Medicine
Notes…
1
Lecture.4 Chest pain
Importance of Chest pain
Chest pain is a common challenge for clinicians in the office or emergency
department.
The differential diagnosis is wide, includes conditions affecting organs throughout
the thorax and abdomen, with prognostic implications that vary from benign to life-
threatening.
Detailed history and thorough clinical examination and appropriate subsequent
investigative pathway is needed
Differential diagnosis of chest pain
Central chest pain
Cardiac
• Myocardial ischaemia (angina)
• Myocardial infarction
• Pericarditis
• Mitral valve prolapse
• Myocarditis
Aortic
• Aortic dissection
• Aortic aneurysm
Oesophageal
• Oesophagitis
• Oesophageal spasm
• Mallory–Weiss syndrome
• Oesophageal perforation
Pulmonary embolus
Mediastinal
• Malignancy
Anxiety/emotion
N
eed S
om
e H
el
p?
Medicine
Notes…
2
Peripheral chest pain
Lungs/pleura
• Pulmonary infarct
• Pneumonia
• Pneumothorax
• Malignancy
• Tuberculosis
• Connective tissue disorders
Musculoskeletal
• Osteoarthritis
• Rib fracture/injury
• Acute vertebral fracture
• Costochondritis
• Intercostal muscle injury
• Epidemic myalgia
Neurological
• Prolapsed intervertebral disc
• Herpes zoster
• Thoracic outlet syndrome
History Is The Key To The Diagnosis Of Etiology Of Chest Pain
Key features in chest pain history
Site and radiation of pain
Character of pain
Onset of pain
Associated features with pain
Relieving and provocating factors
Medicine
Notes…
3
Site and radiation of pain
❖ Myocardial ischemia pain located in the centre of the chest. It may radiate to the
neck, jaw, and arms.
❖ Myocarditis or pericarditis pain felt retrosternally, to the left of the sternum, or in
the left or right shoulder.
❖ Aortic dissection is typically central with radiation to the back.
❖ Central chest pain may also occur with mediastinal tumors or oesophageal disease
❖ Pain situated over the left anterior chest radiating lateraly may due to pleural or lung
disorders, musculoskeletal problems or anxiety. And mitral valve prolapse.
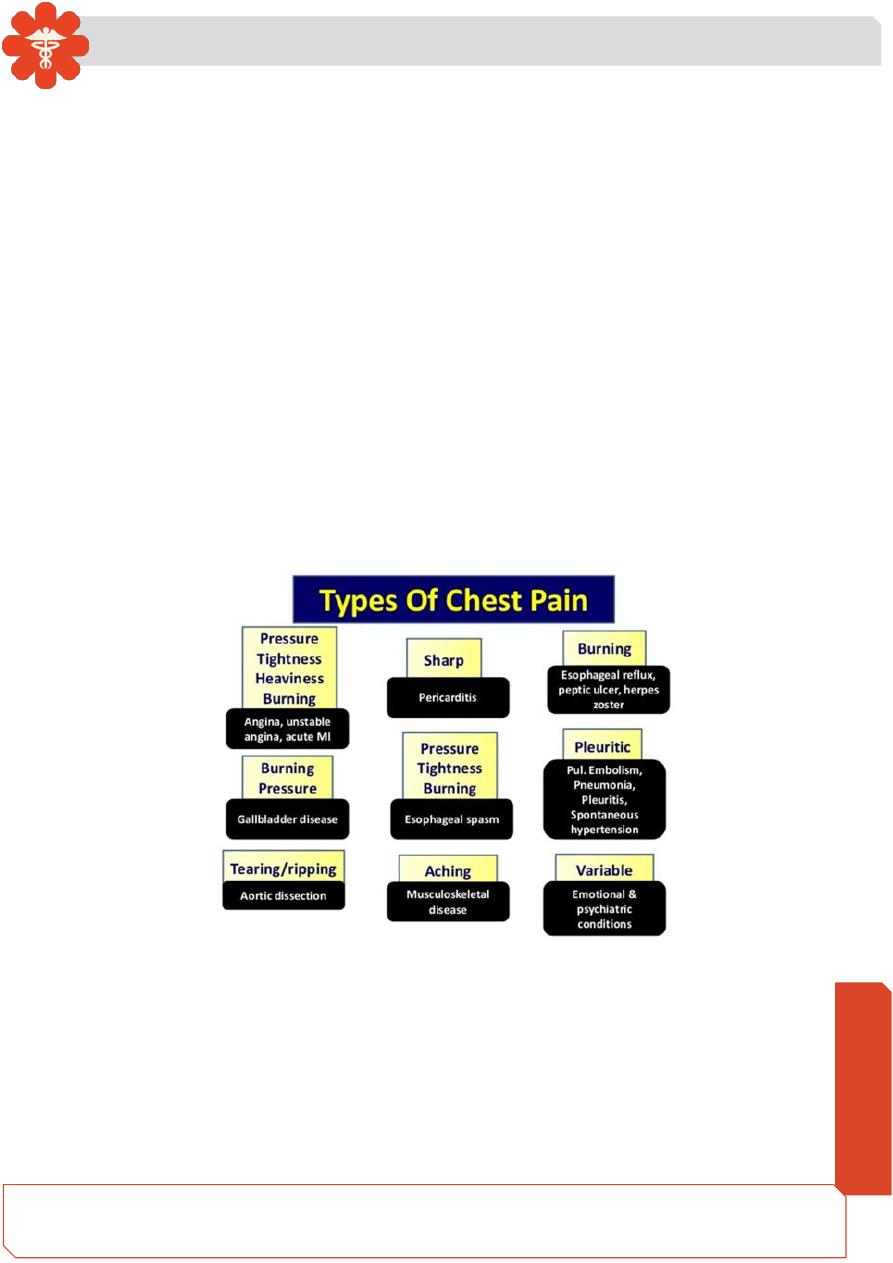
Character of pain
❖
The pain of myocardial ischaemia is dull, constricting, choking or ‘heavy’,
squeezing, crushing, burning or aching or even discomfort rather than a pain.
❖ Pleurisy, sharp chest pain aggravated by deep breathing or coughing
❖
Myocarditis or pericarditis ‘sharp’ and may ‘catch’ during inspiration, coughing,
swallowing or lying flat.
❖
The pain of aortic dissection is severe and ‘tearing’
Onset of pain
❖ The pain associated with myocardial infarction (MI) typically take several minutes
or longer to develop to its maximal intensity
❖ Angina builds up gradually in proportion to the intensity of exertion.
❖ Massive pulmonary embolism (PE) or pneumothorax is usually very sudden in
onset.
Medicine
Notes…
4
Relieving and provocating factors
❖ Angina occurs during exertion, relieved by rest and sublingual tablets, may occur
after a large meal or in a cold wind.
❖ Crescendo or unstable angina, similar pain may be precipitated by minimal
exertion or at rest.
❖ Decubitus angina induced by lying down
❖ Musculoskeletal The pain may vary with posture or movement of the upper body,
or be associated with a specific movement. Pain that occurs after, rather than
during, exertion is usually musculoskeletal or psychological in origin.
Associated features with pain
❖ Autonomic disturbance, including sweating, nausea and vomiting. impending death
usually accompany pain of MI, massive PE or aortic dissection.
❖ Breathlessness accompany myocardial ischemia due to pulmonary congestion,
also accompany respiratory causes of chest pain and associated with cough or
wheeze
❖ prodromal viral illness described in myocarditis or pericarditis
❖ Oesophageal pain dysphagia may be present
❖ Anxiety-induced chest pain may be associated with Breathlessness, throat
tightness, and other evidence of emotional distress.
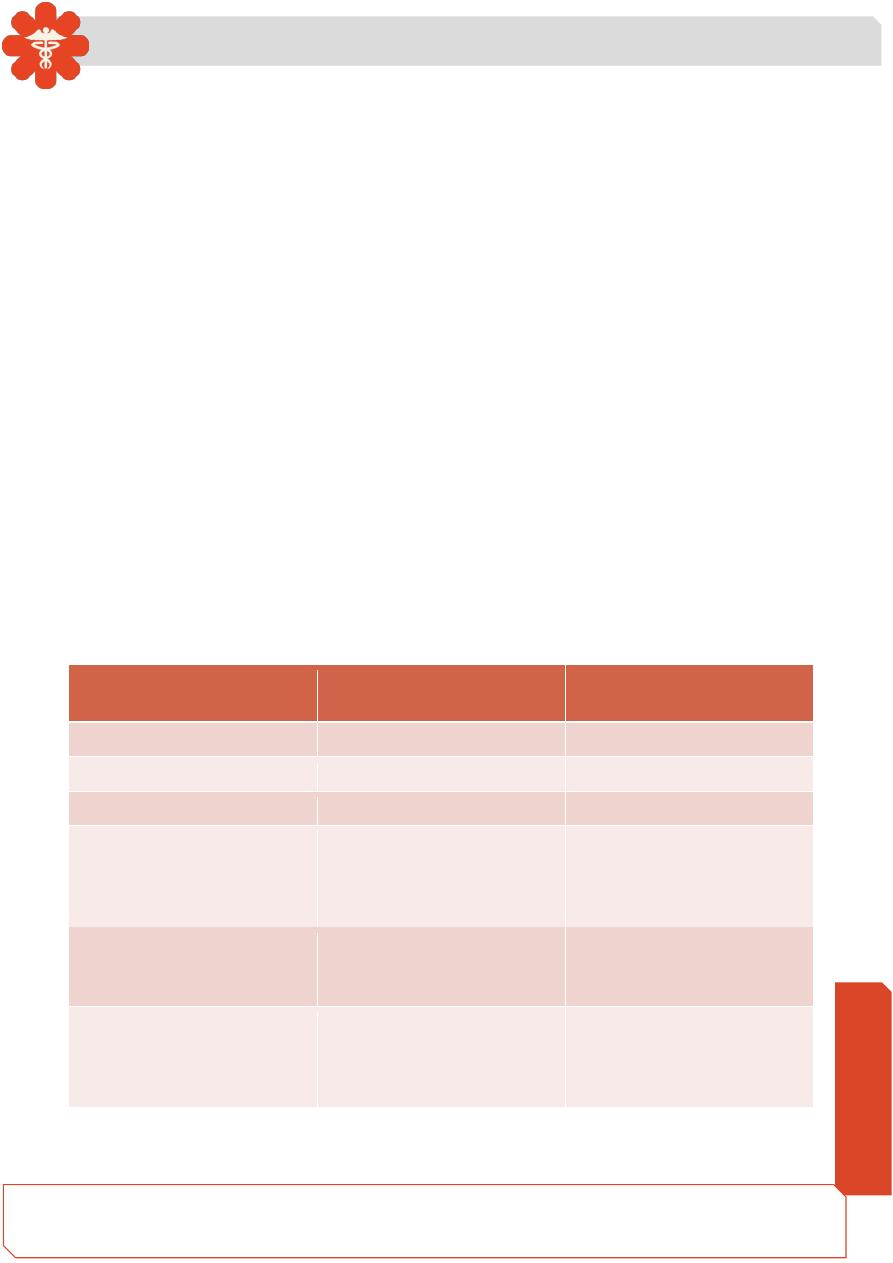
Ischemic
cardiac chest pain
Non-cardiac chest pain
LOCATION
Central, diffuse
Peripheral, localized
RADIATION
jaw/neck/shoulder/arm
Other or no radiation
CHARACTER
Tight, squeezing, choking
Sharp, stabbing, catching
PRECIPITATION
Precipitated by exertion
and/or emotion
Spontaneous, not related
to exertion,
provoked by posture,
respiration or palpation
RELEAVING FACTORS
Rest
response to nitrates
Not relieved by rest
Slow or no response to
nitrates
ASSOCIATED
FEATURES
Breathlessness
Respiratory,
gastrointestinal,
locomotor or
psychological
Medicine
Notes…
5
Characteristics of ischemic cardiac pain
Site: Cardiac pain is typically located in the center of the chest
Radiation: Ischemic cardiac pain may radiate to the neck, jaw, and upper or even
lower arms. Occasionally, cardiac pain may be experienced only at the sites of
radiation or in the back
Character: Cardiac pain is typically dull, constricting, choking or ‘heavy’, and is
usually described as squeezing, crushing, burning or aching. The sensation can be
described as breathlessness, or discomfort rather than a pain.
Provocation:
• Anginal pain occurs during exertion and is relieved by rest. The pain may also be
precipitated or exacerbated by emotion, after a large meal or in a cold wind.
• Unstable angina pain precipitated by minimal exertion or at rest.
• Decubitus angina induced by lying
• Myocardial infarction (MI) may be preceded by a period of stable or unstable angina
but often occurs de novo.
Examples of cardiac chest pain
Stable Angina
Effort-
related chest pain is the hallmark of angina pectoris or ‘choking in the chest. The
reproducibility, predictability and relationship to physical exertion (and occasionally
emotion) of the chest pain are the most important features. The duration of symptoms
should be noted.
Acute Coronary Syndromes
Prolonged, severe cardiac chest pain may be due to
1.Unstable angina
Medicine
Notes…
6
which comprises recent-onset limiting angina, rapidly worsening or crescendo angina,
and angina at rest)
2. Acute MI
Myocarditis and pericarditis
Pain is characteristically felt retrosternally, to the left of the sternum, or in the left or
right shoulder, and typically varies in intensity with movement and the phase of
respiration. The pain is described as ‘sharp’ and may ‘catch’ the patient during inspiration,
coughing or lying flat
Aortic dissection
This pain is severe, sharp and tearing, is often felt in or penetrating through to the
back, and is typically very abrupt in onset .The pain follows the path of the dissection.
Mitral valve prolapse
Sharp left-sided chest pain that is suggestive of a musculoskeletal problem may be a
feature of mitral valve prolapse
Examples of non-cardiac causes of chest pain
Oesophageal pain
This can mimic the pain of angina very closely, is sometimes precipitated by exercise
and may be relieved by nitrates. However, it is usually possible to elicit a history relating
chest pain to supine posture or eating, drinking or oesophageal reflux. It often radiates to
the interscapular region and dysphagia may be present
Musculoskeletal chest pain
This is a common problem that is very variable in site and intensity but does not usually
fall into any of the patterns described above. The pain may vary with posture or movement
of the upper body and is sometimes accompanied by local tenderness over a rib or costal
cartilage.
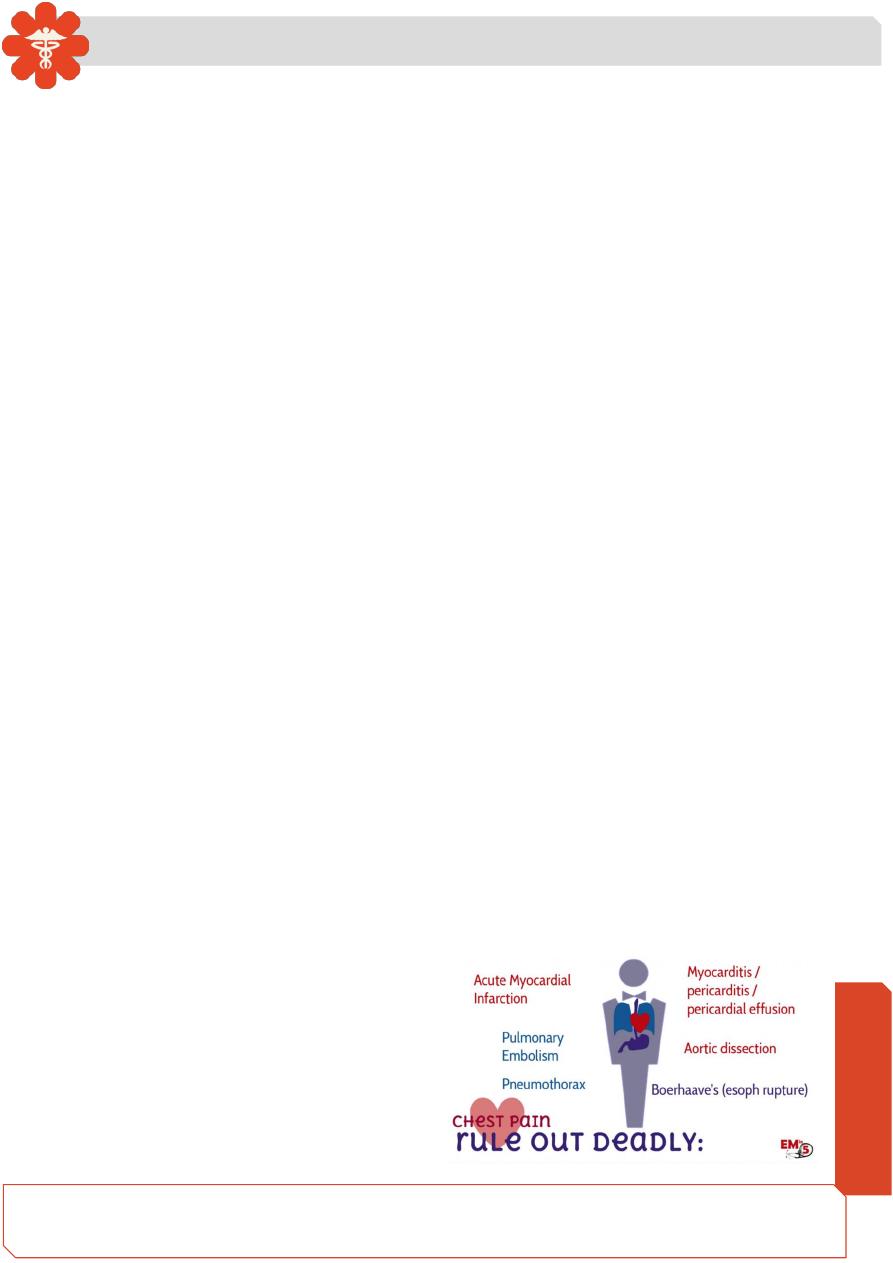
Life threatening causes of chest pain
• Acute coronary syndrome(MI, unstable angina)
• Aortic Dissection
• Pulmonary Embolism
• Tension pneumothorax
• Oesophageal rupture
Medicine
Notes…
7
Clinical signs in assessment of chest pain
Cardio -respiratory examination may detect clinical signs that help guide ongoing
investigation.
Vital signs
Clinical evidence of increased intracardiac pressure (especially a raised jugular
venous pressure) in myocardial ischemia or massive Pulmonary embolism (PE)
Evidence of deep vein thrombosis in PE
Signs of pneumothorax: absent breath sounds and a hyper-resonant percussion
note on the affected side.
❖ bronchial breathing or crackles, are most likely to indicate a respiratory tract
infection
❖ pericardial friction rub in pericarditis
❖
asymmetrical pulses, Marfan’s syndrome and new early diastolic murmur due to
aortic regurgitation in aortic dissection
❖ pleural rub may be audible in pleurisy
❖ Local tenderness of the chest wall in musculoskeletal pain
Initial investigations
Chest X-ray
ECG
Biomarkers (e.g. troponin, D-dimer)