Medicine
Notes…
1
Disorders of Potassium
Hypokalemia:
Hypokalaemia is a common electrolyte disturbance and is defined as existing when serum
potassium falls below 3.5 mmol/L.
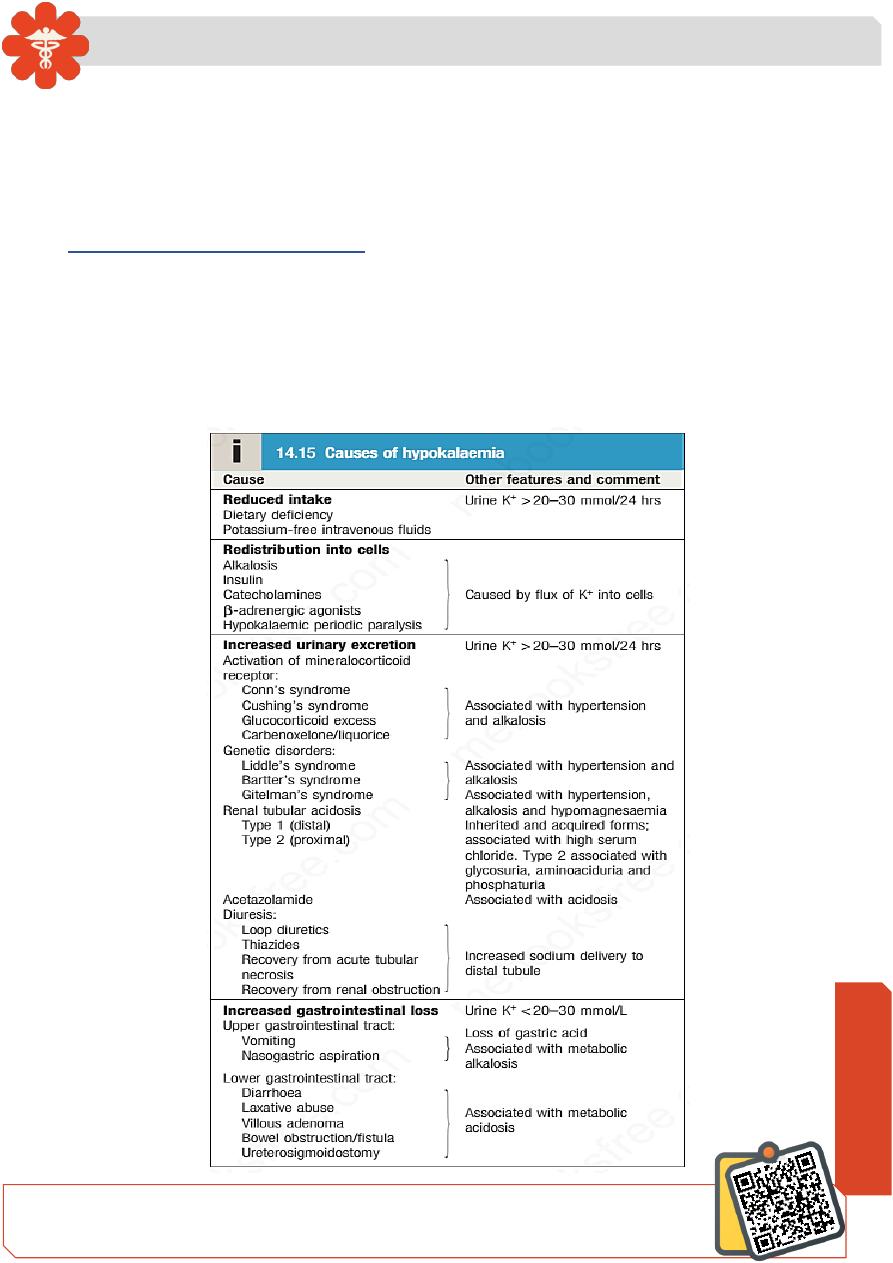
Causes of hypokalemia include:
1. Reduced intake: Dietary deficiency ,Potassium-free intravenous fluids
2. Redistribution into cells:Alkalosis,Insulin,Catecholamines,
β-adrenergic agonists,
Hypokalaemic periodic paralysis.
3. Increased urinary excretion: see box
4. Increased GIT loss: see box
N
eed S
om
e H
el
p?
Medicine
Notes…
2
Clinical features:
Patients with mild hypokalaemia (plasma K+3.0
–3.3 mmol/L) are generally
asymptomatic, but more profound reductions in plasma potassium often lead to muscular
weakness and associated tiredness. Ventricular ectopic beats or more serious
arrhythmias may occur and the arrhythmogenic effects of digoxin may be potentiated.
Typical electrocardiogram (ECG) changes occur, affecting the T wave in particular (
flattening or even inversion of T-wave).
Functional bowel obstruction may occur due to paralytic ileus. Long-standing
hypokalaemia may cause renal tubular damage (hypokalaemic nephropathy) and can
interfere with the tubular response to vasopressin (acquired nephrogenic diabetes
insipidus), resulting in polyuria and polydipsia.
Investigations:
Measurement of plasma electrolytes, bicarbonate, urine potassium and sometimes of
plasma calcium and magnesium is usually sufficient to establish the diagnosis.
Measurement of urinary potassium may be helpful; if the kidney is the route of
potassium loss, the urine potassium is high (> 30 mmol/24 hrs), whereas if potassium is
being lost through the gastrointestinal tract, the kidney retains potassium, resulting in a
lower urinary potassium (generally < 20 mmol/24 hrs).
Management:
Treatment of hypokalaemia involves first determining the cause and correcting this where
possible. If the problem is mainly one of redistribution of potassium into cells, reversal of
the process responsible may be sufficient to restore plasma potassium without providing
supplements. In most cases, however, some form of potassium replacement will be
required. This can generally be achieved with slow-release potassium chloride tablets,
but in more acute circumstances intravenous potassium chloride may be necessary.
The rate of administration depends on the severity of hypokalaemia and the presence
of cardiac or neuromuscular complications, but should generally not exceed 10 mmol of
potassium per hour. In patients with severe, life-threatening hypokalaemia, the
concentration of potassium in the infused fluid may be increased to 40 mmol/L if a
peripheral vein is used, but higher concentrations must be infused into a large ‘central’
vein with continuous cardiac monitoring.
In some circumstances, potassium-sparing diuretics, such as amiloride, can assist in
the correction of hypokalaemia, hypomagnesaemia and metabolic alkalosis, especially
when renal loss of potassium is the underlying cause.
Medicine
Notes…
3
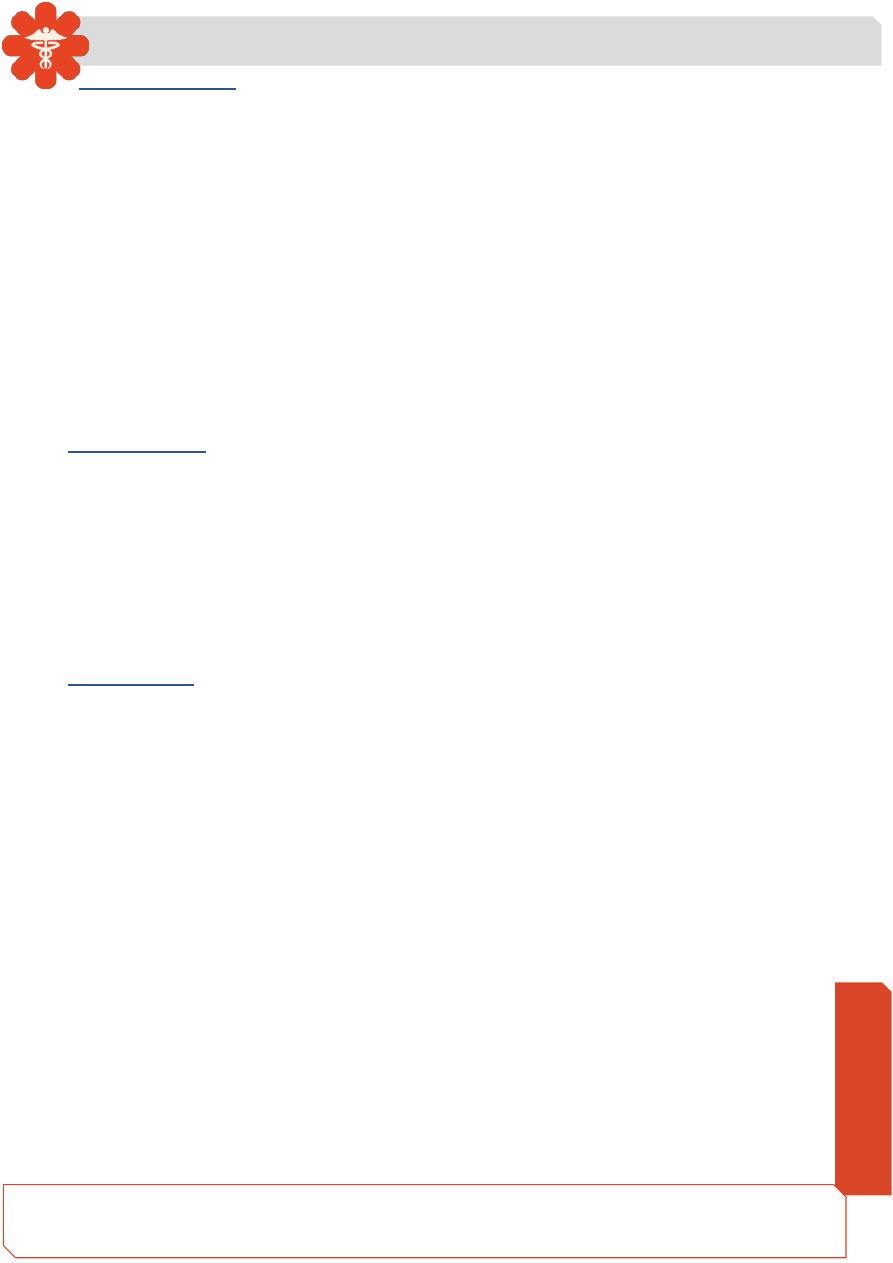
Hyperkaliemia:
Hyperkalaemia is a common electrolyte disorder, which is defined as existing
when serum K+ is > 5 mmol/L.
Clinical features:
Mild to moderate hyperkalaemia (< 6.5 mmol/L) is usually asymptomatic. More
severe hyperkalaemia can present with progressive muscular weakness, but sometimes
there are no symptoms until cardiac arrest occurs. Peaking of the T wave is an early ECG
sign, but widening of the QRS complex presages a dangerous cardiac arrhythmia.
However, these characteristic ECG findings are not always present, even in severe
hyperkalaemia.
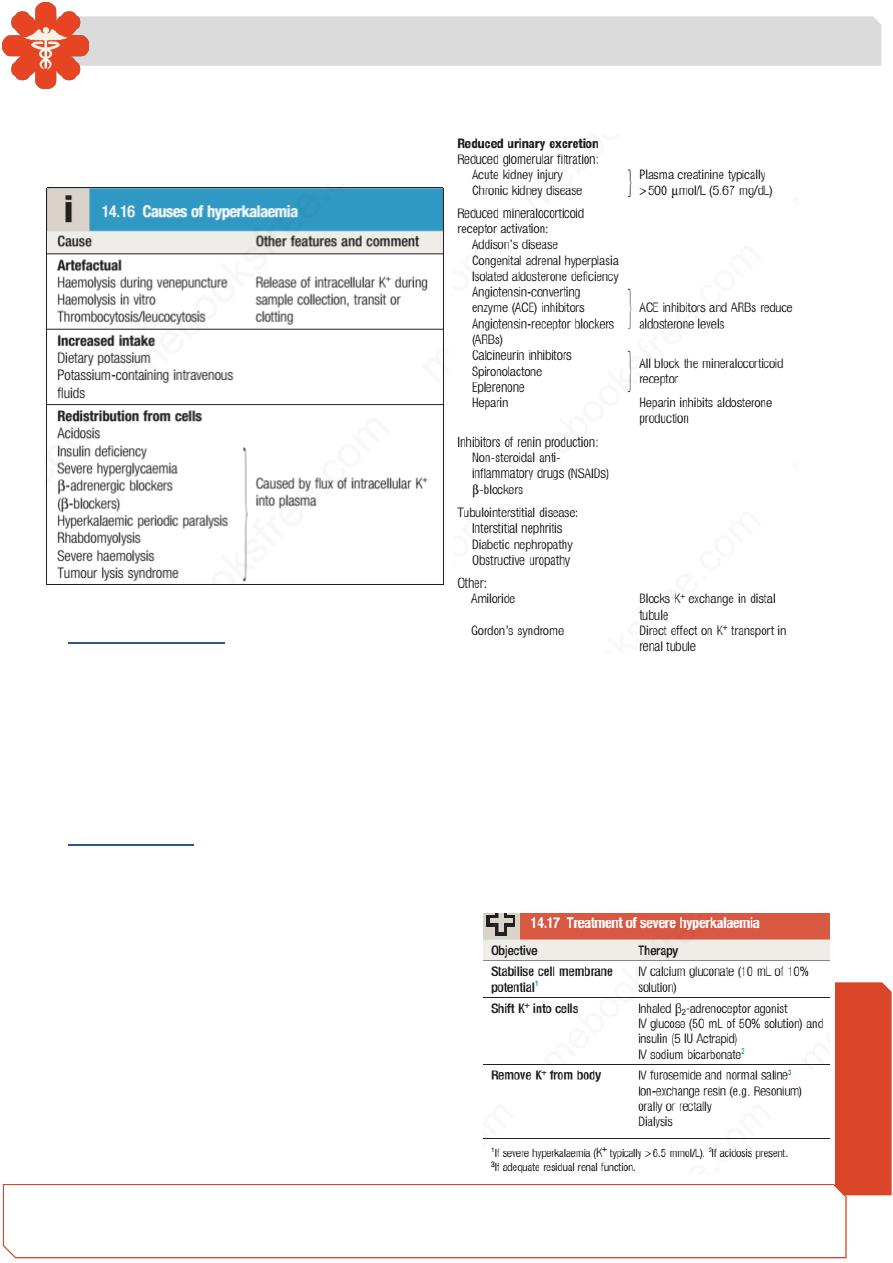
Management:
Treatment of hyperkalaemia depends on its severity and the rate of development, but
opinions vary as to what level of serum potassium constitutes severe hyperkalaemia and
requires urgent treatment. Patients who have
potassium concentrations < 6.5 mmol/L in the
absence of neuromuscular symptoms or ECG
changes can be treated with a reduction of
potassium
intake
and
correction
of
predisposing factors. However, in acute and/ or
severe hyperkalaemia (plasma potassium >
6.5
–7.0 mmol/L), more urgent measures must
be taken.