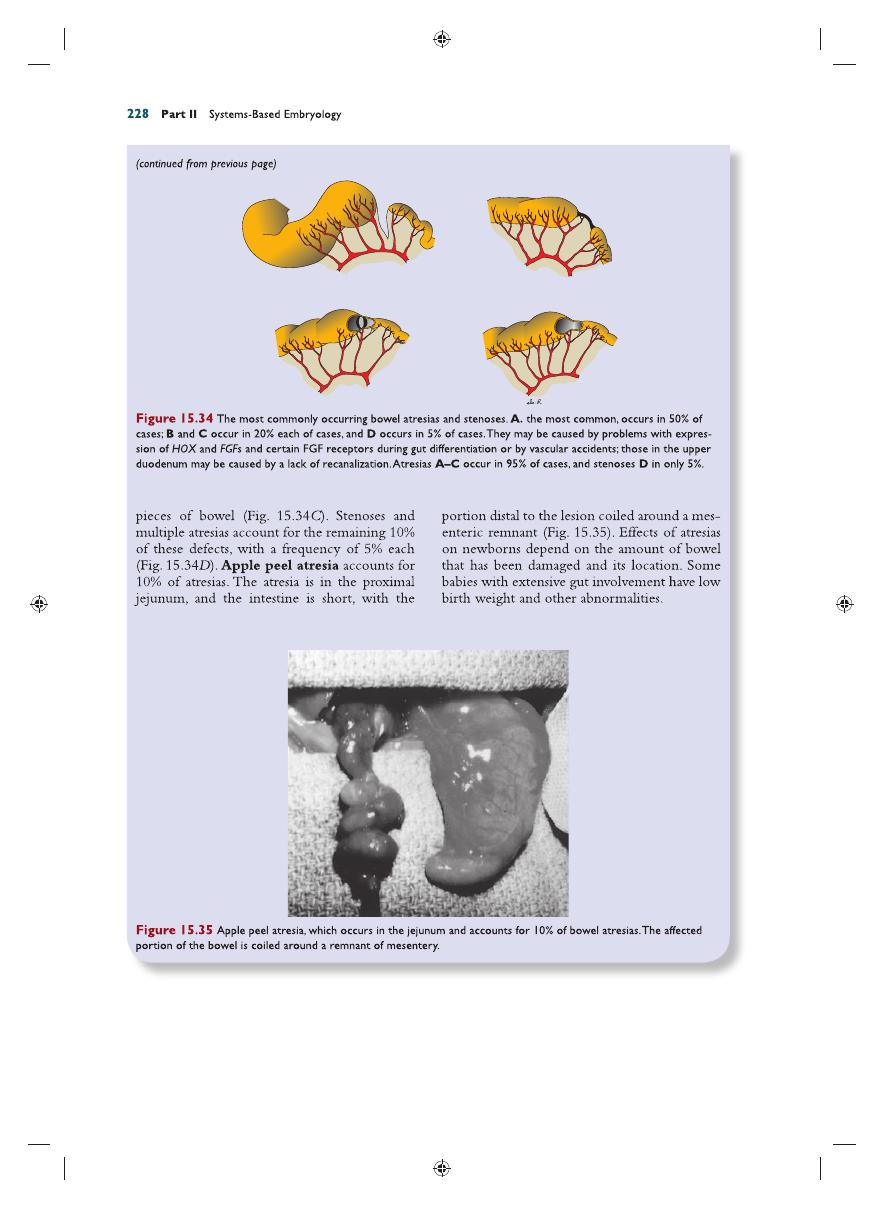
A
D
C
B
Sadler_Chap15.indd 228
Sadler_Chap15.indd 228
8/26/2011 7:21:51 AM
8/26/2011 7:21:51 AM
Chapter 15 Digestive System
229
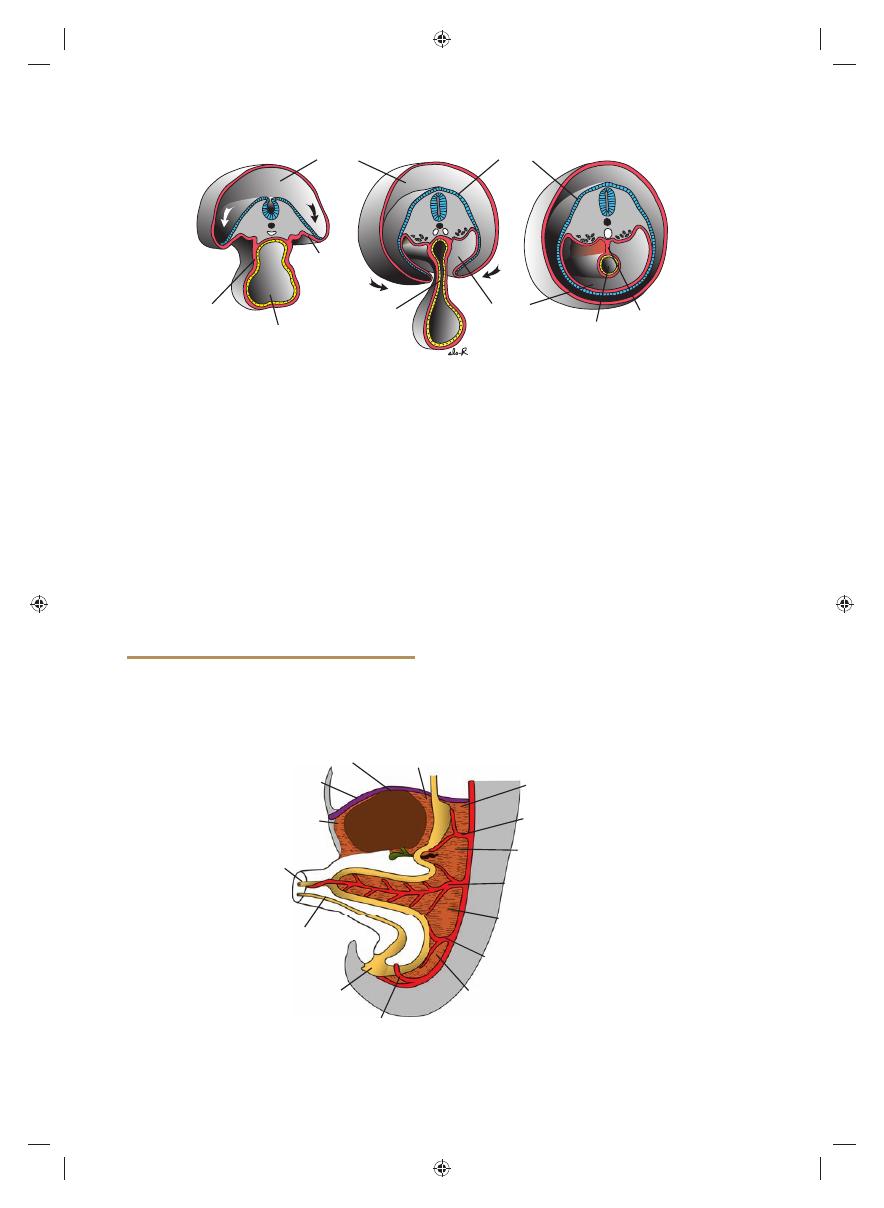
HINDGUT
The hindgut gives rise to the distal third of the
transverse colon, the descending colon, the sig-
moid, the rectum, and the upper part of the anal
canal. The endoderm of the hindgut also forms
the internal lining of the bladder and urethra (see
Chapter 16).
The terminal portion of the hindgut enters
into the posterior region of the cloaca, the
primitive anorectal canal; the allantois enters
into the anterior portion, the primitive uro-
genital sinus
(Fig 15.36A). The cloaca itself is
an endoderm-lined cavity covered at its ventral
boundary by surface ectoderm. This boundary
between the endoderm and the ectoderm forms
the cloacal membrane (Fig. 15.36). A layer of
mesoderm, the urorectal septum, separates the
region between the allantois and hindgut. This
septum is derived from the merging of meso-
derm covering the yolk sac and surrounding the
allantois (Figs. 15.1 and 15.36). As the embryo
grows and caudal folding continues, the tip of
the urorectal septum comes to lie close to the
cloacal membrane (Fig. 15.36B,C). At the end
of the seventh week, the cloacal membrane rup-
tures, creating the anal opening for the hindgut
and a ventral opening for the urogenital sinus.
Between the two, the tip of the urorectal sep-
tum forms the perineal body (Fig. 15.36C).
The upper part (two-thirds) of the anal canal
is derived from endoderm of the hindgut; the
lower part (one-third) is derived from ecto-
derm around the proctodeum (Fig. 15.36B,C).
Ectoderm in the region of the proctodeum on
the surface of part of the cloaca proliferates and
invaginates to create the anal pit (Fig. 15.37D).
Subsequently, degeneration of the cloacal
membrane
(now called the anal membrane)
establishes continuity between the upper and
lower parts of the anal canal. Since the caudal
part of the anal canal originates from ectoderm,
it is supplied by the inferior rectal arteries,
branches of the internal pudendal arteries.
However, the cranial part of the anal canal origi-
nates from endoderm and is therefore supplied
by the superior rectal artery, a continuation
of the inferior mesenteric artery, the artery
of the hindgut. The junction between the endo-
dermal and ectodermal regions of the anal canal
is delineated by the pectinate line, just below
the anal columns. At this line, the epithelium
changes from columnar to stratifi ed squamous
epithelium.
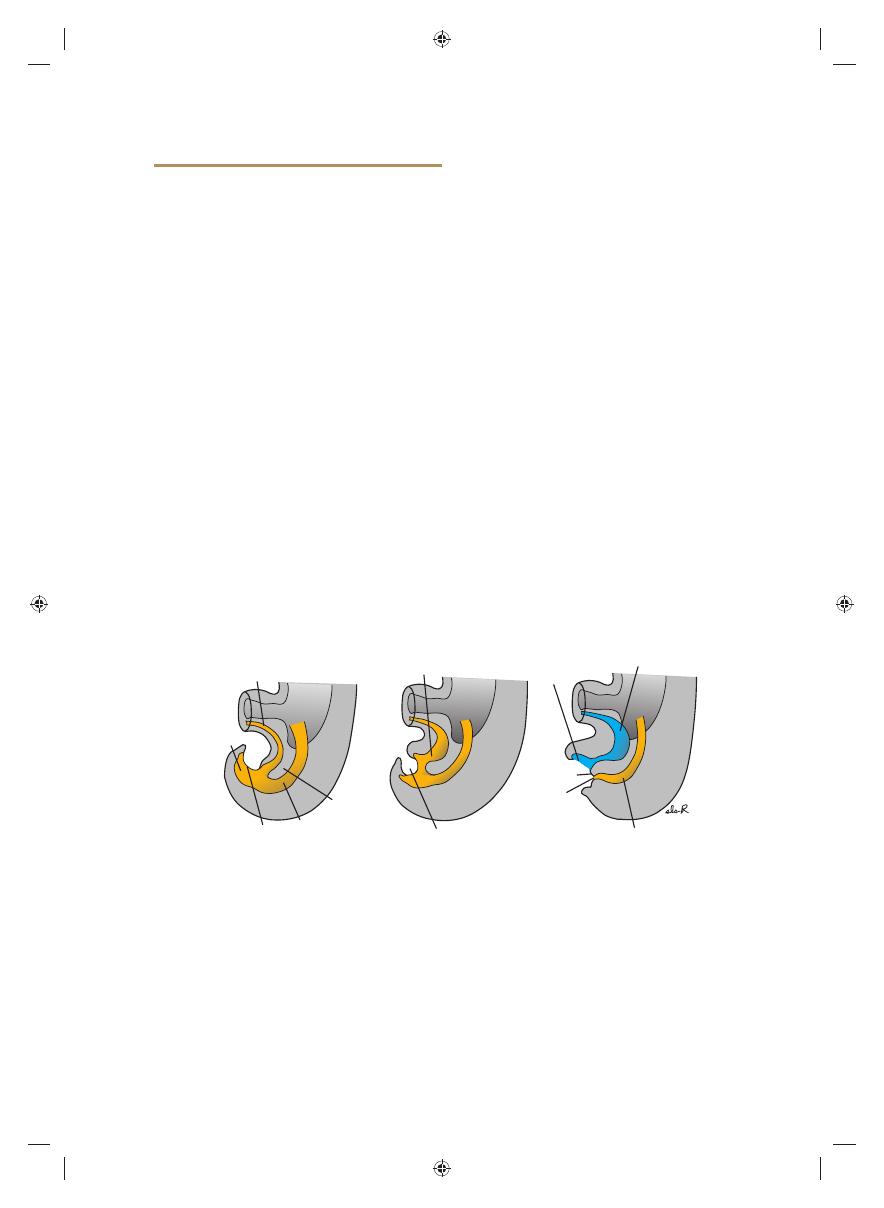
A
B
C
Cloaca
Hindgut
Cloacal
membrane
Urogenital
membrane
Anal
membrane
Anorectal canal
Perineal
body
Primitive urogenital sinus
Allantois
Urinary bladder
Urorectal
septum
Proctodeum
Figure 15.36
Cloacal region in embryos at successive stages of development. A. The hindgut enters the posterior por-
tion of the cloaca, the future anorectal canal; the allantois enters the anterior portion, the future urogenital sinus. The
urorectal septum is formed by merging of the mesoderm covering the allantois and the yolk sac (Fig. 14.1D). The cloacal
membrane, which forms the ventral boundary of the cloaca, is composed of ectoderm and endoderm. B. As caudal fold-
ing of the embryo continues, the urorectal septum moves closer to the cloacal membrane. C. Lengthening of the genital
tubercle pulls the urogenital portion of the cloaca anteriorly; breakdown of the cloacal membrane creates an opening for
the hindgut and one for the urogenital sinus. The tip of the urorectal septum forms the perineal body.
Sadler_Chap15.indd 229
Sadler_Chap15.indd 229
8/26/2011 7:21:52 AM
8/26/2011 7:21:52 AM
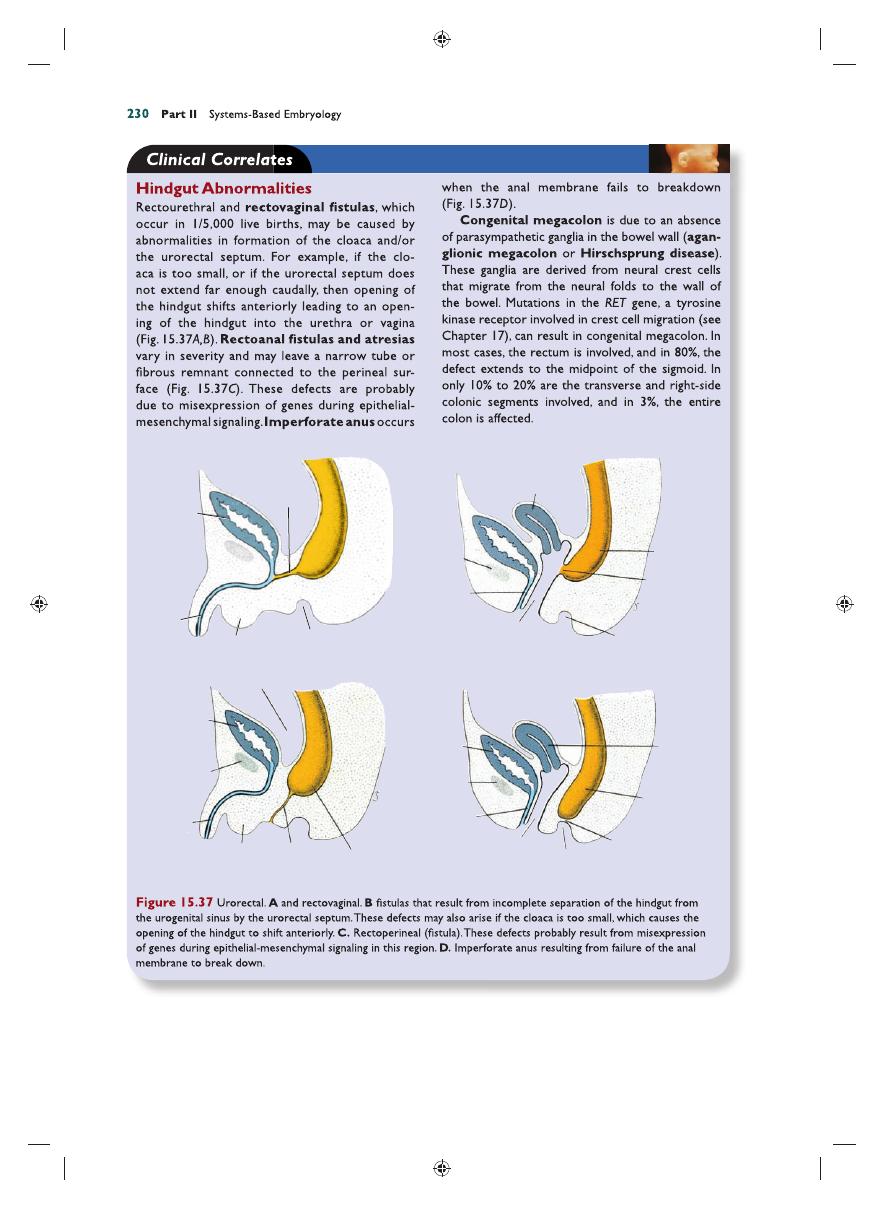
Urinary
bladder
Urethra
Urethra
Urethra
Urethra
Scrotum
Symphysis
Symphysis
Symphysis
Uterus
Uterus
Rectum
Rectum
Rectum
Rectovaginal
fistula
Rectoperineal
fistula
Peritoneal cavity
Anal pit
Anal pit
Anal membrane
Vagina
Vagina
Unrinary
bladder
Unrinary
bladder
Urorectal
fistula
Scrotum
Anal pit
A
B
C
D
Sadler_Chap15.indd 230
Sadler_Chap15.indd 230
8/26/2011 7:21:52 AM
8/26/2011 7:21:52 AM
Chapter 15 Digestive System
231
duct. During the sixth week, the loop grows so
rapidly that it protrudes into the umbilical cord
(physiological herniation) (Fig. 15.26). During
the 10th week, it returns into the abdominal
cavity. While these processes are occurring, the
midgut loop rotates 270° counterclockwise (Fig.
15.27). Remnants of the vitelline duct, failure
of the midgut to return to the abdominal cavity,
malrotation, stenosis, and duplication of parts of
the gut are common abnormalities.
The hindgut gives rise to the region from the
distal third of the transverse colon to the upper part
of the anal canal; the distal part of the anal canal
originates from ectoderm. The hindgut enters the
posterior region of the cloaca (future anorectal
canal), and the allantois enters the anterior region
(future urogenital sinus). The urorectal septum
will divide the two regions (Fig. 15.36) and break-
down of the cloacal membrane covering this area
will provide communication to the exterior for
the anus and urogenital sinus. Abnormalities in the
size of the posterior region of the cloaca shift the
entrance of the anus anteriorly, causing rectovaginal
and rectourethral fi stulas and atresias (Fig. 15.37).
The anal canal itself is derived from endoderm
(cranial part) and ectoderm (caudal part). The
caudal part is formed by invaginating ectoderm
around the proctodeum. Vascular supply to the
anal canal refl ects its dual origin. Thus, the cranial
part is supplied by the superior rectal artery
from the inferior mesenteric artery, the artery of
the hindgut, whereas the caudal part is supplied
by the inferior rectal artery, a branch of the
internal pudendal artery.
Problems to Solve
1.
Prenatal ultrasound showed polyhydram-
nios at 36 weeks, and at birth, the infant had
excessive fl uids in its mouth and diffi culty
breathing. What birth defect might cause
these conditions?
2.
Prenatal ultrasound at 20 weeks revealed a
midline mass that appeared to contain intes-
tines and was membrane bound. What diag-
nosis would you make, and what would be
the prognosis for this infant?
3.
At birth, a baby girl has meconium in her
vagina and no anal opening. What type of
birth defect does she have, and what was its
embryological origin?
Summary
The epithelium of the digestive system and the
parenchyma of its derivatives originate in the
endoderm; connective tissue, muscular com-
ponents, and peritoneal components originate
in the mesoderm. Different regions of the gut
tube such as the esophagus, stomach, duodenum,
etc. are specifi ed by a RA gradient that causes
transcription factors unique to each region to be
expressed (Fig. 15.2A). Then, differentiation of
the gut and its derivatives depends upon recip-
rocal interactions between the gut endoderm
(epithelium) and its surrounding mesoderm (an
epithelial-mesenchymal interaction). HOX genes
in the mesoderm are induced by SHH secreted
by gut endoderm and regulate the craniocaudal
organization of the gut and its derivatives. The gut
system extends from the oropharyngeal mem-
brane to the cloacal membrane (Fig. 15.5) and is
divided into the pharyngeal gut, foregut, midgut,
and hindgut. The pharyngeal gut gives rise to the
pharynx and related glands (see Chapter 17).
The foregut gives rise to the esophagus, the tra-
chea and lung buds, the stomach, and the duodenum
proximal to the entrance of the bile duct. In addi-
tion, the liver, pancreas, and biliary apparatus develop
as outgrowths of the endodermal epithelium of the
upper part of the duodenum (Fig. 15.15). Since the
upper part of the foregut is divided by a septum
(the tracheoesophageal septum) into the esophagus
posteriorly and the trachea and lung buds anteri-
orly, deviation of the septum may result in abnor-
mal openings between the trachea and esophagus.
The epithelial liver cords and biliary system grow-
ing out into the septum transversum (Fig. 15.15)
differentiate into parenchyma. Hematopoietic cells
(present in the liver in greater numbers before birth
than afterward), the Kupffer cells, and connective
tissue cells originate in the mesoderm. The pancreas
develops from a ventral bud and a dorsal bud that
later fuse to form the defi nitive pancreas (Figs. 15.19
and 15.20). Sometimes, the two parts surround the
duodenum (annular pancreas), causing constriction
of the gut (Fig. 15.23).
The midgut forms the primary intestinal
loop (Fig. 15.24), gives rise to the duodenum dis-
tal to the entrance of the bile duct, and continues
to the junction of the proximal two-thirds of the
transverse colon with the distal third. At its apex,
the primary loop remains temporarily in open
connection with the yolk sac through the vitelline
Sadler_Chap15.indd 231
Sadler_Chap15.indd 231
8/26/2011 7:21:55 AM
8/26/2011 7:21:55 AM