Parasitology
Notes…
1
Trematodes Lec.1
The helminthes are multicellular parasites (metazoa) bilaterally symmetrical animals
having three germ layers
• The term helminth (Greek helmins-worm) originally referred to intestinal worms, but now
comprises many other worms, including tissue parasites as well as many free-living
species.
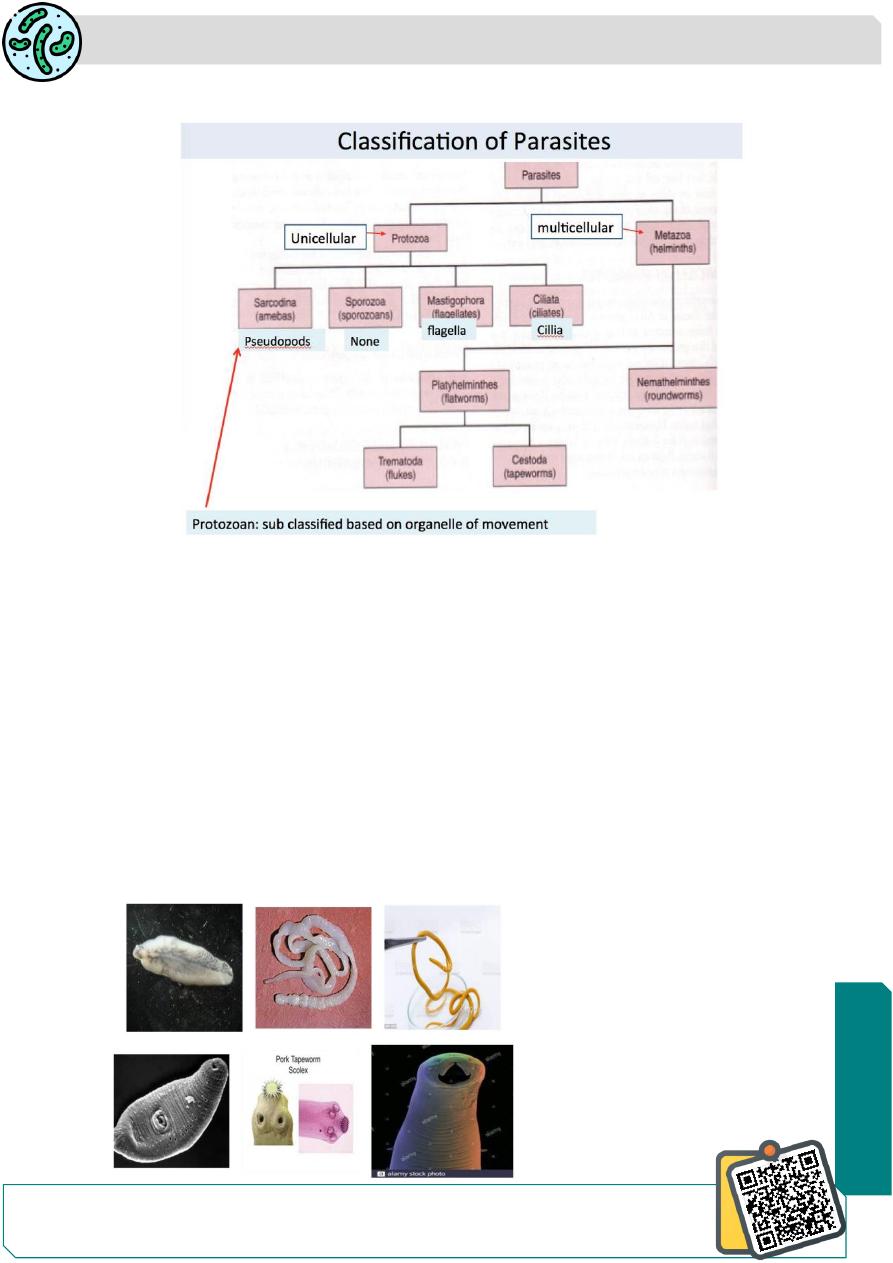
Helminths, which occur as parasite in humans, belong to two phyla
Phylum Platyhelminthes (flatworms): It includes two classes:
i.
Class: Trematoda (flukes or digeneans)
ii.
Class: Cestoda (tapeworms)
1.
2.
Phylum Nemathelminthes: It includes class nematoda
Need So
me
Help?
Parasitology
Notes…
2
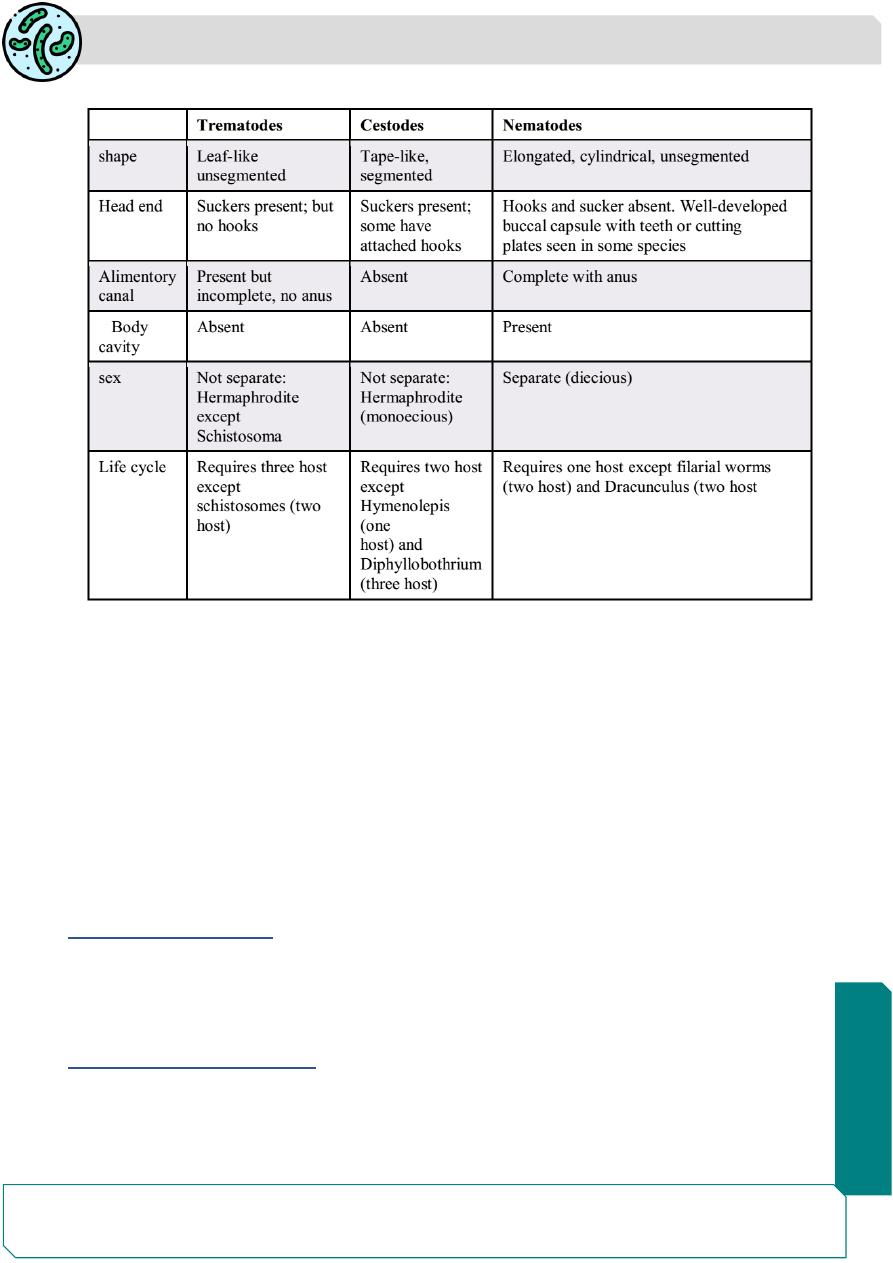
Table: features of different classes of helminthes
Trematoda or trematodes or Digenea.
Commonly known as the flukes, they belong to
Phylum Platyhelminthes ( flatworms)
Class Trematoda.
Classification of trematodes
The Classification of trematodes of medical importance is based on their habitat, the
trematodes may be placed into two categories, those that reside in the intestine, bile duct,
or lung (organ-dwelling) and those that reside in the blood vessels around the intestine
and bladder (blood-dwelling).
A. Blood (Blood fluke)
1. Schistosoma haematobium (In the vesical and pelvic venous plexuses)
2. Schistosoma mansoni (In the inferior mesenteric vein)
3. Schistosoma japonicum (In the superior mesenteric vein)
B. Biliary tract (Liver fluke)
1. Clonorchis sinensis
2. Opisthorchis viverrini
3. Fasciola hepatica
Parasitology
Notes…
3
C . Intestine (Intestinal fluke)
1. Fasciolopsis buski
2. Heterophyes heterophyes
3. Metagonimus yokogawai
D. Respiratory tract ( Lung fluke)
1. Paragonimus westermani
General characters:
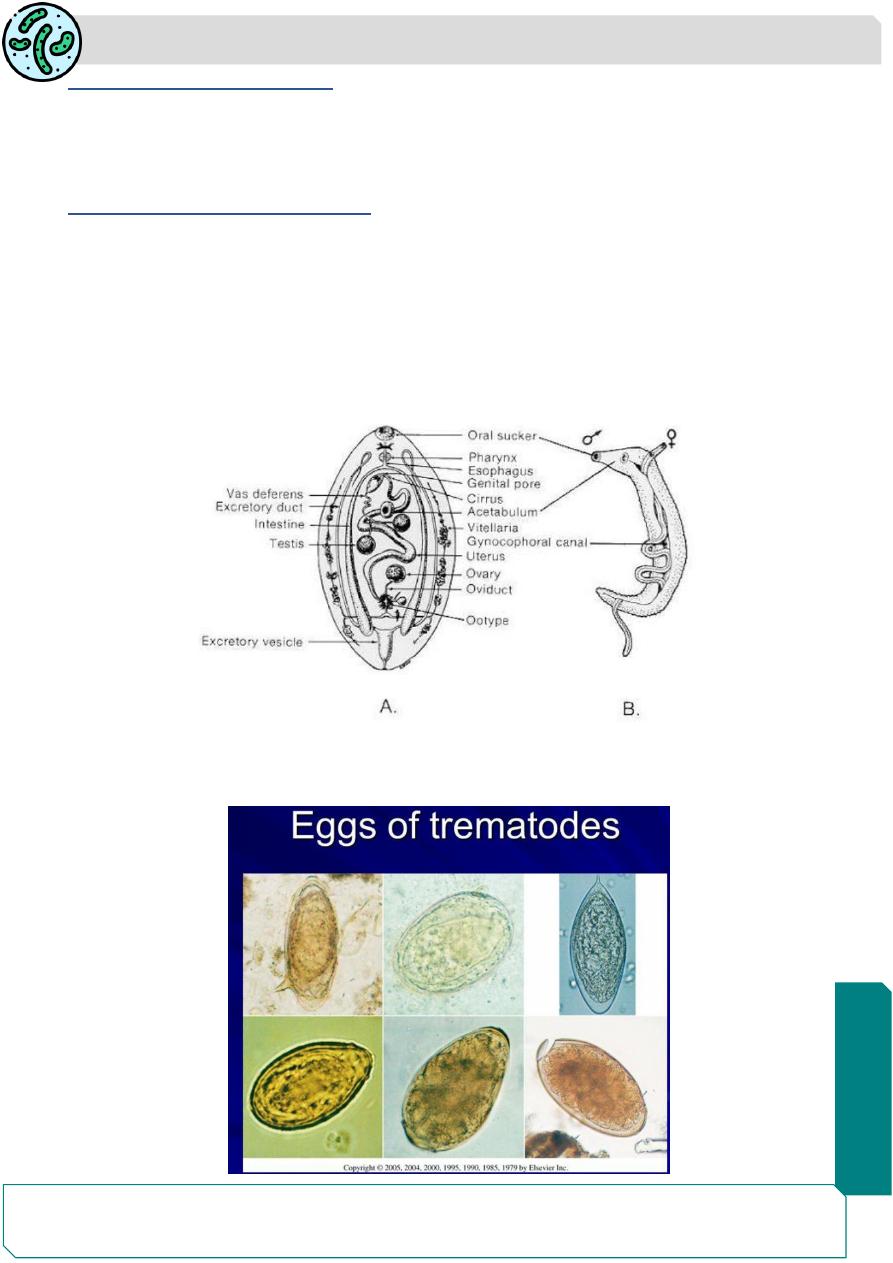
1. Trematodes are unsegmented helminths, flat, broad and leaf shaped. They have large
prominent suckers. The unique feature of flukes is the presence of two muscular cup-
shaped suckers (hence called distomata)the oral sucker surrounding the mouth at the
anterior end and the ventral sucker or acetabulum in the middle, ventrally
2. Trematodes are hermaphrodites except for schistosomes.
3. Their eggs are operculated except for schistosome eggs.

Parasitology
Notes…
4
4. Snails are the only intermediate host for schistosomes and are the
first intermediate host for other trematodes.
5. The miracidium is the 1 st stage larva is ingested by the snail within the egg or release
and penetrates the snail. The cercaria is the 2 nd stage larva that develop in the redia
(cylindrical larva) then attached to aquatic plants or aquatic organisms and develops into
metacercaria.
6. Metacercaria (tailless encrusted larva) is the infective stage for trematodes except for
schistosomes whereby cercariae is the infective stage.
7. The outer surface of the fluke is called the tegument. This is composed of
scleroprotein,.The tegument is the host-parasite interface, and metabolically active body
covering performing all the vital activities such as protection, absorption and secretion
Parasitology
Notes…
5
Blood flukes ( schistosomes)
There are three main species of blood flukes that are primarily associated with disease
in humans (known as schistosomiasis, bilharziasis, or snail fever), all belonging to the
genus Schistosoma.
These three species are
1. Schistosoma haematobium
2. Schistosoma japonicum (Oriental blood fluke)
3. Schistosoma mansoni.
The blood flukes differ in morphology and life cycle characteristics from the other
trematodes. They are similar, however, by requiring a freshwater snail as the intermediate
host. Schistosomiasis is devastating tropical disease ,being a major source of morbidity
and mortality for developing countries in Africa, South America, the Caribbean, the Middle
East, and Asia.
Schistosoma haematobium
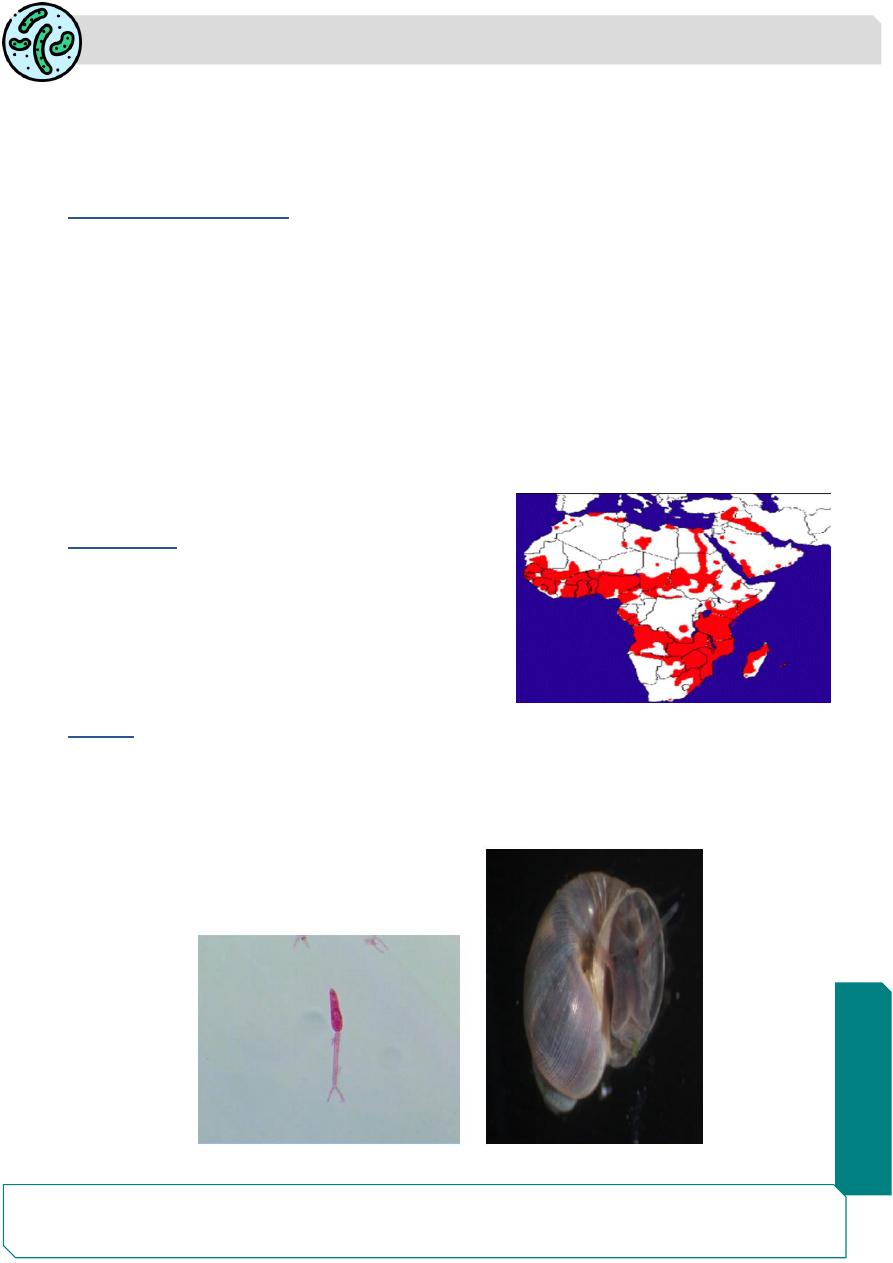
Distribution
Schistosoma haematobium has been known to
occur primarily in the Old World. Almost all of
Africa and portions of the Middle East, including
Iran, Iraq, and Saudi Arabia are considered
endemic regions.
Habitat
The adult worms live in the vesical and pelvic venous plexuses of humans.
Intermediate host: snail genus Bulinus
Infective stage :bifurcated tail cercaria
Parasitology
Notes…
6
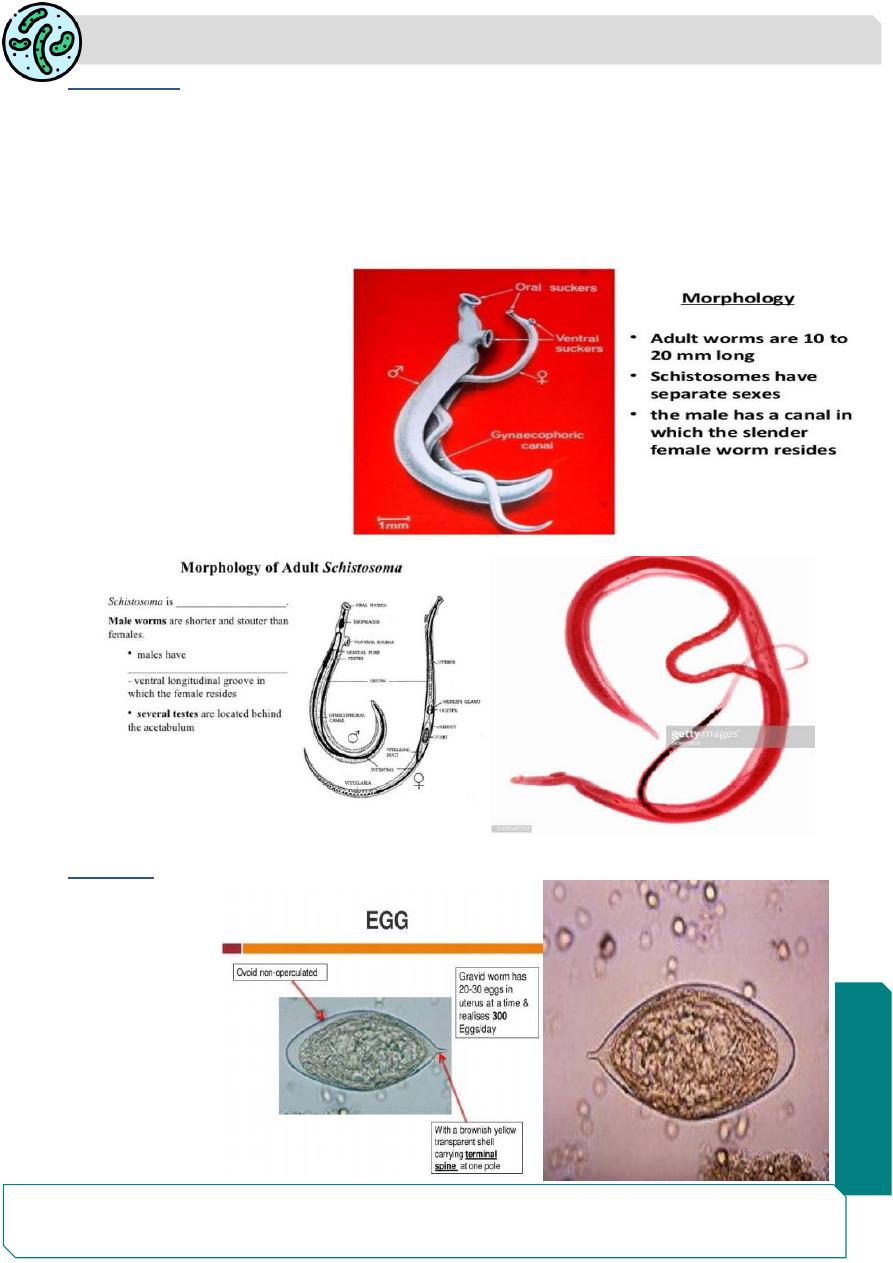
Morphology
The adult male worm is 10
–15 mm long by 1 mm thick and is covered by a finely
tuberculated cuticle.
It has 2 muscular suckers: a small oral sucker and a large prominent ventral sucker.
Immediately behind the ventral sucker and extending to the caudal end is the
gynecophoric canal, where the female worm is found.
The adult female is 20 mm by
0.25 mm with the cuticular
tubercles confined to the 2
ends.
The
gravid
female
worm
contains 20
–30 eggs in its
uterus
at
one
time
and may pass up to 300 eggs
a day.
The eggs
Are elongated,
about 150 μm
by 50 μm, non-
operculated,
with a terminal
spine contain
miracidium
(embryonated) .

Parasitology
Notes…
7
Mechanism of egg expulsion:
The eggs are laid usually in the small venules of the vesical and pelvic plexuses, though
sometimes they are laid in the mesenteric portal system, pulmonary arterioles and other
ectopic sites.
The eggs are laid one behind the other with the spine pointing posteriorly. From the
venules, the eggs make their way through the vesical wall by the piercing action of the
spine, assisted by the mounting pressure within the venules and a lytic substance
released by the eggs. The eggs pass into the lumen of the urinary bladder together with
some extravasated blood.
•they are discharged in the urine, particularly towards the end of micturition.
• For some unknown reasons, the eggs are passed in urine more during midday than at
any other time of the day.
• The eggs laid in ectopic sites generally die and evoke local tissue reactions. They may
be found, for instance in rectal biopsies, but are seldom passed live in feces.
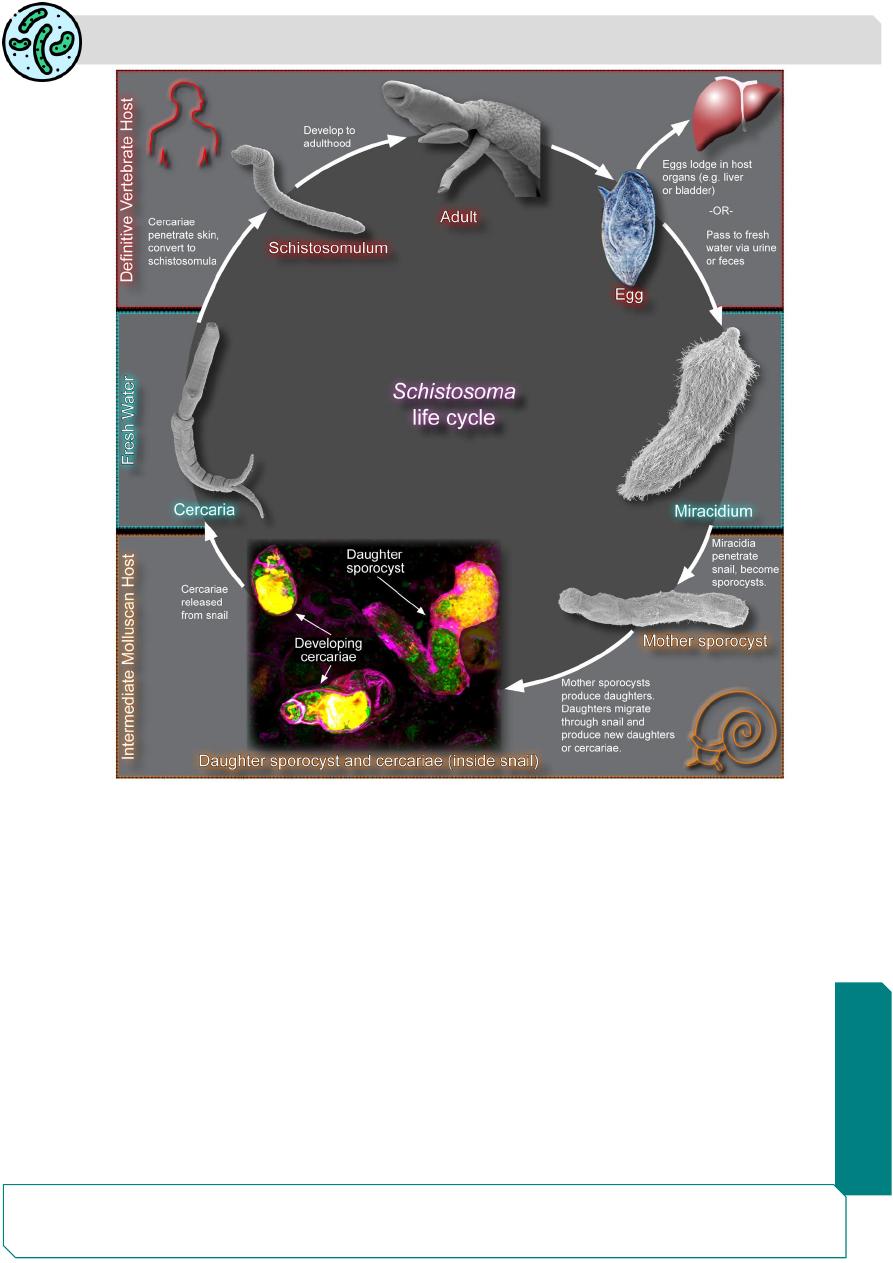
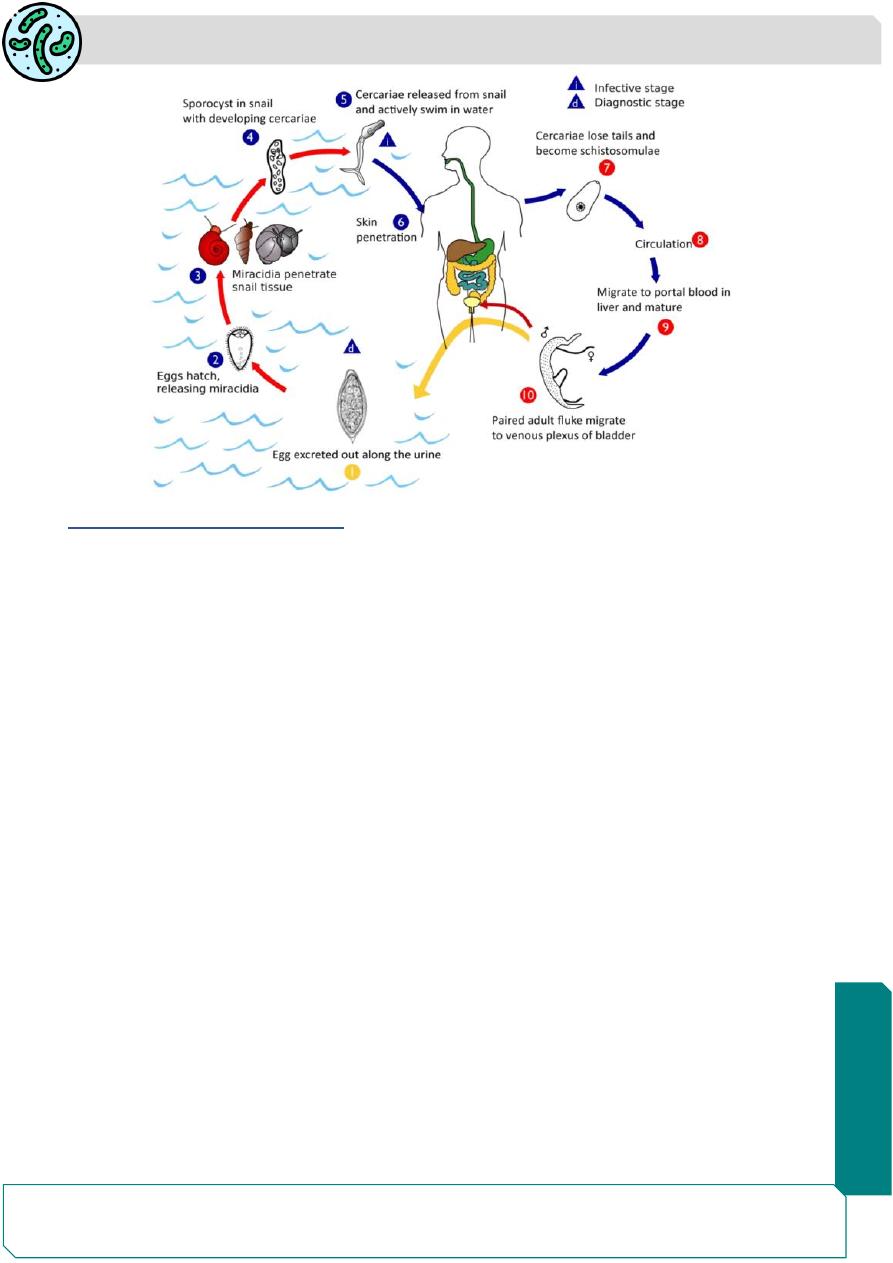
Life cycle
S. haematobium passes its life cycle in two hosts:
1. Definitive host: Humans are the only natural definitive hosts. No animal reservoir is
known.
2. Intermediate host: Freshwater snails (snail of the genus Bulinus).
Infective form:
Cercaria larva.
• The eggs that are passed in urine are embryonated and hatch in water under suitable
conditions to release the free-living ciliated miracidia.
• Miracidia swim about in water and on encountering a suitable intermediate host (snail
Bulinus species).
Development in snail:
Inside the snail, the miracidia lose their cilia and in about 4-8
weeks, successively pass through the stages of the first and second generation
sporocysts
• Large numbers of cercariae are produced by asexual reproduction within the second
generation sporocyst. The cercaria has an elongated ovoid body and forked tail
(bifurcated tail)
• The cercariae escape from the snail into water.
• Swarms of cercariae swim about in water for 1 -3 days. Persons become infected by
contact with water containing cercariae during bathing.
Suckers and lytic substances secreted by cercariae helps them to penetrated intact
skin.
Parasitology
Notes…
8
Development in man:
After penetrating the skin, the cercariae loss their tails and become
schistosomulae which travel via peripheral venules to systemic circulation.
• They then start a long migration, through the vena cava till it reaches the liver.
• In the intrahepatic portal veins, the schistosomulae grow and become sexually
differentiated
adolescents
about
20
days
after
skin
penetration.
• They then start migrating against the bloodstream into the inferior mesenteric veins,
ultimately reaching the vesical and pelvic venous plexuses, where they mature, mate and
begin laying eggs. Eggs start appearing in urine usually 10-12 weeks after cercarial
penetration.
The adult worms may live for 20- 30 years.
Parasitology
Notes…
9
Clinical stages and Pathology
✓ Asymptomatic. It is believed that most chronic Schistosoma infections contracted in
known endemic areas remain asymptomatic.
✓ Schistosomiasis, Bilharziasis. Schistomiasis can be divided into three phases:
(1) The Prepatent stage migratory phase lasting from penetration to maturity which will
be in the form of Cercarial dermatitis patient will be presents with transient itching and
petechial lesions at the site of entry of the cercariae , more often seen in visitors to
endemic areas than among locals who may be immune due to repeated exposure. It last
for 1 week and it is called (swimmer's itch)
(2) The acute phase which occurs when the schistosomes begin producing eggs, Clinical
features during oviposition include painless terminal haematuria. Haematuria is initially
microscopic, but become gross in heavy infection. Patients develop frequency of
micturition with burning sensation. Cystoscopy shows hyperplasia and inflammation of
bladder mucosa. In endemic regions, haematuria is so widespread that it is thought a
natural sign of puberty for boys, and is confused with menses in girls.
Katayama fever (more common with S. japonicum and S. mansoni than S. haematobium)
is a systemic hypersensitivity reaction to the schistosomulae migrating through tissue and
deposition of ova in the host tissue. It is presented with rapid onset of fever, nausea,
myalgia, malaise, fatigue, cough, diarrhea, and eosinophilia occur 1 to 2 months after
exposure. Although rare in chronically exposed persons, it is common in people new to
endemic areas, such as tourists and travelers.

Parasitology
Notes…
10
(3) The chronic phase which occurs mainly in endemic areas many of the eggs die and
become calcified eventually producing fibrosis of vesical mucosa and formation of egg
granulomas (sandy patches). which may lead to urinary tract blocking leading to
obstructive uropathy (hydroureter and hydronephrosis), which can be further complicated
by bacterial infection and kidney failure. In the most severe condition, chronic bladder
ulcers and bladder carcinoma develop.
Organized by:
Mustafa Mahmood Hashim