
Trematodes lec 2
د. اسماء زكي شيتاوي
Pathology of Schistosoma haematobium
The pathology of chronic schistosomiasis, which is far more common
than the acute form of the infection, results from egg-induced immune
response, granuloma formation, and associated fibrotic changes .
The eggs induce a granulomatous host immune response which is
indicated by lymphocytes , eosinophils, and, also activated macrophages.
This granuloma formation induces chronic inflammation.
Although cercarial and adult worms are minimally immunogenic,
schistosomal eggs are highly immunogenic and induce vigorous
circulating and local immune responses. Adult worms can absorb host
proteins. If not attacked by the immune system, they can live for years in
the blood stream as they are coated with host antigens.
Egg retention and granuloma formation in the urinary tract can lead to
bladder polyps and ulcer.
S haematobium infection is also associated with an increased rate of
bladder cancer, usually squamous cell rather than transitional cell.
Ectopic egg deposition can lead to additional clinical syndromes,
including involvement of skin, lungs, brain, muscles, adrenal glands,
genitalia, and eyes.
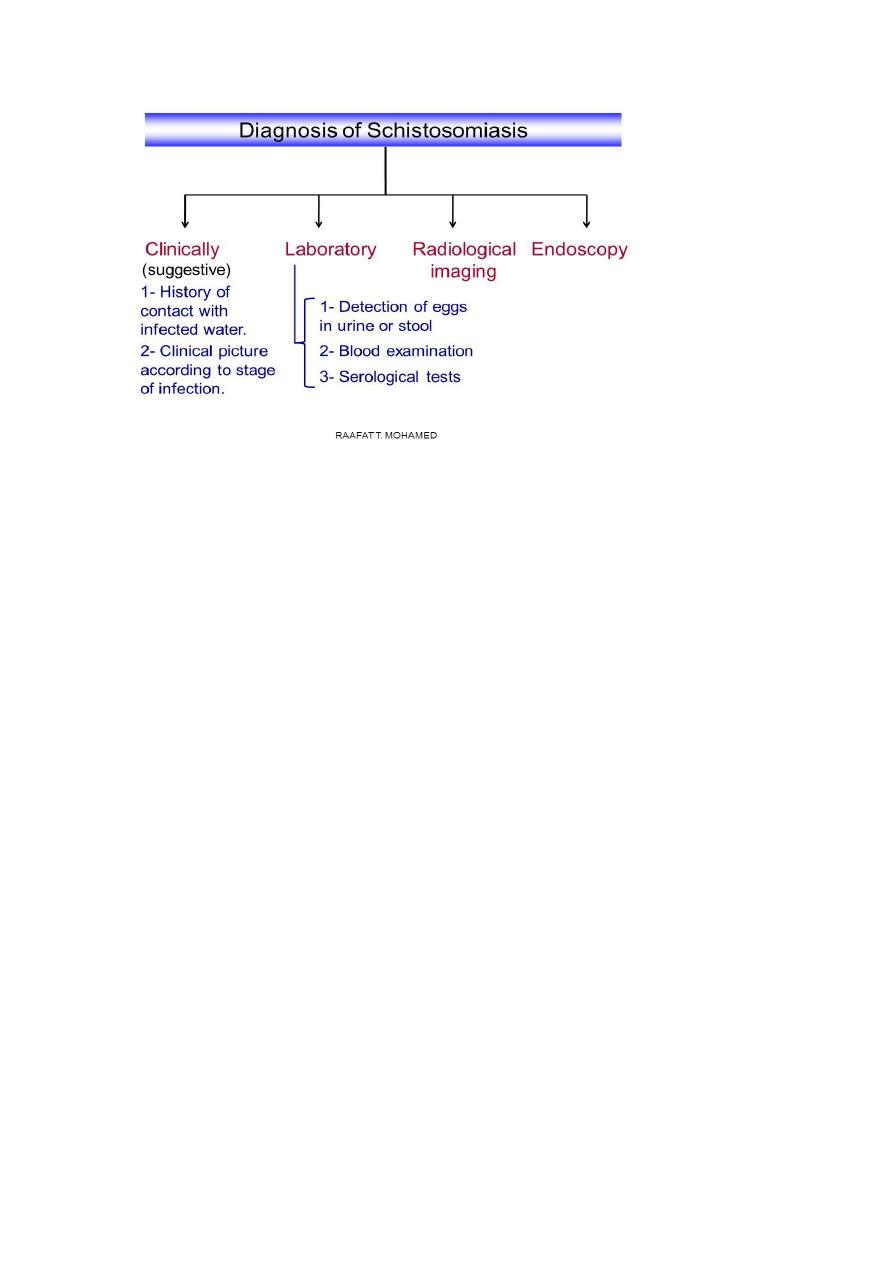
Diagnosis
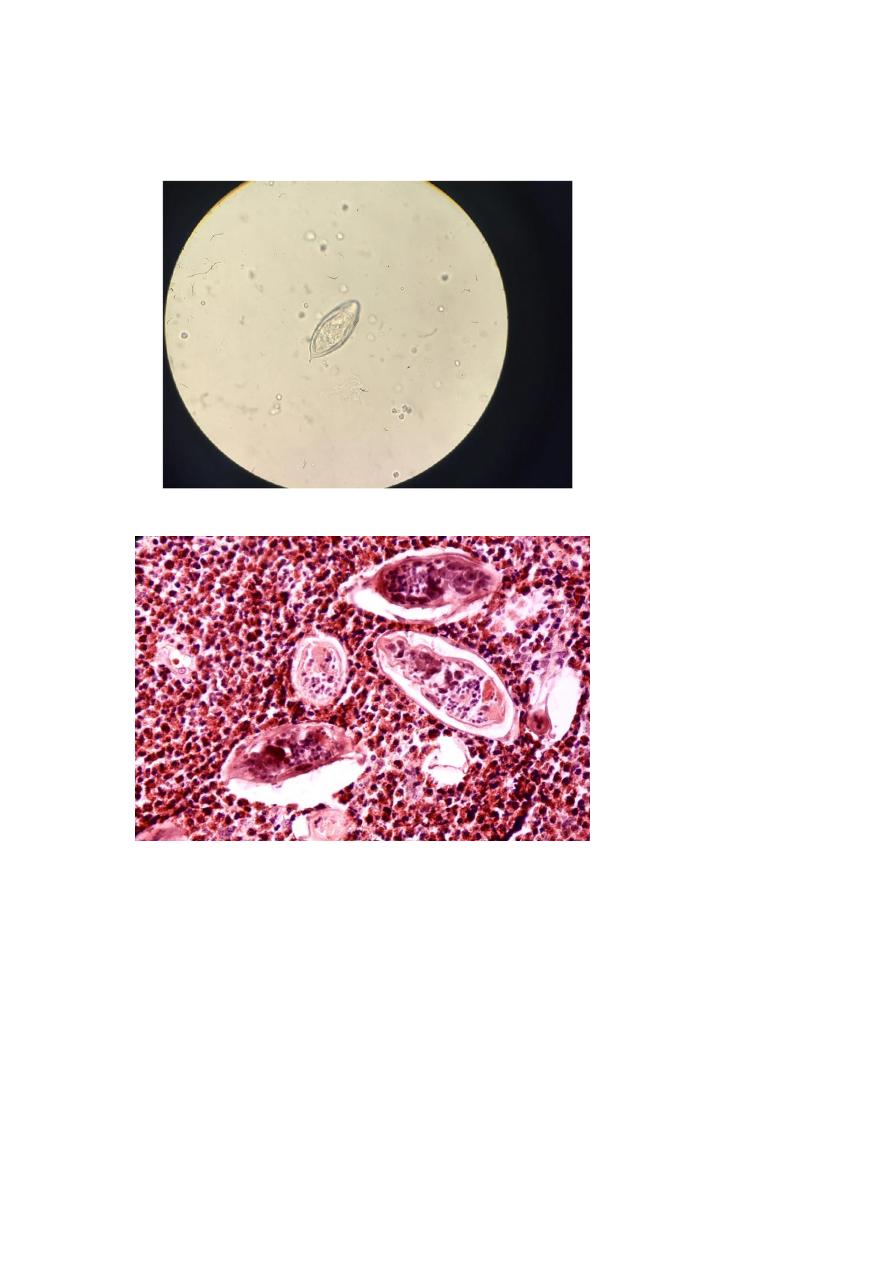
1. Microscopic examination: Detection of eggs with characteristic
terminal spines in centrifuged urine sample. Eggs which are
deposited in rectum may be occasionally found in faeces.
To
optimize recovery of S. haematobium in urine, the specimen should
be collected between noon and 2 pm
(10 am to 2 pm).
2. Biopsy Bladder mucosa or rectal biopsies to demonstrate eggs.
3. Imaging x-ray to detect calcification f bladder. Ultra sound and IVP
(intravenous pylograph) shows complication hydronephrosis and
hydroureter.
4. Detection of schistosomal antibodies using ELISA. Cannot
differentiate between past and recent infections.
5. Detection of antigen in the urine or serum.
6. Molecular diagnosis: PCR on clinical samples.
Treatment
Praziquantel (40 mg/kg/day orally in 2 divided doses for 1 day) is the
drug of choice.
Metrifonate is the alternative drug.
Prevention and Control
1. Proper disposal of urine and faeces.
2. Treatment of infected persons.
3. Avoid swimming, bathing and washing in snail-infested water
4. Control of snails

Schistosoma mansoni
Distribution
It is widely distributed in Africa, South America and the Caribbean
islands.
Habitat Adult worm lives in the inferior mesenteric vein.
Definitive host: man
Intermediate host : fresh water snail genus Biomphilarai
Infective stage: bifurcated tail cercaria
Morphology
Schistosoma mansoni resembles S. haematobium in morphology, except
the adult worms are smaller and their integuments are covered with
coarse tubercles. The uterus of the gravid female contains very few eggs
(1–3 only).
The egg is similar to that of Schistosoma haematobium except it has a
lateral spine .
The worm passes about 350 egg /day
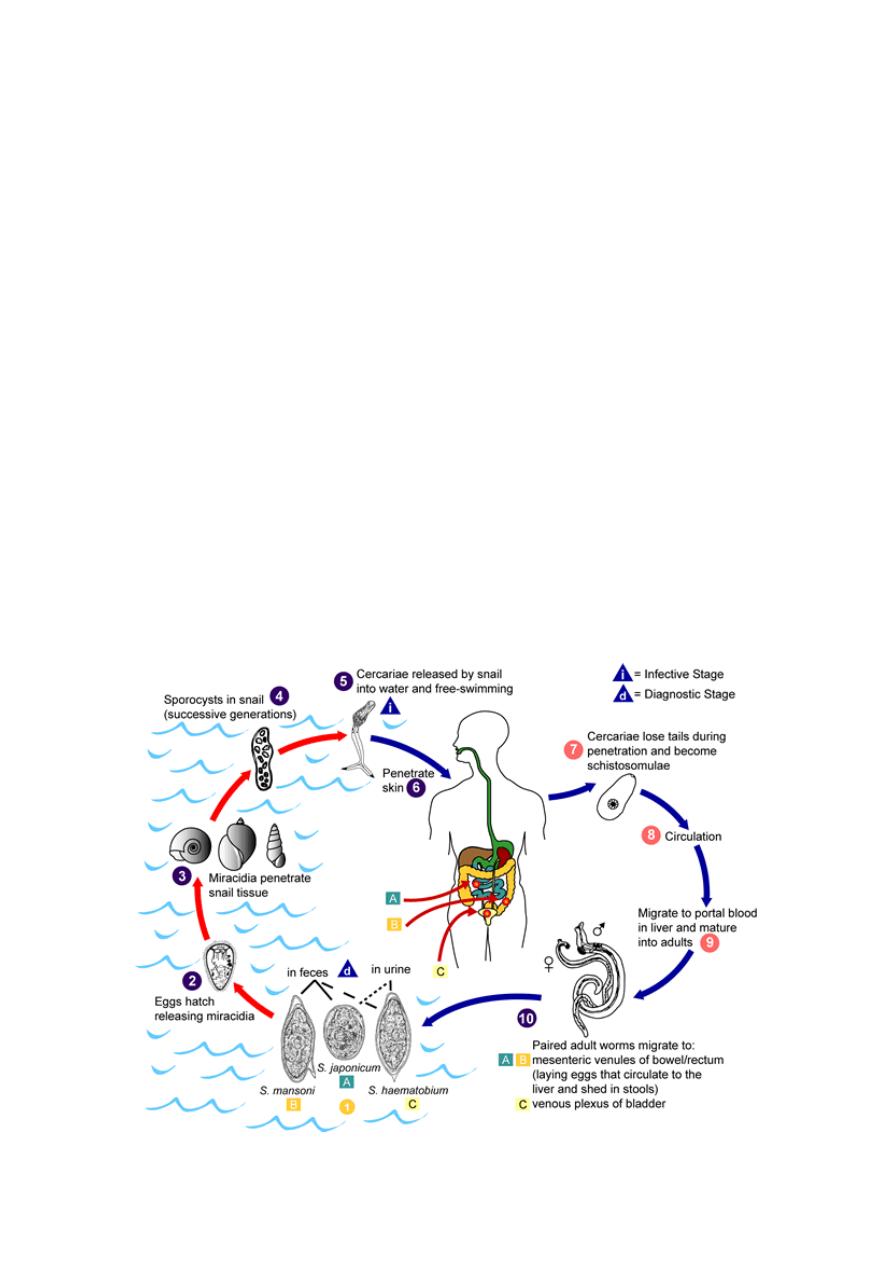
Life Cycle
Similar to S. haematobium except that Adult
worms in humans reside in
the mesenteric venules in various locations, it occurs more often in the
inferior mesenteric veins draining the large intestine and when it
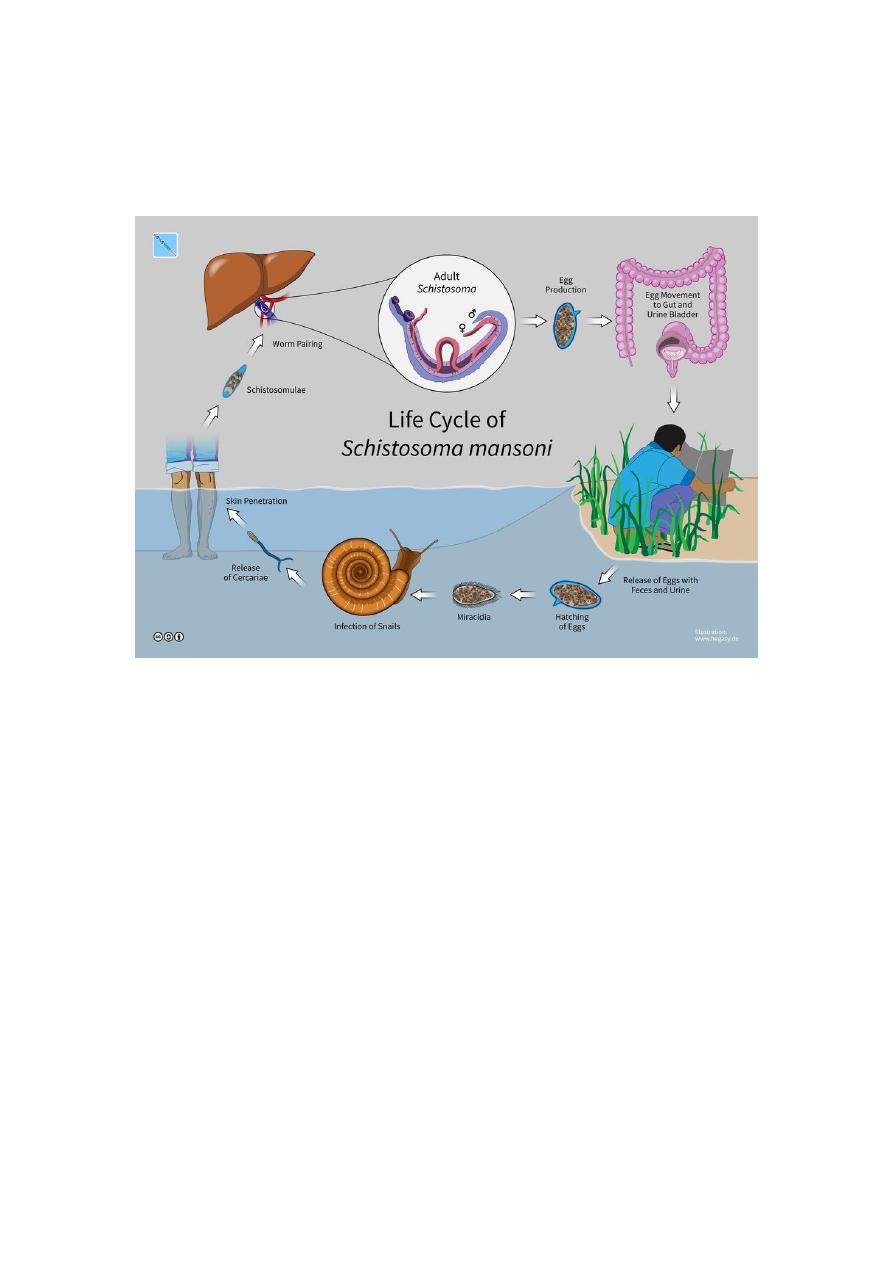
deposited the eggs are moved progressively toward the lumen of the
intestine.
Pathogenesis and Clinical Features
1.
The prepatent stage begins with cercarial invasion and ends with
initiation of egg laying. Cercarial dermatitis may develop after skin
penetration by the cercariae .It is self-limiting.
2.
Acute stage Katayama fever may develop in acute infection.
Symptoms of schistosoma mansoni are mainly intestinal. Patients
develop colicky abdominal pain and dysentery, which may persist
intermittently for many years
3.
Chronic stage: The eggs deposited in the intestinal wall of colon
and rectum, cause inflammatory reactions causing granulomas,
hyperplasia and followed by fibrosis Chronic inflammation can
lead to bowel wall ulceration, hyperplasia, and polyposis with
heavy infection , eggs that are carried through portal circulation to
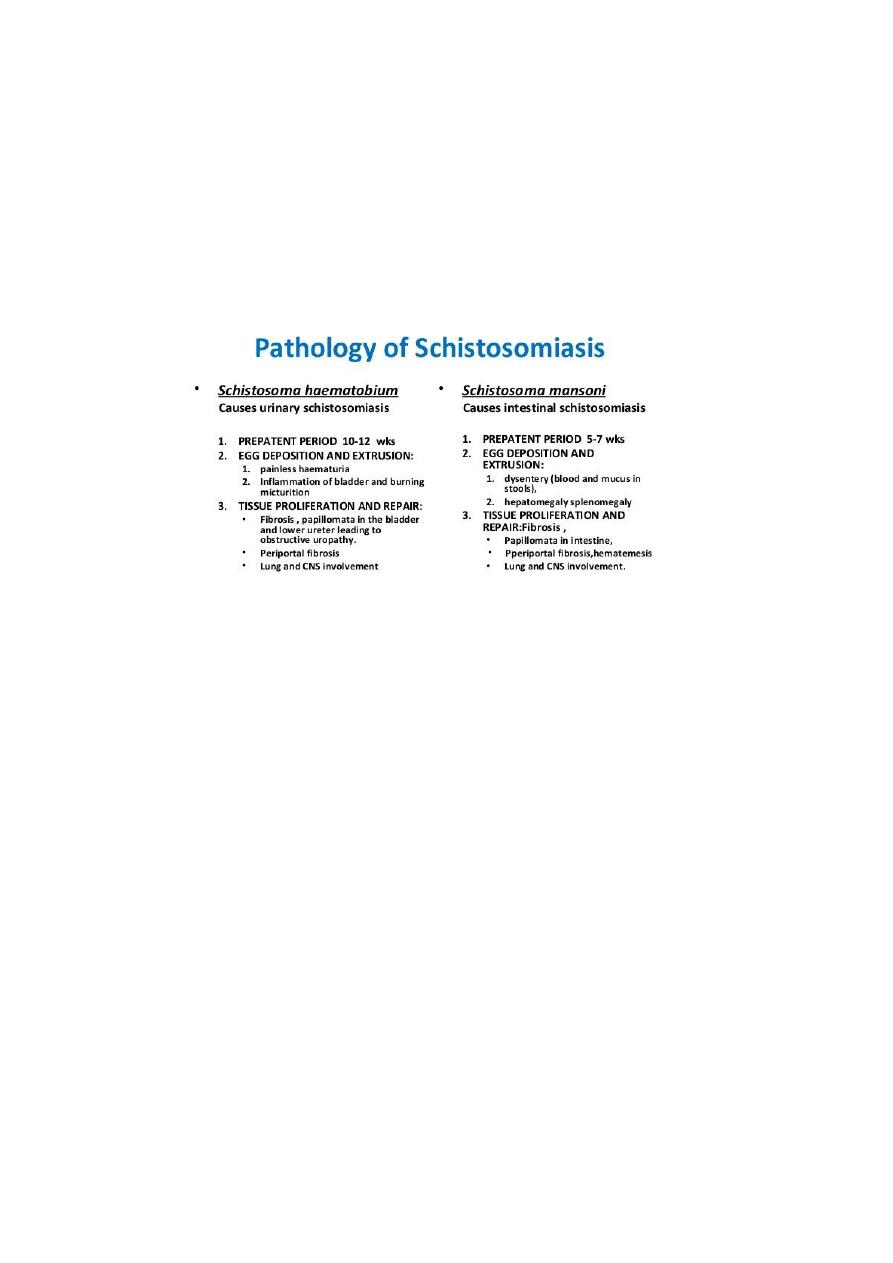
the liver may cause hepatosplenomegaly, periportal fibrosis
what
is called Symmer's fibrosis (also known as "clay pipe stem"
fibrosis, these occur due to intrahepatic portal vein calcification
which assume the shape of a clay pipe in cross section) and portal
hypertension.
Diagnosis
1. Microscopic examination
Detection of eggs with lateral spines in stool sample. Stool concentration
and sedimentation methods may be used in light infection.
2. Biopsy Biopsy of rectal mucosa to demonstrate eggs.
3. Serodiagnosis
4. Molecular diagnosis PCR on stool sample.
Treatment
Praziquantel (40 mg/kg/day orally in 2 divided doses for 1 day) is the
drug of choice, Oxamniquine is also effective
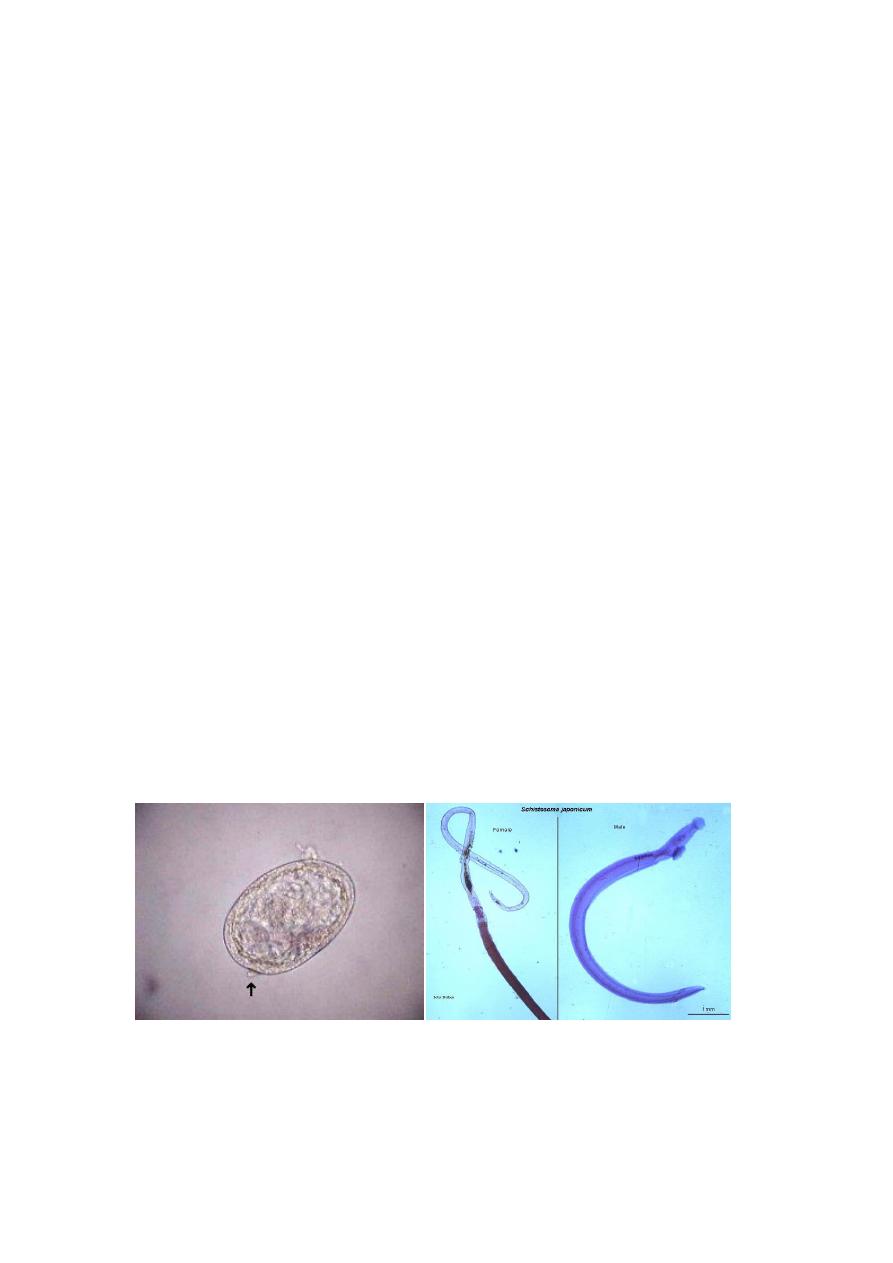
Schistosoma japonicum
Common name Oriental blood fluke
Distribution
Schistosoma japonicum is found in the Far East, Japan, China, Taiwan,
Philippines and Sulawesi.
Habitat
The adult worms are seen in the venules of the superior mesenteric vein.
Definitive host: man and domestic animals
Infective stage bifurcated tail cercaria
Morphology
Morphologically, they are similar to S. haematobium and S. mansoni
except the adult male is larger than other schistosomes comparatively
slender with smooth cuticle. The uterus of gravid female contains as
many as 100 eggs at one time and may pass out 3000 eggs daily.
The eggs of Schistosoma japonicum are smaller and more rounded than
other species, measuring 70-100 µm long by 55-64 µm wide. The spine
on S. japonicum eggs is smaller and less conspicuous than other species
(lateral knob).
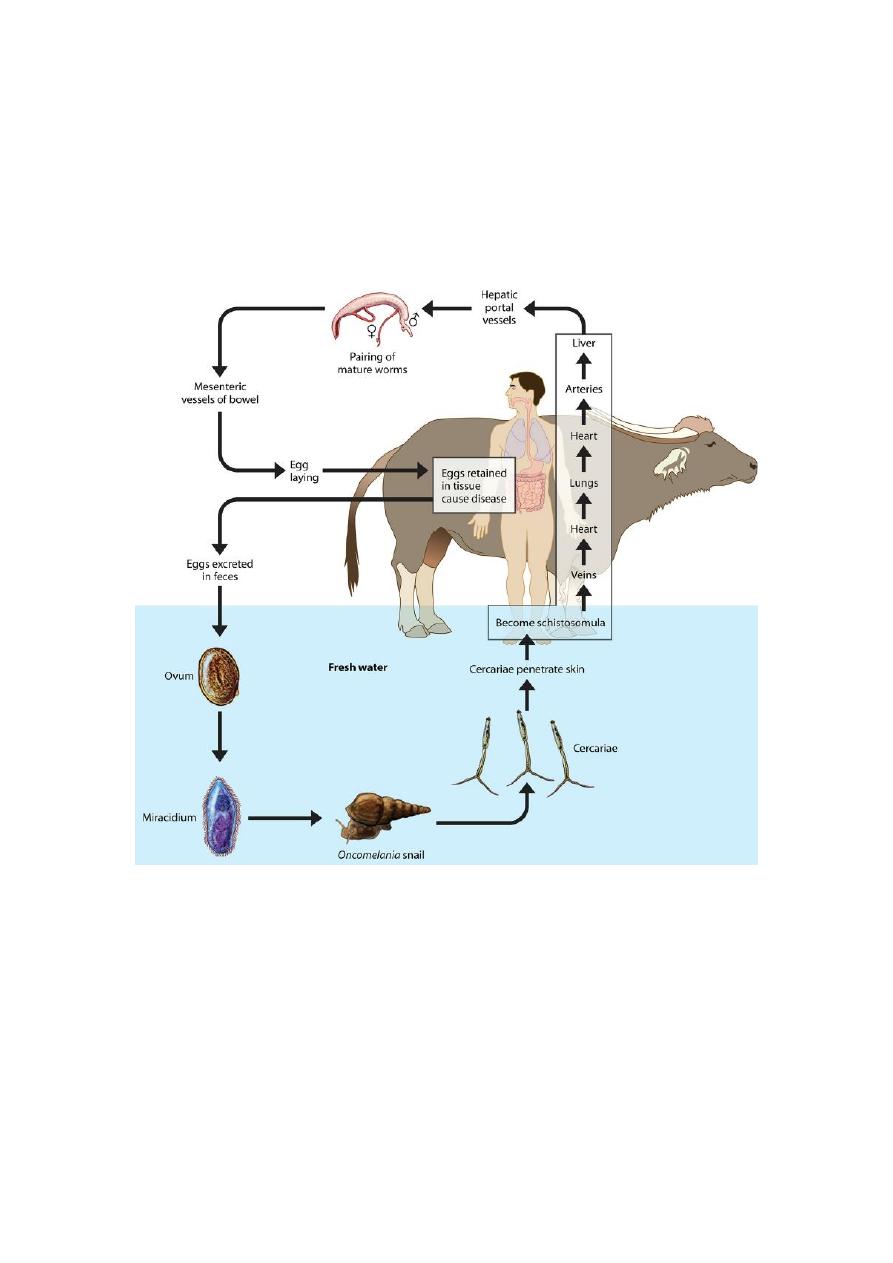
Life Cycle
Similar to S. haematobium
Pathogenesis and Clinical Features
Its pathogenesis is similar to that of S. mansoni, but because of its higher
egg output, the clinical manifestations are more severe, during the acute
phase. Katayama fever is similar to that seen in S. mansoni. Intestinal
manifestations are colicky abdominal pain and dysentery. Patient may
also develop anaemia. There is hepatomegaly with periportal fibrosis and
portal hypertension.
Diagnosis
Similar to that of S. mansoni
Treatment
Praziquantel (60 mg/kg/day orally in 3 divided doses for 1 day) is the
drug of choice.
Prevention and Control
Similar to that of S. haematobium
Schistosomal Dermatitis
Schistosomes of birds and semiaquatic mammals produce cercariae
that are capable of penetrating human skin but cannot develop into adults.
Humans may present with dermatitis which is frequently more severe
than the dermatitis produced by human schistosomes
.
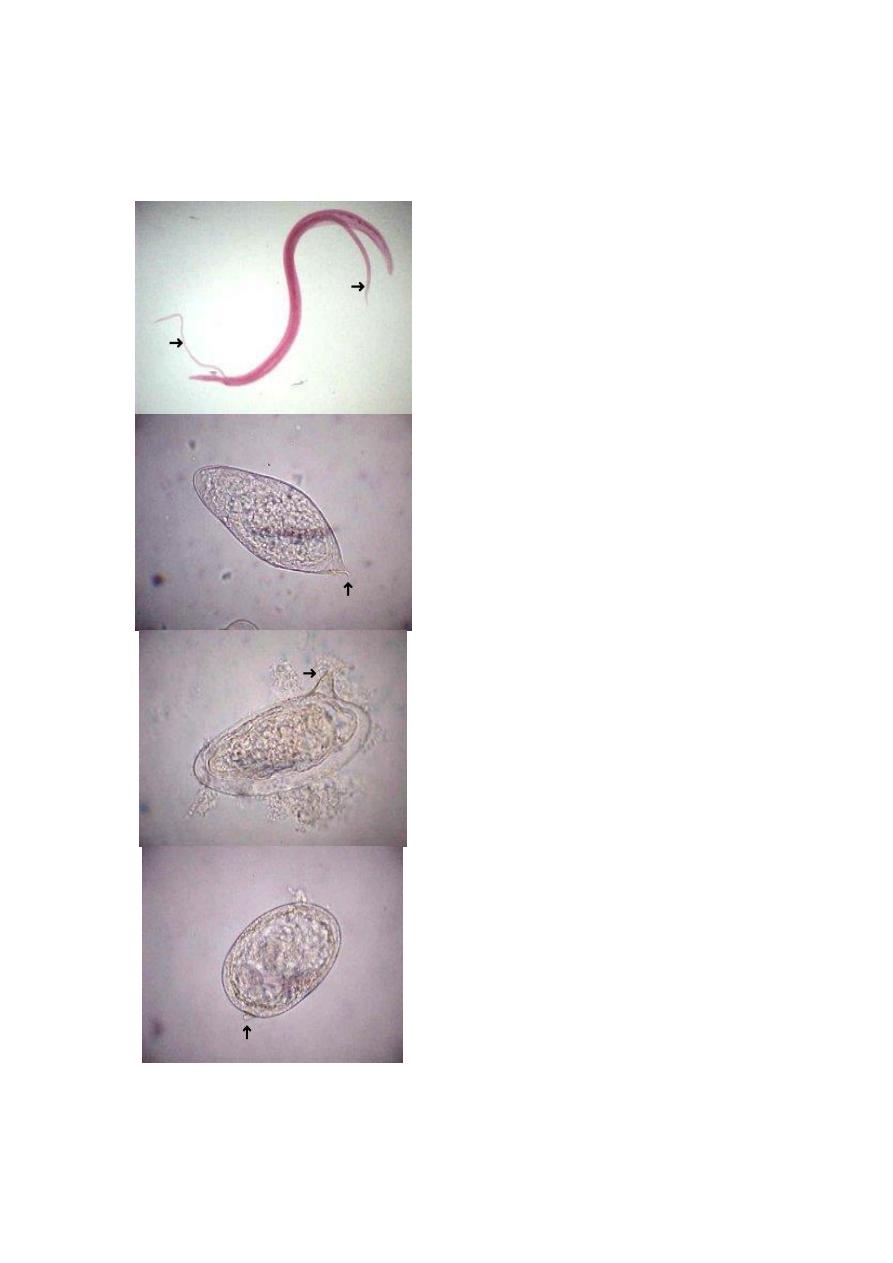
Adult Male & Female: The female worm
(arrows) resides in the gynecophoral
groove of the male. Note the long, narrow
shape, ideal for living in veins. They are
approximately 8 mm in length.
Egg: Schistosoma haematobium eggs are
passed in the urine and have a prominent
terminal spine (arrow). They measure
approximately 150 um in length.
Egg: Schistosoma mansoni eggs are
passed in the feces and have a large,
lateral spine (arrow). They measure
approximately 150 um in length.
Egg: Schistosoma japonicum eggs are
passed in the feces and have a vestigial,
nubby lateral spine (arrow). They are also
more rounded than the other 2 species and
measure approximately 100 um in length.
Differences between schistosomes
feature
S.haematobium S.mansoni
S.japonicum
egg
Terminal spine
Lateral spine
Lateral knob
Definitive
host
man
man
Man and domestic
animal
Intermediate
host
Bulinus
biomphalaria
Oncomelania
ovary
Behind the
middle of the
body contain 20
-30 eggs
Anterior to the
middle of the
body contain 1-3
eggs
In the middle of the
body contain 50 or
more eggs
No. of egg
passed/day
300egg
350 egg
3000 egg
Testis
4-5 in group
8-9 in zigzag row 6-7 in single file
Location
vesical and pelvic
venous plexuses
Inferior
mesenteric vein
superior mesenteric
vein