
Parasitology
Notes…
1
Malaria Lec.1
INTRODUCTION
Malaria is a life-threatening protozoan disease caused by Plasmodium species.
It characterized by fever ,anemia and splenomegaly. It’s typically transmitted
through the bite of an infective female
Anopheles
mosquito.
CLASSIFICATION
CAUSATIVE AGENTS OF HUMAN MALARIA
1)
Plasmodium vivax:
Benign tertian malaria (periodicity of fever is once in 48 hours,
i.e. recurs every third day).
2)
Plasmodium falciparum:
Malignant tertian or subtertian malaria (severe malaria,
periodicity of fever is once in 36-48 hours, recurs every third day).
3)
Plasmodium ovale:
Benign tertian malaria (periodicity of fever is once in 48 hours,
i.e. recurs every third day).
4)
Plasmodium malariae:
Benign quartan malaria (periodicity of fever is once in 72
hours, i.e. recurs every fourth day).
5)
P. knowlesi:
causes quotidian malaria (fever periodicity is once in 24 hours, i.e.
recurs every day). It is a parasite of monkey but can also affect humans.
History and Distribution
The name malaria
(mal: bad, aria: air)
was derived from the ancient false belief:
thought to be caused by foul emissions from marshy soil.
French army surgeon Alphonse Laveran (1880) was the first to discover the
causative agent
Plasmodium
, in the red blood cell (RBC) of a patient in Algeria.
➢
P. vivax
is the most widely distributed, being most common in Asia, North Africa,
and Central and South America.
➢
P. falciparum
the predominant species in Africa, New Guinea and Haiti, is rapidly
spreading in Southeast Asia and India.
➢
P. ovale
is virtually confined to West Africa where it ranks second after
P.falciparum.
➢
P. malariae
is present in most places but is rare, except in Africa
Need So
me
Help?
Parasitology
Notes…
2
classification of endemicity
The World Health Organization (WHO) has recommended the classification of endemicity
depending on the spleen or parasite rate in a statistically significant sample in the
populations of children (2-9 years) and adults in to:
❖
Hypoendemic (transmission is low):
Spleen or parasite rate less than 10%.
❖
Mesoendemic (transmission is moderate):
Spleen or parasite rate 11-50%.
❖
Hyperendemic (transmission is intense but seasonal(rainy season)):
Spleen or
parasite rate 51-75%.
❖
Holoendemic (transmission is intense and constantly present):
Spleen or parasite
rate more than 75%.
Vector
Human malaria is transmitted by over 60 species of
female
Anopheles mosquito.
Male Anopheles doesn’t feed on man and feeds
exclusively on fruit juices, so that the male
Anopheles doesn’t transmit the disease. Whereas
female Anopheles needs at least two blood meals
before laying eggs.
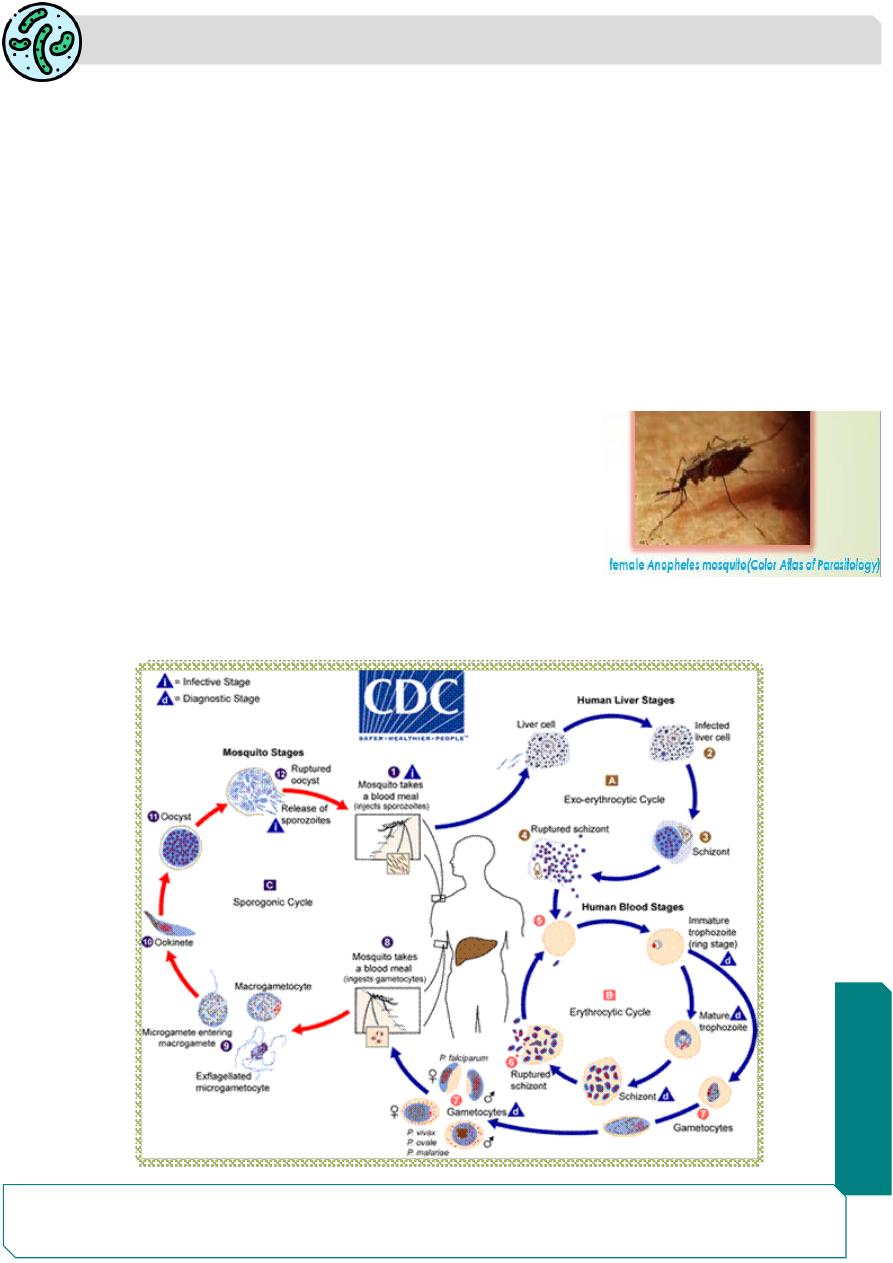
Life Cycle

Parasitology
Notes…
3
Definitive host: Female Anopheles (Anopheline) mosquito is the definitive host
where the sexual cycle (sporogony) takes place.
Intermediate host: Man acts as intermediate host where the asexual cycle
(schizogony) takes place. In humans, schizogony occurs in two locations, in the
liver cells (
exoerythrocytic schizogony, preerythrocytic schizogony)
and in the red
blood cell (
erythrocytic schizogony).
Human Cycle (Schizogony)
Human infection comes through the bite of infective female
Anopheles
mosquito
The sporozoites (infective forms) are injected from the salivary gland of the
mosquito when feeds on blood.
The sporozoites pass into the bloodstream, where some reach the liver and enter
the hepatocytes.
Pre-erythrocytic (tissue, intrahepatic) stage or exo-erythrocytic stage:
The circumsporozoite protein present on the surface of sporozoites binds to the
receptors on the surface of hepatocytes facilitating the entry of sporozoites.
The sporozoites, which are elongated spindle-shaped bodies, become rounded
inside the liver cells. They enlarge in size and undergo repeated division to form
pre-erythrocytic
or
exoerythrocylic schizont which
contain
uninucleate
merozoites.
• Liver schizonts normally rupture in 6-15 days and release thousands of
merozoites into the bloodstream.
• Duration of pre-erythrocytic schizogony varies from 5 days to 15 days depending
on the species.
Erythrocytic stage:
The merozoites invade the RBCs. the receptor for the merozoite is glycophorin
,
the differences in the
glycophorins of red cells of different species may account
for the species specificity of malaria parasites.
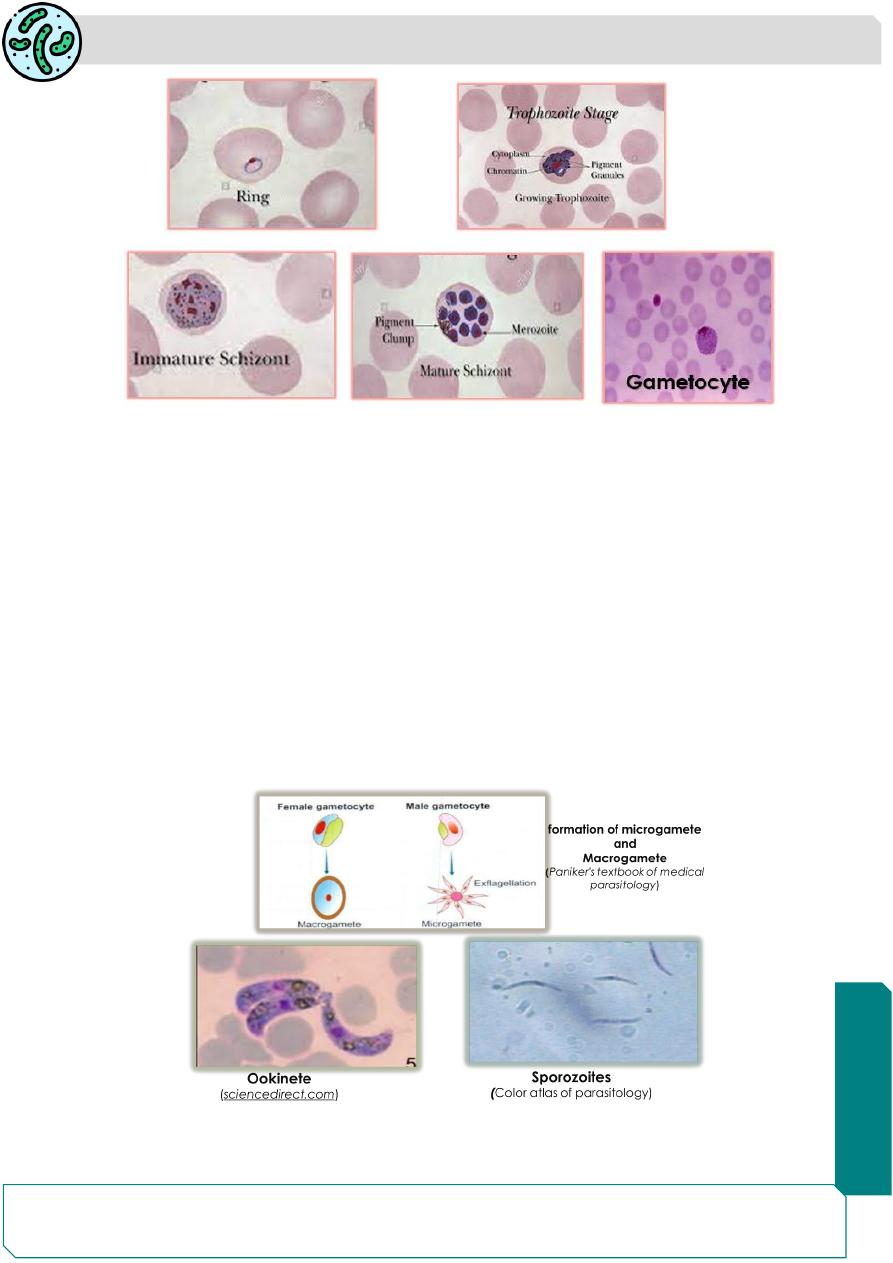
In the erythrocyte, the merozoite appears as a rounded body having a vacuole
incenter with the cytoplasm pushed to the periphery and the nucleus at one pole
(signet ring appearance), these the young parasites are called the
ring forms
.
As the ring form develops, it enlarges in
size becoming irregular in shape and
called the ameboid form.
Parasitology
Notes…
4
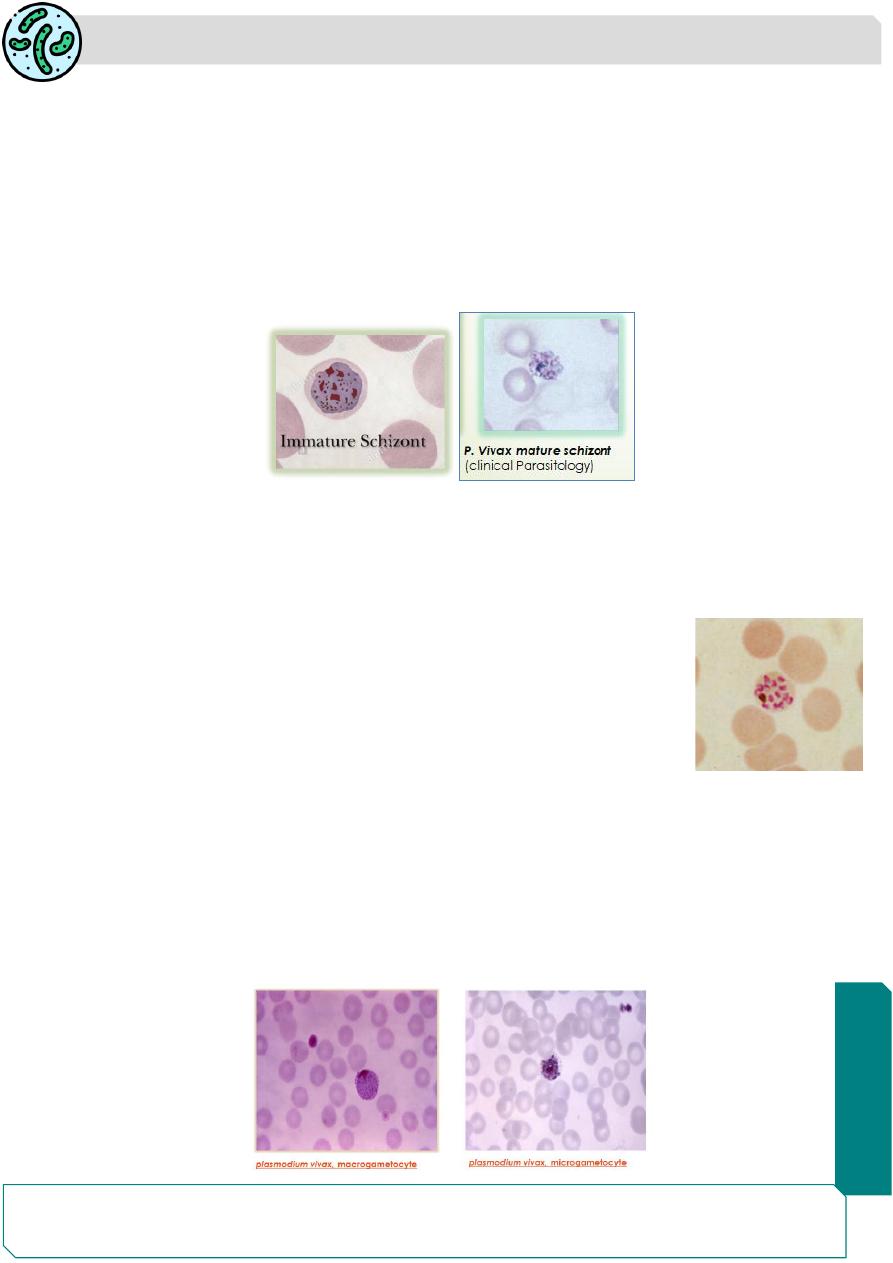
When the ameboid form reaches a certain stage of development, its nucleus starts
dividing by mitosis (immature schizont) followed by a division of cytoplasm to
become mature
schizonts.
The mature schizont bursts releasing the merozoites
into the circulation. The merozoites invade fresh erythrocytes within which they
go through the same process of development.
The rupture of the mature schizont releases large quantities of pyrogens (malarial
pigments, cytokines and toxins). This is responsible for the febrile paroxysms
characterizing malaria.
Malarial pigment
Plasmodium
parasite feeds on hemoglobin of the erythrocyte. it does not
metabolize hemoglobin completely and therefore, leaves behind a hematin-globin
pigment called the malaria pigment or hemozoin pigment, as residue.
The appearance of malarial pigment varies, mostly it is brown
black in color and numerous (except in
P. vivax
it is yellowish
brown in color and in
P. falciparum,
it is few in number)
Gametogony
Some of the merozoites that infect RBCs develop into sexually
differentiated forms, the
gametocytes.
In all species, the female gametocyte is larger, numerous, their cytoplasm stains
deep blue, nucleus is small, red and compact
(macrogametocyte)
while the male
gametocyte are smaller in size, lesser in number, their cytoplasm stains pale blue,
and nucleus is larger, stains red and diffuse
(microgametocyte).
A person with gametocytes in blood is a carrier or reservoir and play an important
role in the transmission of the disease.
Parasitology
Notes…
5
The Mosquito Cycle (Sporogony)
❖ In the mosquito, gametocytes develops in to gametes:
❖ Macro gametocyte one macrogamete.
❖ Microgametocyte 6-8 microgamete,by process called exflagellation.
Exflagellation The nuclear material and cytoplasm of the male gametocytes divides
to produce eight microgametes with long, actively motile, whip-like filaments
❖ One microgametes fertilize macrogamete zygote mobile ookinete.
❖ Ookinete penetrates the gut mucosa of mosquito to the hemocoel side (outer
side ) of the gut oocyte which contains the sporoblast that divided rapidly
to form thousands of sporozoites break out of oocyte hemocoel
salivary gland next patient.
incubation period:
The interval between the entry of sporozoites into the host and
the earliest manifestation of clinical illness.
Parasitology
Notes…
6
Prepatent period:
The interval between the entry of the sporozoites into the body
and the first appearance of the parasites in blood (Ring forms are the first asexual
form that can be demonstrated in the peripheral blood).
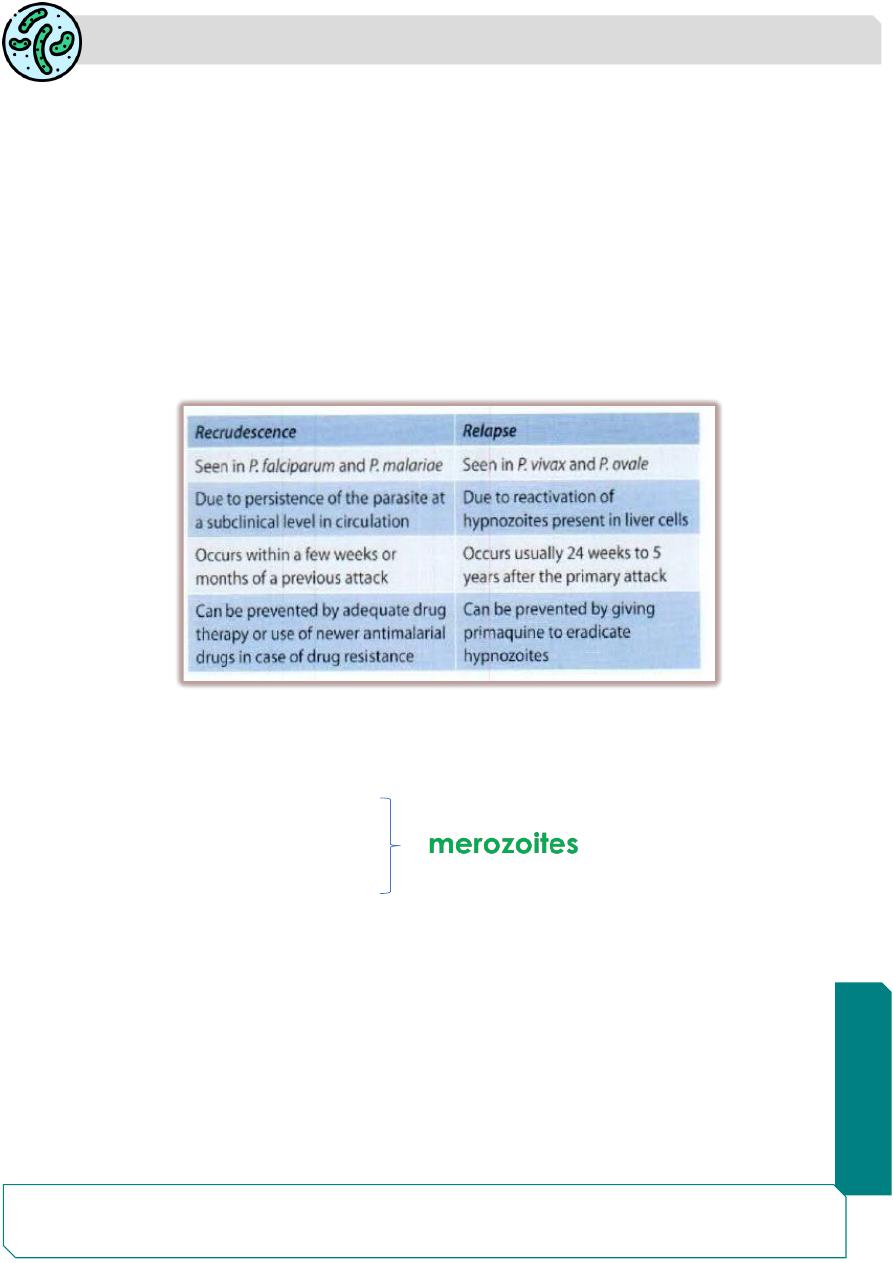
Recrudescence:
In
P. falciparum and P. malariae
, due to persistence of drug
resistant parasites, even after completion of treatment, small numbers of
erythrocytic parasites persist in the bloodstream and in a course of time; they
multiply to reach significant numbers resulting in clinical disease
.
no hypnozoites
are found.
Relapse:
Some sporozoites of
P. vivax and P. ovale
remain dormant (resting
phase) in liver called hypnozoites which cause relapse of malaria after many years
Modes of transmission:
Man gets infection by the bite of infective female
Anopheles
mosquito.
Rarely, it can also be transmitted by:
❖ Blood transfusion.
❖ Transplacental transmission.
❖ contaminated syringes.
Summary
Malaria disease caused by Plasmodium parasite.
P.vivax, P.ovale, P.falciparum and P malariae are the main plasmodium spp.
causing malaria.
Man is the intermediate host.
Female Anopheles (Anopheline) mosquito is the final host.