
Trematodes lec. 3
د.اسماء زكي شيتاوي
Liver flukes
1. Fasciola hepatica
2. Clonorchis sinensis
3. Opisthorchis viverrini
The adults of these trematodes live in the biliary ducts and may be also
found in the gallbladder in heavy infections.
The, Clonorchis sinensis (the Chinese liver fluke) and Opisthorchis
viverrini (the Southeast Asian liver fluke), are elongated and narrow and
much smaller than Fasciola (the sheep liver fluke).
.
Fasciola hepatica
: sheep liver fluke
Disease: fascioliasis( in sheep: liver rot.)
Distribution It is worldwide in distribution, being found mainly in sheep-
rearing countries.
Morphology
The adult worm: It is one of the largest flukes in the world measuring 30
mm long and15 mm broad (Fasciola gigantica, though, is even bigger
and can reach up to 75 mm). Leaf-shaped fleshy fluke, It has a conical
projection anteriorly with powerful oral sucker and is rounded
posteriorly. The acetabulum is a larger sucker than the oral sucker and is
located at the anterior
.
It is a hermaphrodite.
F. hepatica is equipped with
so-called shoulders
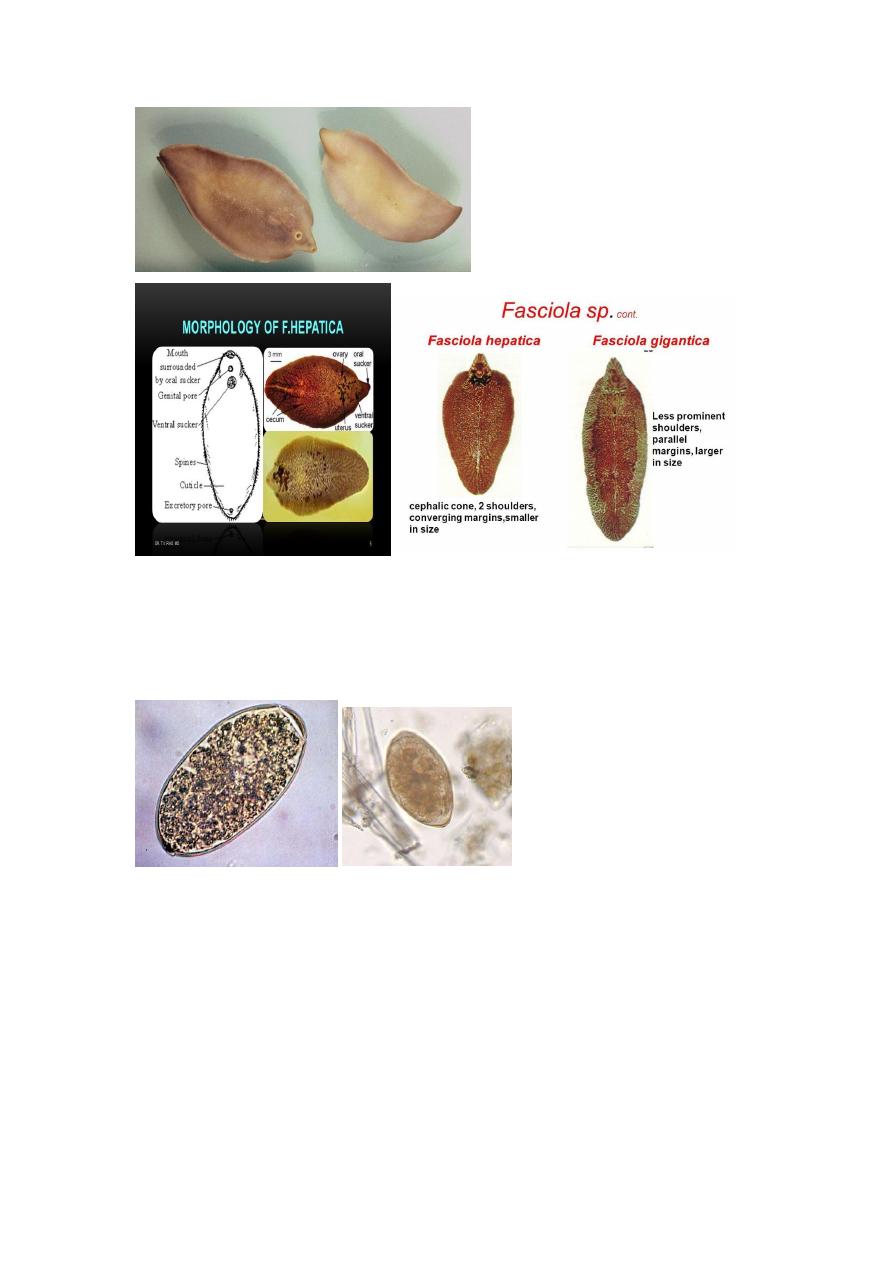
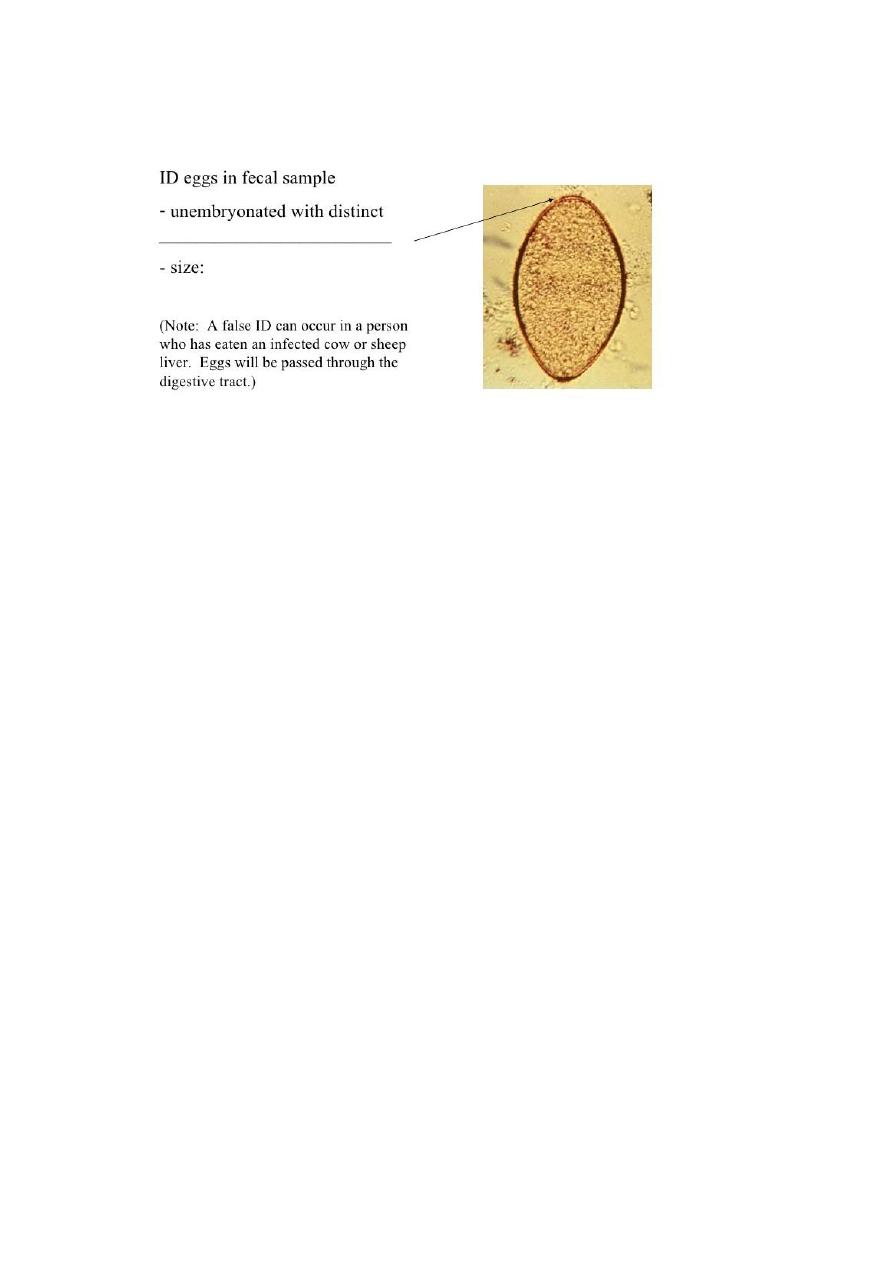
Egg: large, ovoid, operculated, bile stained, measuring 140 μm by 80
μm in size. When passed out it is unembroynated
Life cycle
Habitat The parasite resides in the liver and biliary passages of the
definitive host live up to 10 years in human.
Definitive host: Sheep, goat, cattle and man. Eggs are laid in the biliary
passages and are shed in feces.
1
st
intermediate host snail:
genus Lymnaea.
2
nd
intermediate host freshwater plants, especially watercress
Infective stage; metacercaria
Mode of infection: ingestion of metacercariae encysted on aquatic
vegetation.
F. hepatica passes its life cycle in one definitive host and two
intermediate hosts.
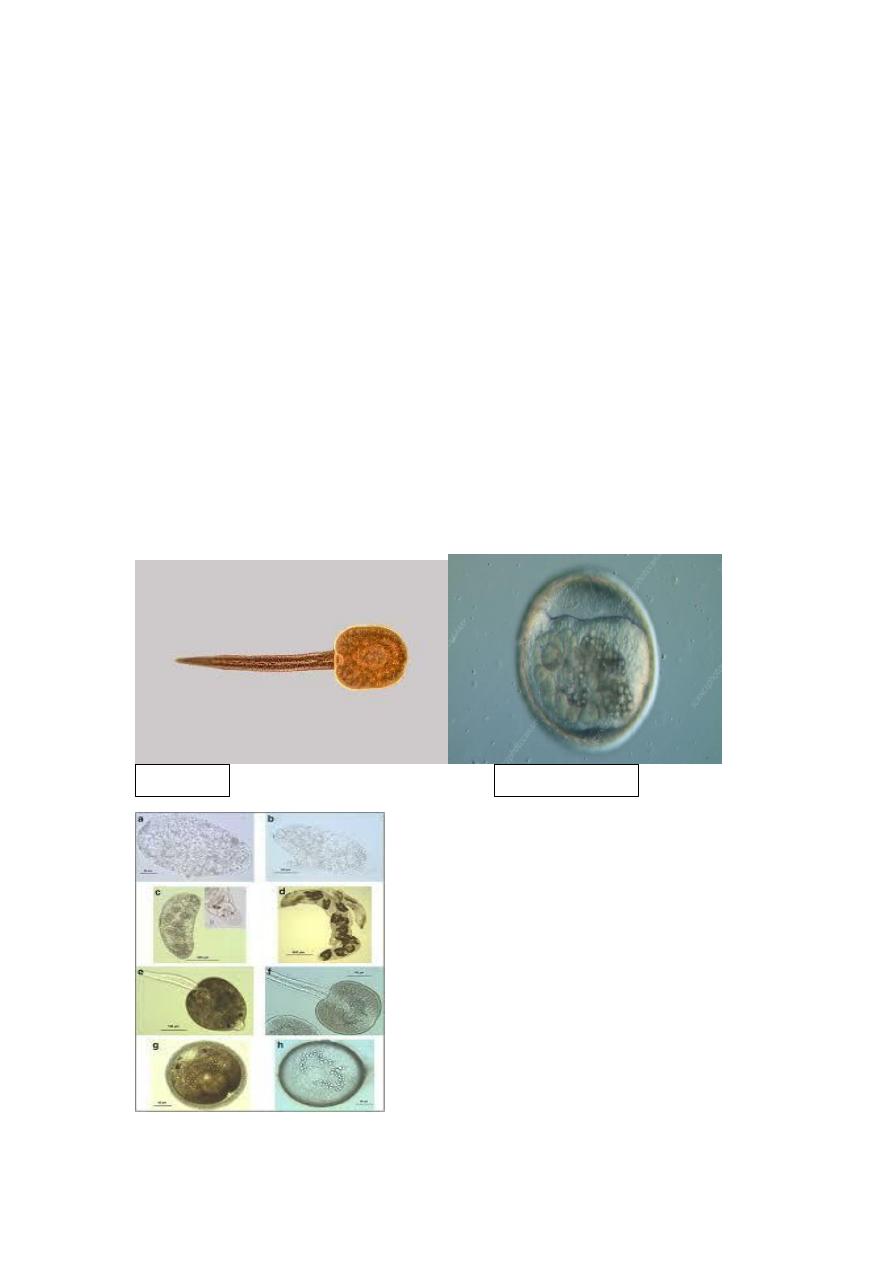
The embryo matures in water in about 10 days and the miracidium
escapes. It penetrates the tissues of first intermediate host, snails of the
genus Lymnaea
In snail, the miracidium progresses through the sporocyst and the first
and second generation redia stages to become the cercariae in about 1-2
months.
• The cercariae escape into the water and encyst on aquatic vegetation or
blades of grass to become metacercariae, which can survive for long
periods.
Cercaria
Metacercaria
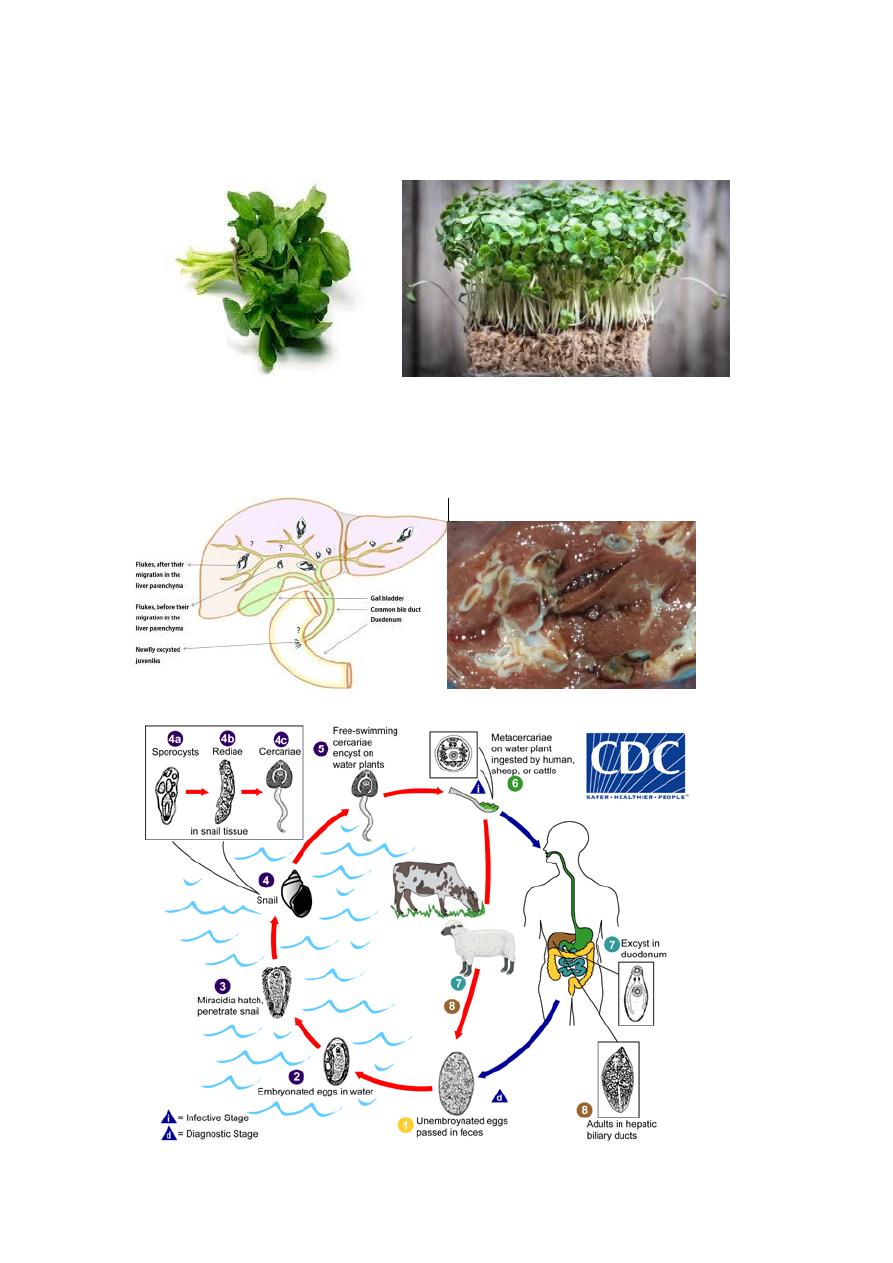
• Sheep, cattle, or humans eating watercress or other water vegetation
containing the metacercaria become infected.
The metacercariae excyst in the duodenum of the definitive host and
pierce the gut wall to enter the peritoneal cavity.
They penetrate to liver, reach the biliary passages and liver paranchyma ,
where they mature into the adult worms in about 3-4 months.
Pathogenesis and Clinical Features
F. hepatica is large causes more mechanical damage and parenchymal
injury.
As humans are not its primary host, it causes more severe inflammatory
response. Some larvae penetrate right through the liver and diaphragm
ending up in the lung.
• In acute phase during the migration of the larva, patients present with
fever, right upper quadrant pain, eosinophilia and tender hepatomegaly.
In chronic phase, patients may develop biliary obstruction, biliary
cirrhosis, obstructive jaundice, cholelithiasis and anemia. No association
to hepatic malignancy has been ascribed to fascioliasis.
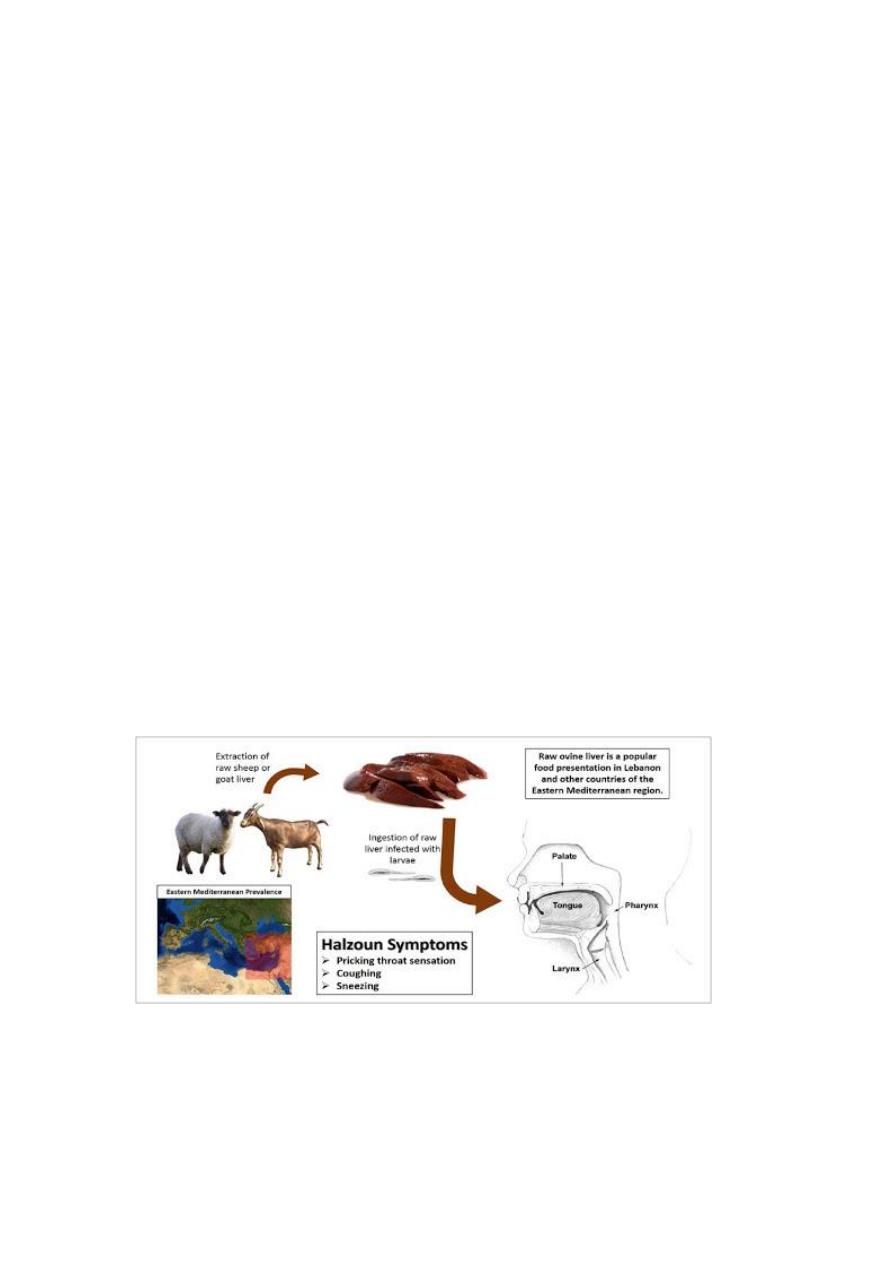
Occasionally, ingestion of raw liver of infected sheep results in a
condition called halzoun. The adult worms in the liver attach to the
pharyngeal mucosa, causing edematous congestion of the pharynx and
surrounding areas, leading to dyspnea, acute dysphagia, deafness and
rarely, asphyxiation. Halzoun is particularly common in Lebanon and
other parts of the Middle East and North Africa
.
False fascioliasis???
Laboratory diagnosis
1. Stool examination for the egg. Using a sedimentation method and a
wet mount with or without iodine staining. More than one
specimen may need to be examined to find the parasite. Sometimes
eggs are found by examining duodenal contents or bile. Infected
people don’t start passing eggs until they have been infected for
several months; people don’t pass eggs during the acute phase of
the infection.
2. Serology
Enzyme immunoassay (EIA) and ELISA to detected serum IgG
antibody cross reactivity with other trematodes, such as the
schistosomes, may be an issue.
The role of serology is important in
A. the acute phase of infection, before the onset of egg
production;

B. the chronic phase, in cases with low-level or sporadic
production of eggs
C. In cases of ectopic infection, in which eggs are not found in
stool
Treatment
The drug of choice for the treatment of Fasciola spp. is triclabendazole
(praziquantel is not effective). It is given in single oral dose of 10 mg/kg.
Bithionol is an alternative drug.
Prevention and Control
1. Prevent pollution of water courses with sheep and cattle faeces
2. Proper sanitation
3. Wash watercresses and other water vegetations, preferably in hot water
or cook well before consumption.
Clonorchis sinensis (the Chinese liver fluke),
Opisthorchis viverrini (the SoutheastAsian liver fluke)
Clonorchis sinensis
Disease clonorchiasis
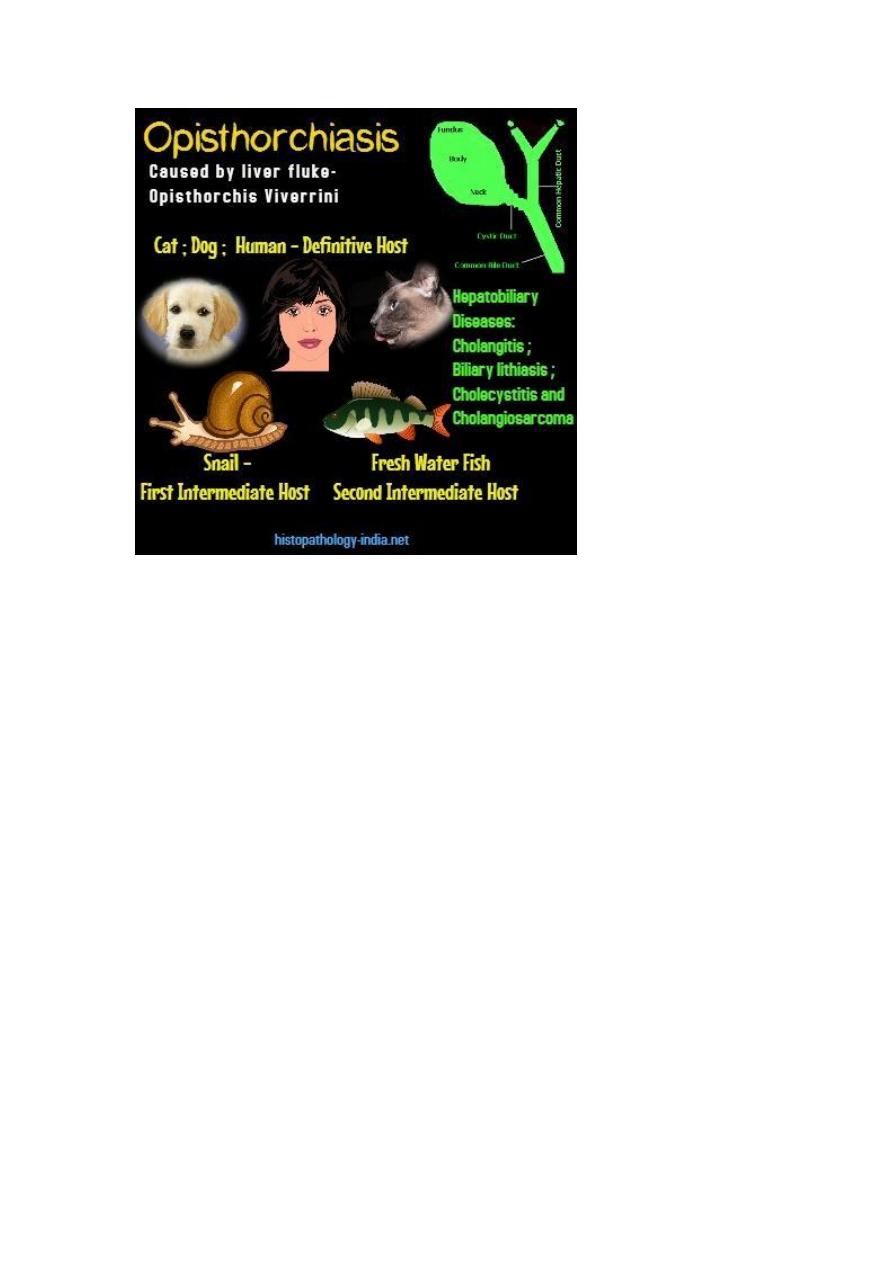
Opisthorchis viverrini
Disease opisthorchiasis
distribution occurs in Japan, Korea, Taiwan, China and Vietnam.
Opisthorchis viverrini is common in Thailand
Morphology (both worms have almost the same feature)
The adult worm has a flat, transparent, spatulate body; pointed anteriorly
and rounded posteriorly .It is 10–25 mm long and 3–5 mm broad. Each
end of the adult worm is narrower than the mid portion of the body. The
adult worm can survive many years in the biliary tract. The worm is
hermaphrodite and passes eggs into the bile duct. The testis of the adult
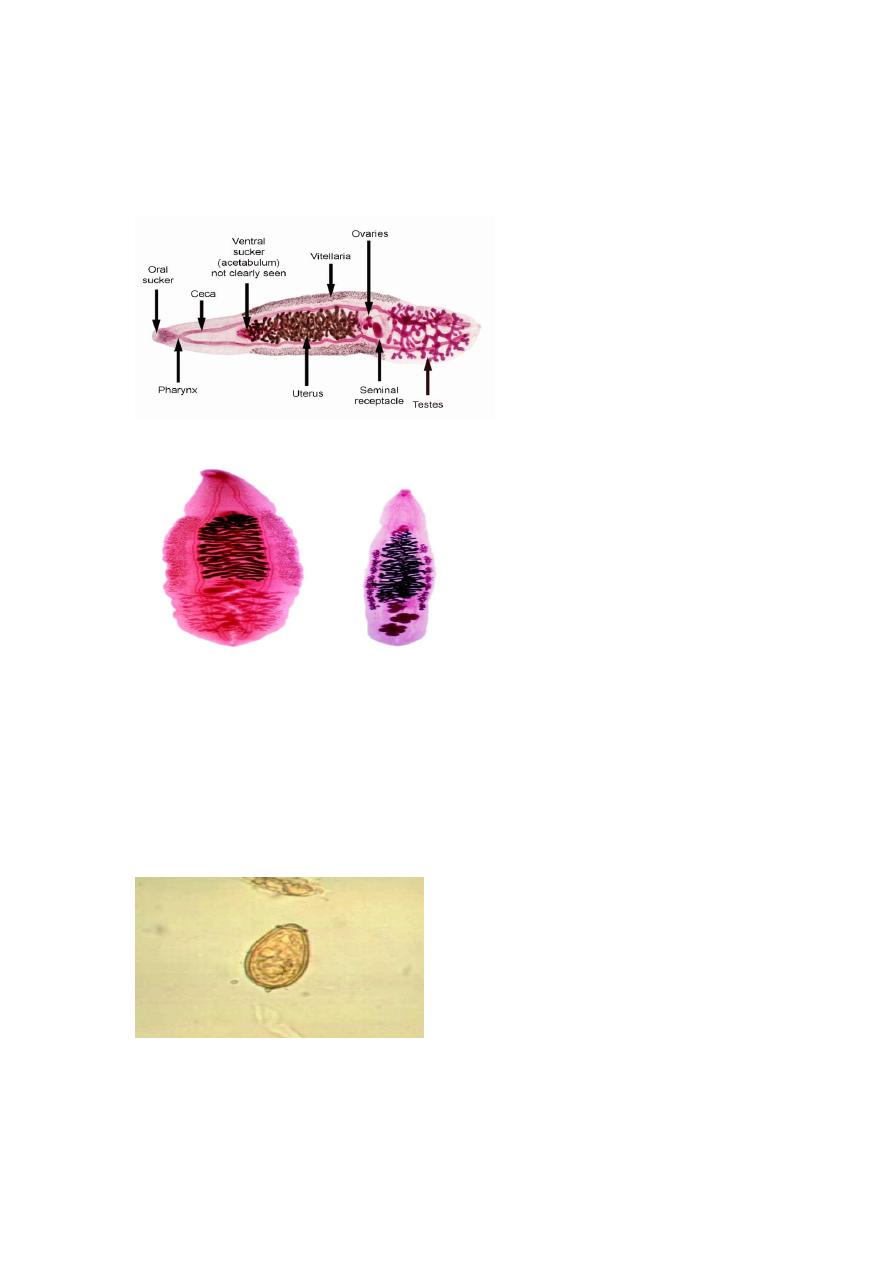
worm are branched in Clonorchis sinensis and lobe shape in
Opisthorchis viverrini.
Morphology of eggs: are broadly ovoid, 30 μm by 15 μm with a
yellowish brown (bile-stained) shell. It is jug shaped and operculated with
characteristic shoulders at the terminal end of the egg, a small knob is
sometimes visible. A thick rim is located around the operculum and is
referred to as shoulders
.
The eggs passed in faeces contain ciliated
miracidia .

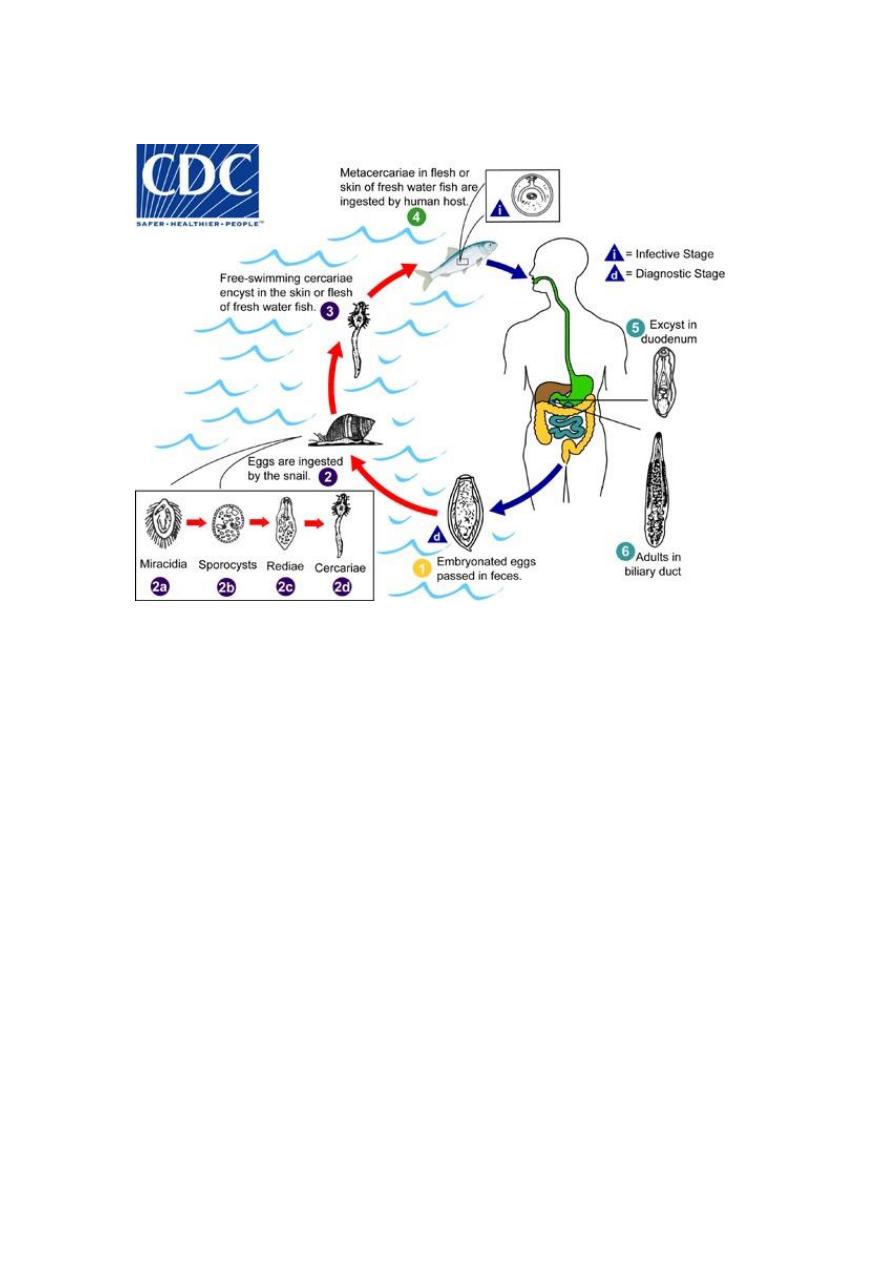
Life cycle
Habitat
Adult worm lives in the biliary tract.
Definitive host: human and carnivorous animals
Definitive host: Humans are the principal definitive host, but dogs and
other fish -eating canines act as reservoir hosts.
Intermediate hosts: Two intermediate hosts
1
st
intermediate host :
snail
genus Bulimus
2
nd
intermediate host: fresh water fish
Infective form: Metacercaria larva.
Mode of infection: Man acquires infection by eating undercooked
freshwater fish carrying metacercariae larvae.
Clonorchis eggs although embryonated do not hatch in water, but only
when ingested by suitable species of snails .The miracidium develops
through the sporocyst and redia stages to become cercaria .The cercariae
escape from the snail and swim about in water, waiting to get attached to
the second intermediate host, suitable freshwater fish. The cercariae shed
their tails and encyst under the scales or in the flesh of the fish to become
metacercariae, which are the infective stage for humans
.
Infection occurs when such fish are eaten raw or inadequately processed
by human or other definitive hosts. The metacercariae excyst in the
duodenum of the definitive host travel in the body enter the common bile
duct through the ampulla of Vater and proceed to the distal bile
capillaries, where they mature in about a month and assume the adult
form
• Adult worms produce eggs, which exit the bile ducts and are excreted in
the feces.
The cycle is then repeated
Pathogenesis and clinical features:
The migration of the larva up the bile duct induces desquamation,
followed by hyperplasia and sometimes adenomatous changes. The
smaller bile ducts undergo cystic dilatation. The adult worm may cause
obstruction and blockage of the common bile duct leading to cholangitis.
Chronic infection may result in calculus formation.
1. Light infections with C. sinensis or O. viverrini are most common
and may be asymptomatic.
2. Heavier infections with these flukes may present with fever,
abdominal pain, and jaundice. Eosinophilia and increased serum
levels of IgE may occur. Severe infections may cause obstruction
of the biliary ducts, resulting in enlargement and tenderness of the
liver, cirrhosis, cholecystitis and cholangiocarcinoma.
Laboratory diagnosis
1. Identification of the liver flukes is primarily made by recovery of
the eggs in feaces using a sedimentation method and a wet mount
with or without iodine staining.
2. Serology
Enzyme immunoassay (EIA) and ELISA to detected serum IgG
antibody cross reactivity with other trematodes, such as the
schistosomes, may be an issue.
Treatment
The drug of choice for treatment of infections with Clonorchis and
Opisthorchis is praziquantel (25 mg/kg) given orally three times per day
for 2 days.

Prevention and Control
Prevention and control measures for halting the spread of C. sinensis
include practicing proper sanitation procedures, especially in regard to
fecal disposal by the human and reservoir host (dogs and cats) and
avoiding the ingestion of raw, undercooked, or freshly pickled freshwater
fish and shrimp.