College of Medicine University of Mosul /Department of: Microbiology
Subject: Parasitology Stage: 3
rd
2021-2022
Dr. Ahmed Al harbi Date: 15/11/2021 No. 1
Pa
ge
1
Lecture Title: Giardia lamblia
Synonyms:
Giardia lamblia (G. lamblia), Giardia doudenalis, Giardia intestinalis
Objectives:
The main objectives of the lecture are:
1. Biology of Giardia parasite
2. Epidemiology and transmission of infection by G. lamblia
3. Pathogenesis and clinical picture of giardiasis
4. Laboratory diagnose and treatment of infection by G. lamblia
5. Control of infection by G.lamblia.
Biology
Habitat
G. lamblia is an intestinal flagellate protozoan lives in the duodenum and upper
jejunum; and is the only protozoan parasite found in the lumen of the human small
intestine.
Infective stage (form):
Is the mature cyst
The infective dose is >=10 mature cysts
Historical background:
Giardia was originally observed by van Leeuwenhoek in 1681, in his own
diarrheal stool.
Described by Vilem Dusan Lambl in 1859 and by Alfred Giard in 1895.
Morphology:
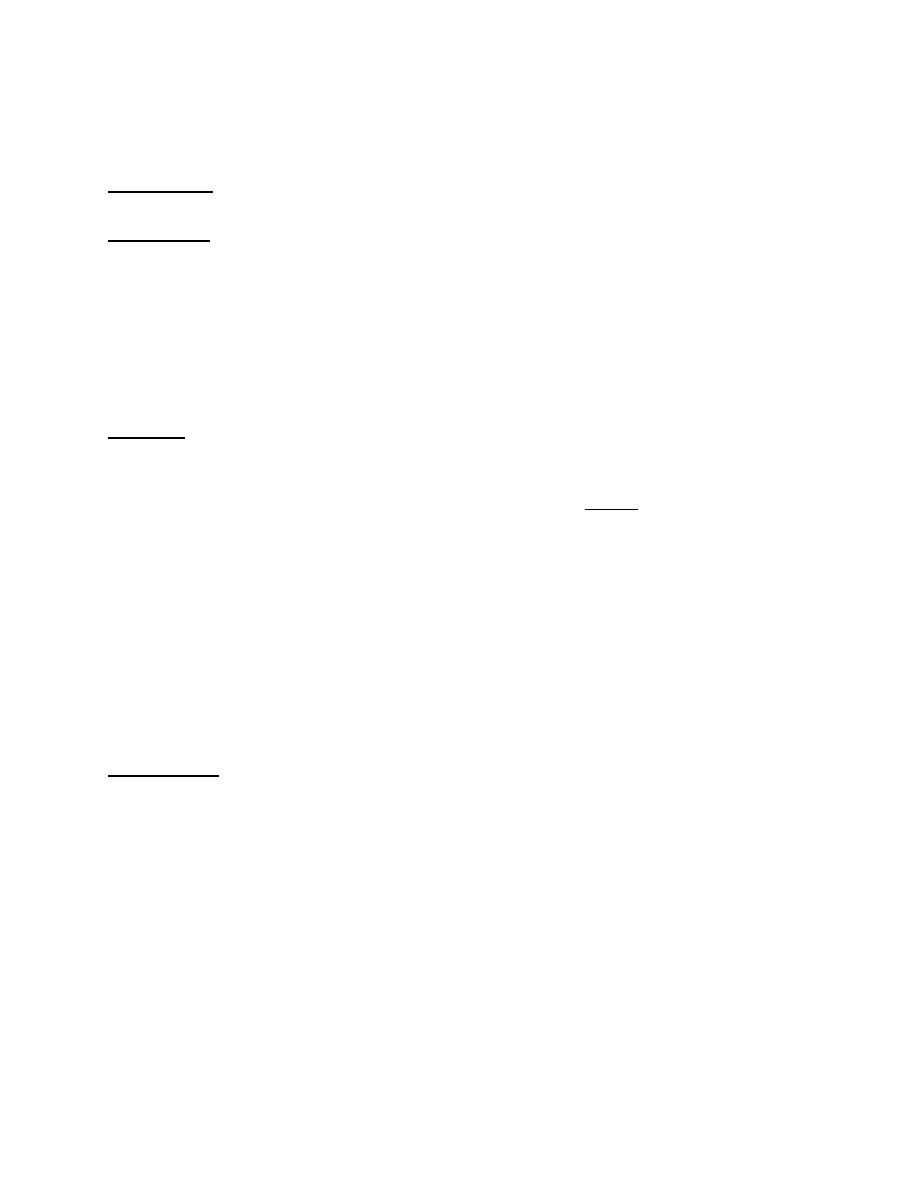
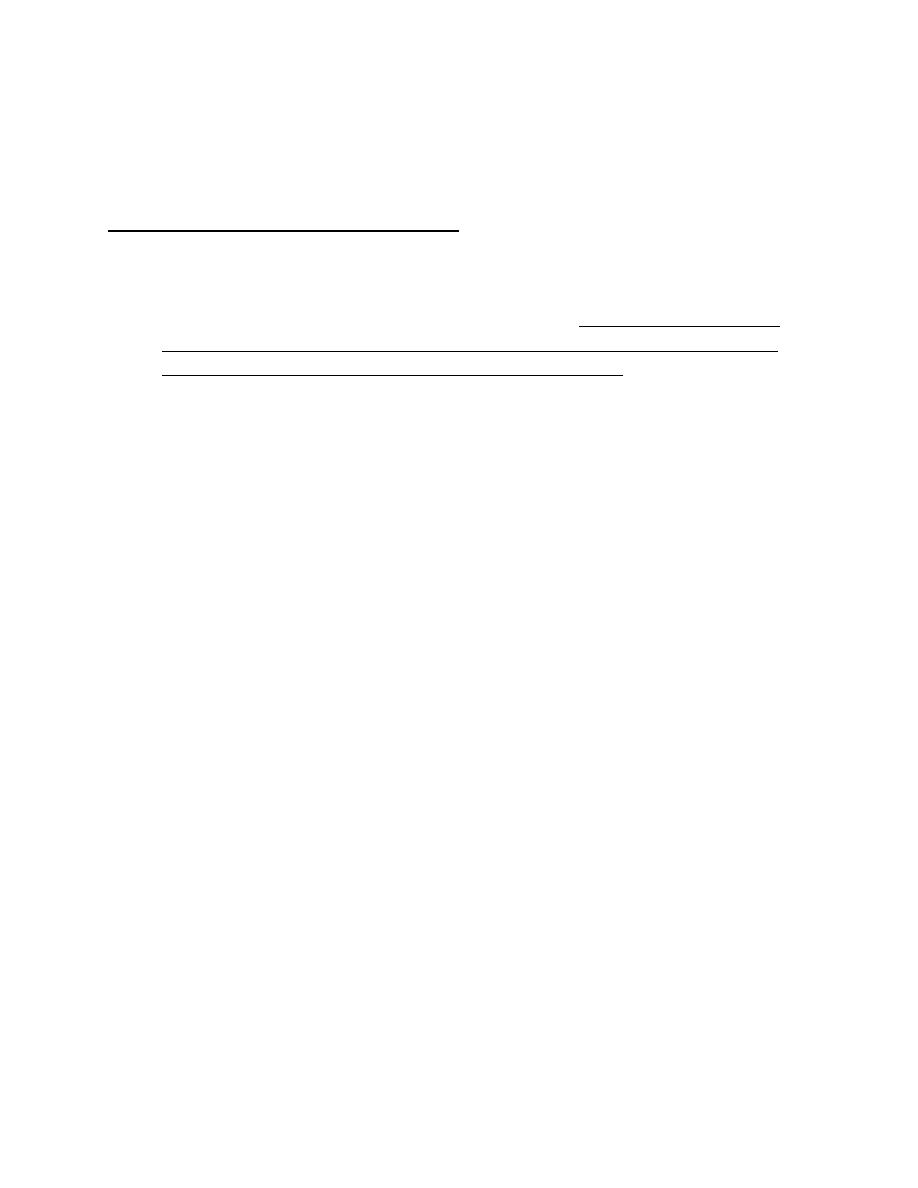
A. Cyst:
The cyst stage has smooth-wall, oval, measures 8-12 μm by 7-10 μm.
When the cyst matures, nuclear division happens.
Cyst is surrounded by hyaline cyst wall.
Mature cyst contains 4 nuclei and then the cyst releases 2 trophozoites upon
excystation.
Once the host is infected, trophozoites may appear in the duodenum within
minutes.
Excystation occurs within 5 minutes of exposure of the cysts to an
environment with a pH between 1.3 and 2.7.
College of Medicine University of Mosul /Department of: Microbiology
Subject: Parasitology Stage: 3
rd
2021-2022
Dr. Ahmed Al harbi Date: 15/11/2021 No. 1
Pa
ge
2
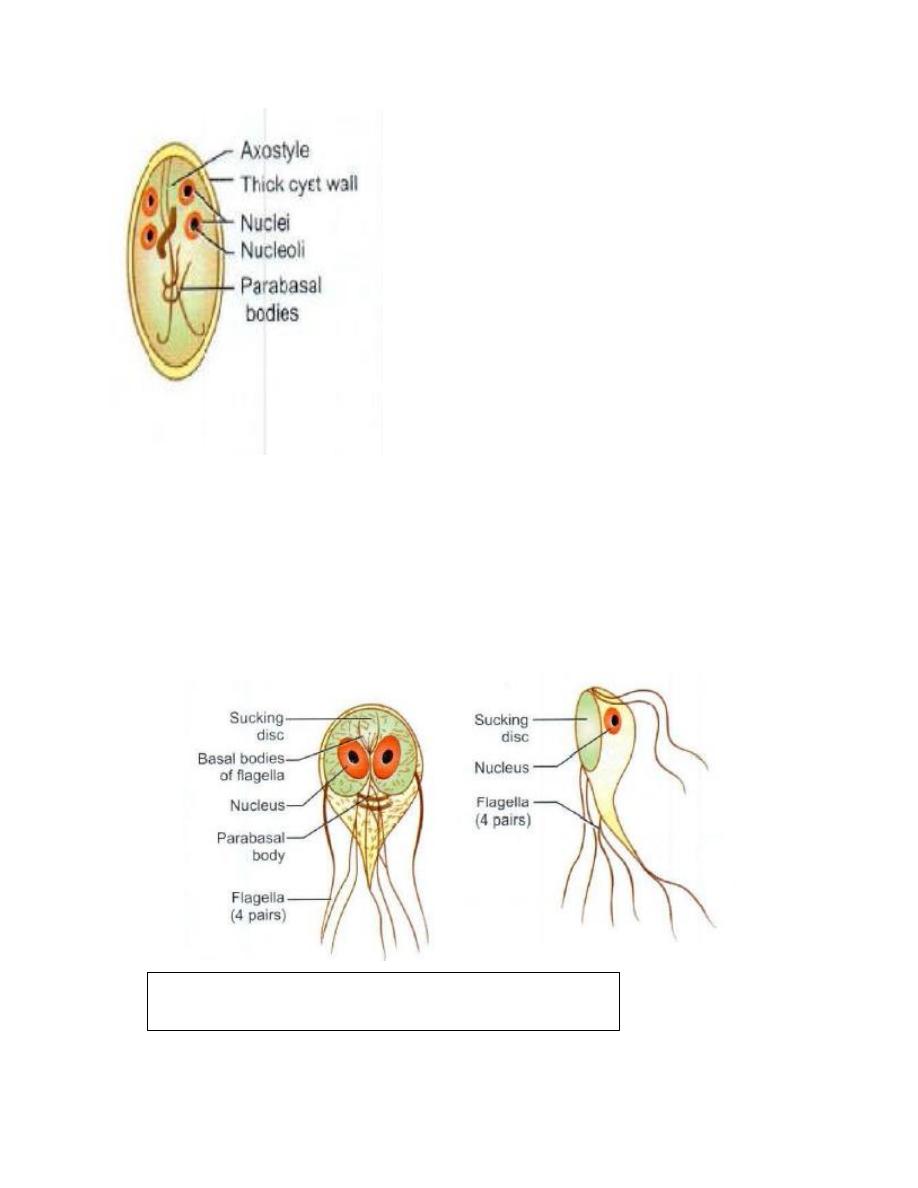
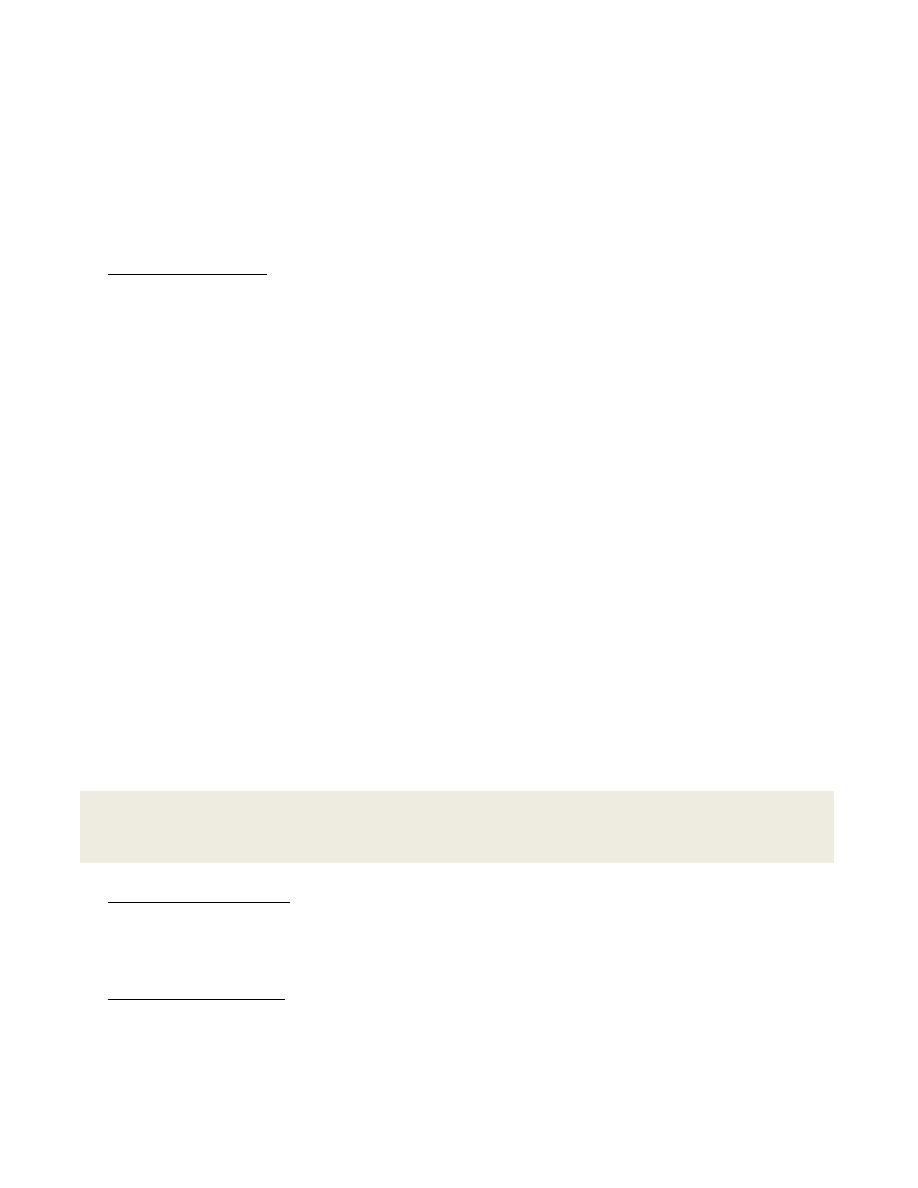
B. Trophozoite:
It is teardrop-shaped (or tennis racket), measures 9-21 by 5-15 µm.
The trophozoite has a convex dorsal surface and a flat ventral surface that
contains the ventral disk.
The trophozoite has long axostyles, 4 pairs of flagella, directed posteriorly,
that aid the parasite in moving.
Two symmetric nuclei with prominent karyosomes produce the
characteristic face like image that appears on stained preparations.
G. lamblia cyst.(1)
Trophozoite of G. lamblia.(1)
College of Medicine University of Mosul /Department of: Microbiology
Subject: Parasitology Stage: 3
rd
2021-2022
Dr. Ahmed Al harbi Date: 15/11/2021 No. 1
Pa
ge
3
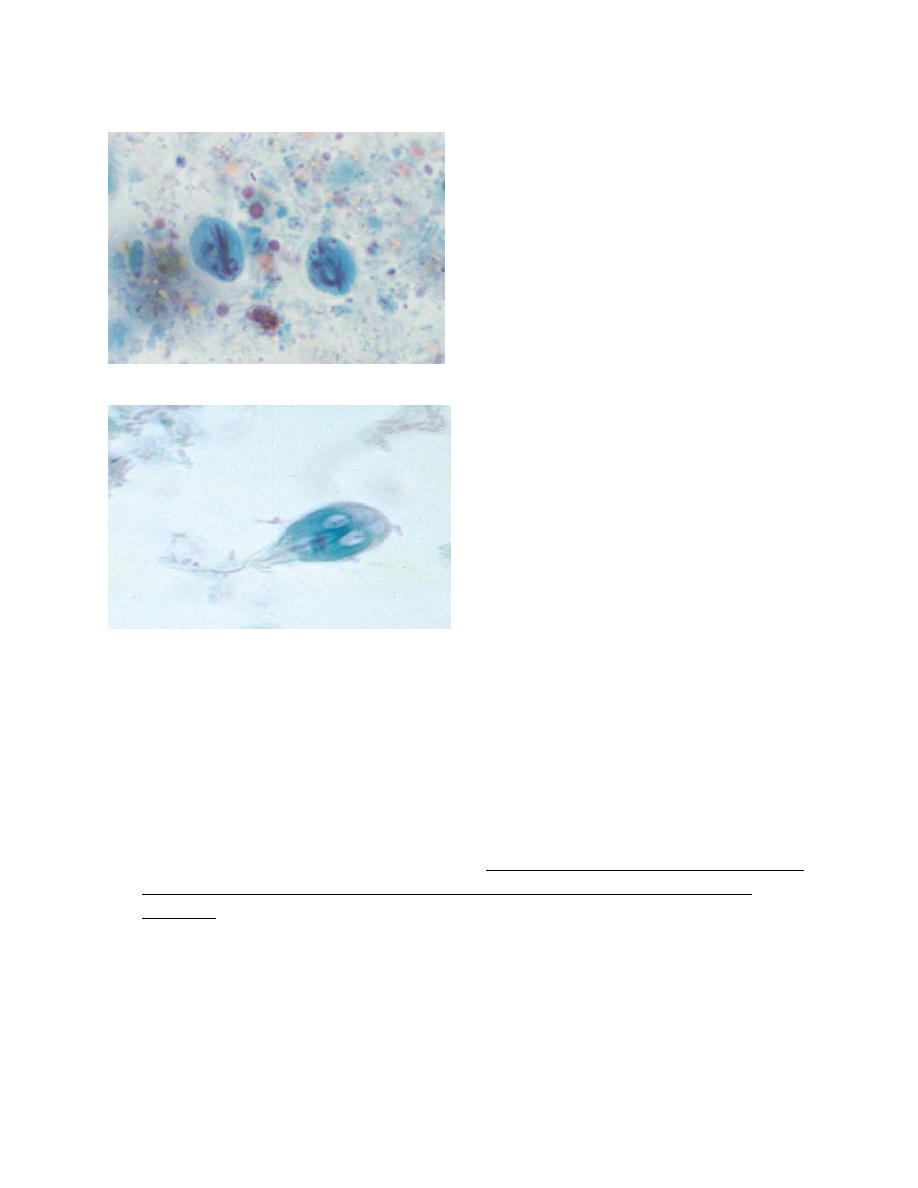
Giardia intestinalis cyst. Note red-stained nuclei (trichrome stain, ×1000). (2)
Giardia lamblia trophozoite under microscope. (3)
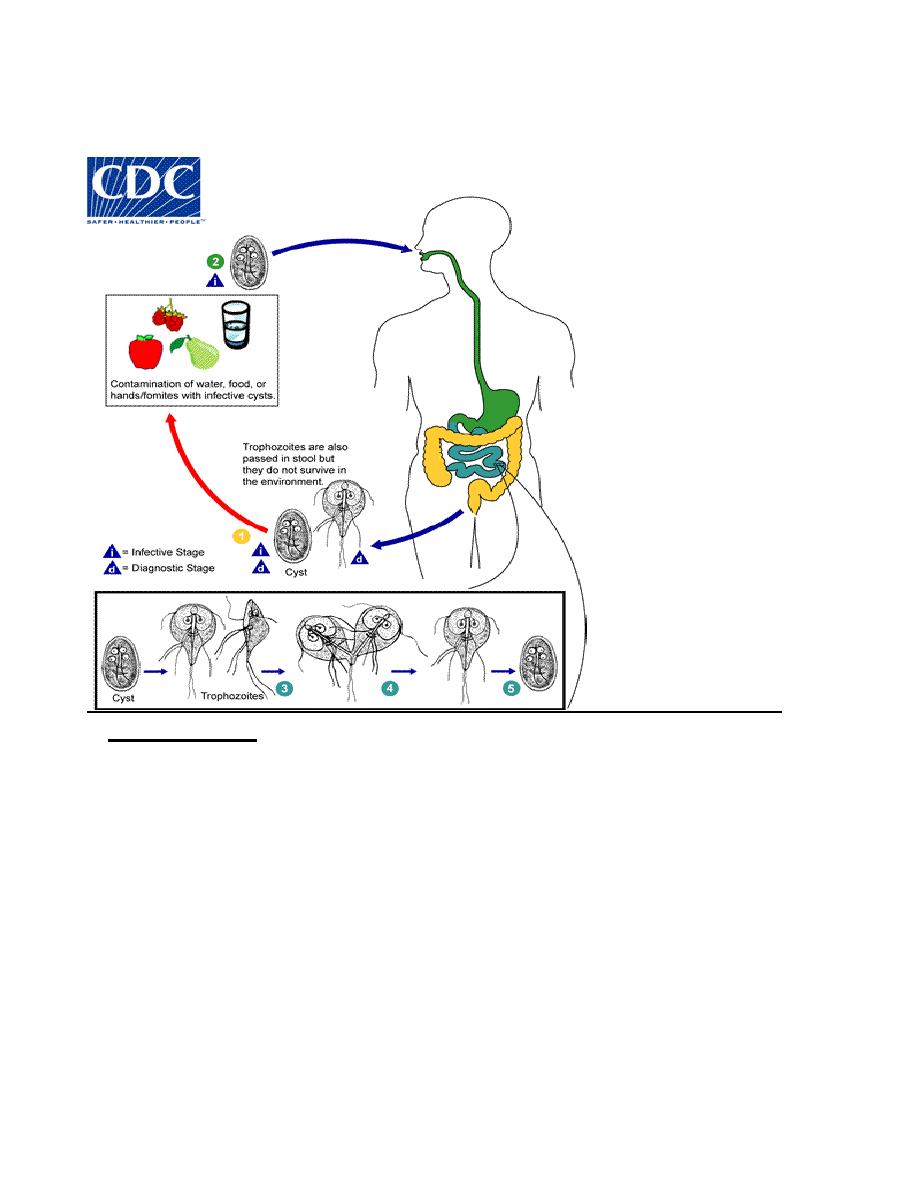
Life cycle
Mature cyst (the infective stage) is found on surfaces; in soil, food and water
that have been contaminated with feces from infected individuals.
Trophozoites can also be found in feces (both regarded as diagnostic stages)
.
Giardia cyst is protected by an outer shell that allows it to survive outside the
body for long periods of time and makes it tolerant to chlorine disinfection.
The cysts are hard and can survive several months in cold water.
Life cycle starts upon ingestion of cysts. Because the cysts are infectious when
passed in the stool or shortly afterward, person-to-person transmission is
possible.
Excystation occur in the small intestine releasing trophozoites (each cyst
produces two trophozoites).
Trophozoites multiply by longitudinal binary fission, remaining in the lumen
of the proximal small bowel where they can be free or attached to the mucosa
by a ventral sucking disk.
College of Medicine University of Mosul /Department of: Microbiology
Subject: Parasitology Stage: 3
rd
2021-2022
Dr. Ahmed Al harbi Date: 15/11/2021 No. 1
Pa
ge
4
Encystation (formation of cysts) occurs as the parasites pass to the colon. The
cyst is the stage that is found most commonly in non-diarrheal feces.
Life cycle of G.lamblia.(4)
Epidemiology:
Transmission of infection
Worldwide, more prevalent in warm climates, especially among children.
Giardia intestinalis has been isolated from the stools of beavers, dogs, cats,
and primates.
Beavers may act as reservoir host for G. intestinalis.
Giardia can be picked up from:
• Surfaces (such as bathroom handles, changing tables, or toys) that contain
feces (poop) from an infected person or animal.
• Drinking water or using ice made from water sources where Giardia may
live (for example, untreated or improperly treated water from lakes, streams,
or wells)
• Swallowing water while swimming or playing in water where Giardia may
live, especially in lakes, rivers, springs, ponds, and streams
College of Medicine University of Mosul /Department of: Microbiology
Subject: Parasitology Stage: 3
rd
2021-2022
Dr. Ahmed Al harbi Date: 15/11/2021 No. 1
Pa
ge
5
• Eating uncooked food that contains Giardia organisms
• Having contact with someone who is ill with giardiasis
• Traveling to countries in which giardiasis is common
Pathogenicity and clinical picture:
Pathogenicity
The mechanisms by which Giardia causes diarrhea and intestinal
malabsorption are probably multi-factorial.
The proposed pathological mechanisms include: damage to the epithelial
brush border, enterotoxins, immunological reactions, altered gut motility,
fluid hyper secretion, and loss of sacharidase enzymes.
Variant-specific surface proteins (VSSPs) of Giardia play an important role
in virulence and infectivity of the parasite. Antigenic variation helps the
parasite in evasion of host immune system.
Risk factors for infection
Being a child.
Male homosexuality
Mentally illness
Blood group A,
Achlorhydria,
Use of Cannabis
Chronic pancreatitis
Malnutrition and immune defects such as 1gA deficiency and
hypogamma globulinemia. Patients with cystic fibrosis and living in
crowded areas.
Clinical picture:
A symptomatic
Acute giardiasis:
It develops after an incubation period of 1 to 14 days (average of 7 days) and
usually lasts 1 to 3 weeks. Acute symptoms include:
Diarrhea, gases, greasy stools that tend to float (steatorrhea), abdominal cramps,
GIT upset or nausea/vomiting, and dehydration (loss of fluids).
The symptoms of giardiasis might seem to resolve, but come back again after
several days or weeks. Giardiasis may be mild and self limited or can cause
weight loss and malabsorption.
Giardiasis in children
Severe giardiasis might delay physical and mental growth, slow development,
growth retardation and malnutrition.
College of Medicine University of Mosul /Department of: Microbiology
Subject: Parasitology Stage: 3
rd
2021-2022
Dr. Ahmed Al harbi Date: 15/11/2021 No. 1
Pa
ge
6
Chronic Giardiasis:
Cases of giardia infection may resemble IBS usually diagnosed by finding cysts in
the stool of patients. Occasionally, Giardia colonizes the gallbladder, causing
biliary colic and jaundice.
Diagnosis:
Stool examination:
The traditional basis of diagnosis is the detection of G. intestinalis
trophozoites or cysts in the stool of infected patients via a stool ova and
parasite (O&P, i.e. general stool examination) examination.
Fresh stool can be mixed with an iodine solution or methylene blue and
examined for cysts on a wet mount.
If not immediately examined, stool should be preserved in 10% formalin,
with subsequent trichrome or iron hematoxylin staining.
Trophozoites may be seen in fresh watery stool but difficult because they
disintegrate rapidly. If the stool is not fresh or is semi formed to formed,
trophozoites will not be found.
Cysts passed in soft and formed stools.
Ideally, 3 stool samples from each patient on different days should be
examined because of potential variations in fecal excretion rate of cysts.
G intestinalis is identified in 50-70% of patients after a single stool
examination and in more than 90% after 3 stool examinations.
Stool concentration methods are used when there is low excretion rate of
cysts.
Cyst passage may lag behind the onset of symptoms by a week or more.
Because many antibiotics, enemas, laxatives, and barium studies mask or
cause, the disappearance of parasites from the stools, microscopic
examination should be postponed for 5 days following these interventions.
Duodenal Aspiration:
It is done by aspiration of duodenal contents and demonstration of trophozoites.
It is more invasive than stool examination and, may have a lower diagnostic yield.
Immunological tests:
Stool antigen enzyme-linked immunosorbent assays are highly sensitive.
Direct Immunofluorescence Assay (DFA) can be used to show the parasites
in stool samples.
Note
: Trophozoites are best to be examined by permanent staining
techniques ( trichrome stains).

College of Medicine University of Mosul /Department of: Microbiology
Subject: Parasitology Stage: 3
rd
2021-2022
Dr. Ahmed Al harbi Date: 15/11/2021 No. 1
Pa
ge
7
Since levels of serum immunoglobulin G (IgG) remain elevated for long
periods, they are not beneficial in making diagnosis of acute giardiasis.
Serum anti-Giardia immunoglobulin M (IgM) can be beneficial in
distinguishing between acute infections and past infections (serology is not
part of routine lab examination for Dx of G. lamblia).
Treatment:
Single dose of tinidazole 2 g, or metronidazole 400 mg 3 times daily for 10
days, or nitazoxanide 500 mg orally twice daily for 3 days.
Paromomycin has been recommended for use in pregnancy because systemic
absorption is low, but the cure rate is lower than other agents.
Prevention:
Proper hand wash with soap and good sanitation.
Infected individuals not allowed using swimming pools, lakes, and rivers
until they are symptom-free for few weeks.
Chlorination, sedimentation, and filtration methods should be implemented
adequately to purify public water supplies. Drinking water can be boiled for
at least 5 minutes. Chlorine or iodine water treatments are less effective than
boiling or filtration, but they may be used as alternatives.
Advice travelers to endemic areas to avoid eating uncooked foods that may
have been grown, washed, or prepared with contaminated water.
Breastfeeding appears to protect infants from infection. Breast milk contains
detectable titers of secretory IgA, which is protective for infants.
Summary:
G. lamblia is
the only protozoan parasite found in the lumen of the human
small intestine.
Exists in two morphological forms (cyst and trophozoite)
Mature cyst is the infective stage which is transmitted orally
Causes, acute gastroenteritis or chronic condition
Most commonly diagnosed by stool smear
Treated by tinidazole or metronidazole
Prevention is important to decrease burden of transmission of disease

College of Medicine University of Mosul /Department of: Microbiology
Subject: Parasitology Stage: 3
rd
2021-2022
Dr. Ahmed Al harbi Date: 15/11/2021 No. 1
Pa
ge
8
References:
1.
Paniker J CK , 2018, Paniker
,
s textbook of medical parasitology, 8
th
edition, Newdelhi, London , Panama, JAYPEE.
2.
Zeibig A. Elizabeth, 2013, Clinical parasitology, USA, Elsevier
3.
‘Forbes BA, Sahm DF,Weissfeld AS: Bailey & Scott’s diagnostic microbiology, ed 12, St Louis, 2007, Mosby’
4.
CDC.gov
5.
BURTON J. Bogitsh,Clint E. Carter, and Thomas N. Oeltmann, 2013, Human parasitology 4
th
edition, USA and UK,
Elsevier.
6.
Dickson D. Despommier, Daniel O. Griffin, Robert W. Gwadz, Peter J. Hotez, and Charles A. Knirsch. Parasitic diseases
6
th
edition.New yourk Parasites Without Borders, Inc. NY.
7.
Hayden Randall , Wolk Donna, Caroll Karen and Tang Yi. DIAGNOSTIC MICROBIOLOGY
IMMUNOCOMPROMISED HOST . , N.W., Washington, DC , USA. “nd edition.