
Lec.5
Appendix
Class (3) :The Ciliated Protozoa
: The ciliate protozoa constitute a large number of species characterized by
1. having numerous short ectoplasmic threads or cilia, which are present in the
trophozoite.
2. Near the anterior end of the body there is a conical mouth, the cytostome, and
at the opposite end an anal opening, the cytopyge.
3. There are two types of nuclei, a larger, less dense macronucleus and nearby a
small, dense micronucleus ( or at times more than one ).
4. Multiplication is by transverse binary fission, with division of the cytoplasm
following that of the nuclei.
5. Many species also undergo conjugation, during which exchange of nuclei oc-
curs.
Balantidium coli:
Balantidium coli has a cosmopolitan distribution in hogs and is a common para-
sites of man, it is found mostly in warm climates.
Morphology:
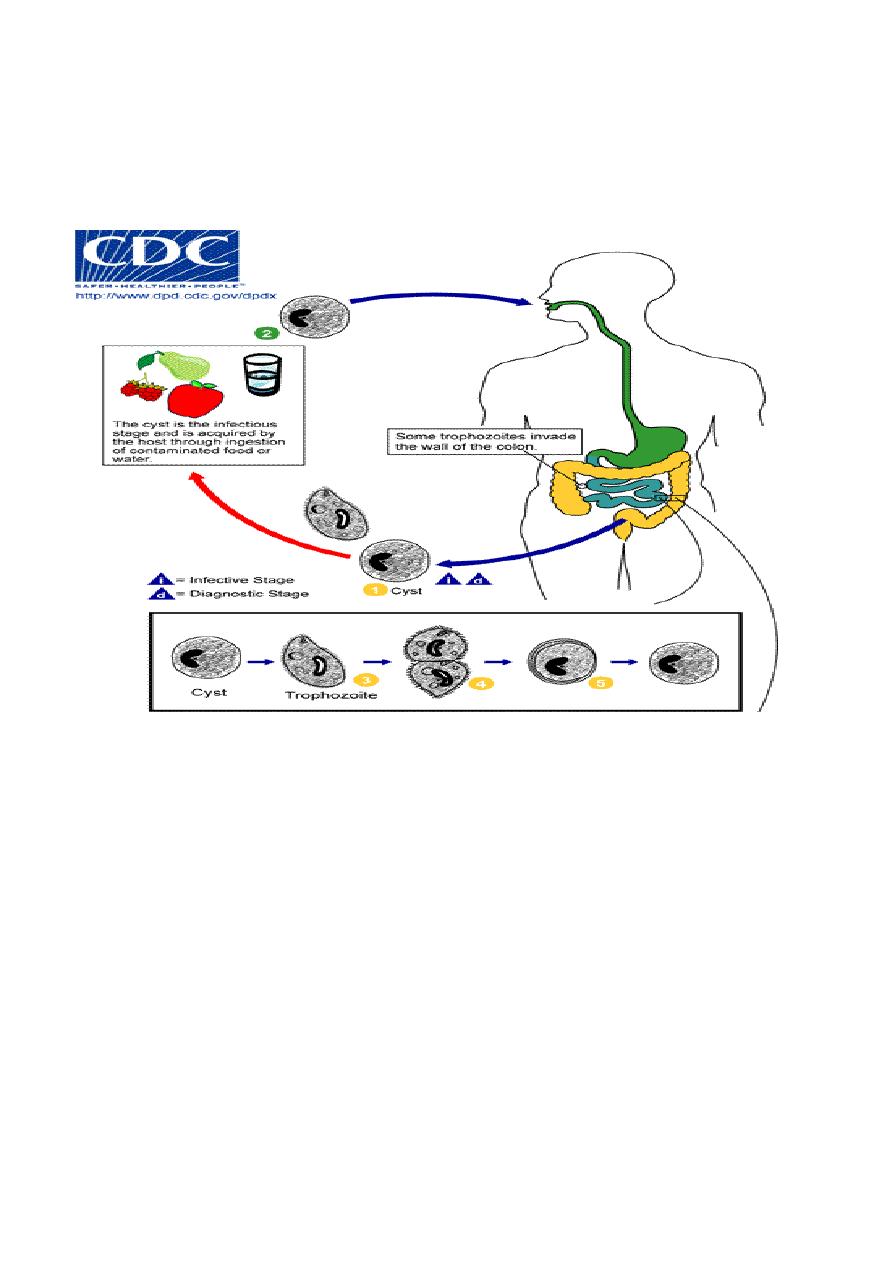
The organism has two stages, trophozoite and cyst.
-
Trophozoite : The trophozoite is the largest of the protozoa parasitizing man.
It is ovoidal, greenish-gray, covered with short cilia which are constantly in
motion during life, and has a vigorous forward movement as it plows through
even relatively thick liquid feces. The anterior end is somewhat conical and
the posterior end broadly rounded. To one side of the anterior tip there is a
funnel-shaped peristome, which leads into the cytostome , A minute cytopy-
ge is situated at the opposite end. One and at time two large pulsating vac-
uoles are found within the cytoplasm. The body is covered with a relatively
tough pellicle. Somewhat posterior to the equator of the organism there is an
elongated kidney-shaped macronucleus and lying within the concave side of
the macronucleus a minute micronucleus.
-
Cyst : The cyst, spherical, is the resting and transfer stage. On encystation the
cilia are soon lost, though the marking on the cell surface remain.

Route of transmission :
Transmission of parasite is by contaminated food and water by the cyst stage of para-
site through faecal – oral transmission . Trophozoite is not infective stage since it is
damage with gastric enzymes if it is enter through the oral route. Further trophozoite
encyst when release with stool and cannot persist for along time within the external
environment.
Life cycle :
Balantidium coli has simple life cycle . after ingestion of cyst stage by the suitable
host excystaion occur in small intestine to release the traophozoites . The natural
habitat of Balantidium coli trophozoite is the cecal level of the large intestine but the
parasite also occurs at all lower levels. It feeds on host cells, bacteria and other nutri-
tious substances in the tissues or lumen of the large bowel.
Asexual reproduction consist of transverse binary fission, in which the micronu-
cleus first divides, then the macronucleus, followed by the cytoplasm, resulting in two
daughter organisms. Although conjugation has been observed in B.coli, this is not a
common occurrence and apparently is not essential for its propagation.
Pathology :
There is little if any evidence that Balantidium coli produces deep invasion of the
intestinal wall, although there may be superficial erosion of the mucosa. the mucosal
layer may be penetrated, with extensive submucosal destruction.
Since Balantidium coli is a much larger, sturdier organism than Entamoeba his-
tolytica, it produces a bigger opening in the intestinal mucosa as it enters the wall.
Moreover, its penetration seems to be accomplished more by boring action than by
lysis. Once established in the tissue it usually has no difficulty in penetration through
the muscularis mucosae into the submucosa, where it spreads out rapidly, causing
rapid destruction of the tissues; but unlike E. histolytica it rarely invades the muscular
coats and it has seldom been found in extra-intestinal tissues. While balantidial le-

sions may develop at any level of the large intestine, they most commonly occur in
the cecal and sigmoid-rectal regions.
The symptoms in balantidiasis vary from fulminating, sometimes fatal dysentery
or profuse diarrhea to an essentially asymptomatic carrier state. In this respect the
parallel the broad spectrum of symptoms in amebic colitis.
Diagnosis and Treatment.:
Diagnosis is made on recovery of the characteristic trophozoites and cysts of Bal-
antidium coli in the stool. Care must be taken that the stool and the water or physio-
logic saline solution employed in making fecal films or microscopic diagnosis of this
infection are not contaminated with free-living infusorians, otherwise these ciliates
may be mistaken for B. coli. Albendazole is the drug of choice.
Prevention :
1. Proper disposal of sewage .
2. Human stool should not be used as fertilizer.
3. Good personal hygiene .
4. Washing of raw vegetable and fruits before consumption and protection of food
from flies and cockroaches .
5. cyst is resistant to routine chlorination therefore drinking water should be puri-
fied by either boiling , filtration or iodination.
Good luck .....Prof. Dr. Amal kh. Khalaf 2020/2021