Growth and development
Mazin Al-Jadiry5 October 2015
Human Development
Specific Objectives:By the end of this lecture, the student will be able to:
Define growth and development
Identify the importance of growth and development
Mention the principles of growth and development
List factors affecting growth and development
Growth
Growth refers to an increase in physical size of the whole body or any of its parts.It is simply a quantitative change in the child’s body.
It can be measured in Kg, pounds, meters, inches, ….. etc
Growth: generally refers to changes in size
Development
Development refers to a progressive increase in skill and capacity of function.It is a qualitative change in the child’s functioning.
It can be measured through observation.Development:Occurs through maturation of physical & mental capacities & learning
Stages of Growth & DevelopmentPrenatal
- Embryonic (conception- 8 w)
- Fetal stage (8-40 or 42 w)
Infancy
Neonate: Birth to end of 1 month
Infancy: 1 month to end of 1 year
Early Childhood
Toddler: 1-3 years
Preschool: 3-6 years
Middle Childhood
School age: 6 to 12 years
Late Childhood
Adolescent: 13 years to approximately 18 yearsGrowing up
“Growing up” involves three major dynamic processes:Growth
Development
Sexual Maturation
Physical Growth
Increase in the size of the body as a whole or the increase in its separate parts.Growth milestones are the most predictable.
It is essential to plot the child’s growth on gender and age appropriate charts
Physical Growth
The growth of a child occurs in four phases—Fetal
Infantile
Juvenile & Adolescent
Fetal Growth
Prenatally, the growth of the head predominates, reaching the peak in the third trimester.The size of an infant at birth is affected:
Primarily by maternal size
Secondarily by other Intra uterine factors such as
Maternal nutrition,
Use of tobacco and alcohol,
Placental adequacy,
Intrauterine infection and
Gestational age at birth.
Infantile Growth
During the first 12–24 months after birth, the time of greatest postnatal growth velocity, the infant “seeks his or her own curve.” That is, by age 2–3 years, the child's stature reflects his or her own genetic endowment rather than mother's size and health.Infancy is a period of rapid but decelerating growth; the average of infant's birth weight doubles within 5 mo, but is only triple at 1 yr.
Infantile Growth
Length follow a similar but less dramatic growth curve, it increases by 30% at 5 mo, the growth rate slowly decreases so that the length is only 50% above birth length at 1 yr.Growth of the brain occurs almost exclusively during the early years of life. At birth, it is 25% of adult size and at 1yr, 75%. Full development is not achieved until adolescence.
Juvenile and adolescent Growth
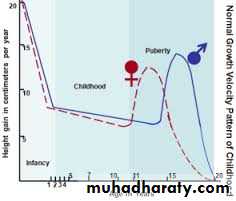
Growth during the remainder of childhood occurs at a rate of 5–6 cm per year, along the percentile band achieved by 2–3 years.
Adolescence is characterized by an abrupt, short-lived increase in growth velocity (the “growth spurt”), mediated by gonadal & growth hormones.
Adult height may to some degree be predictable by the mid-parental height (maternal height plus paternal height, divided by two).
Developmental Milestones
A skill that a child acquires within a specific time frame.4 fields with a sequence of development:
• Gross Motor - the development of locomotion (Latin locō, from a place, place + motion).• Vision and fine manipulation - the development of eye-hand control
• Hearing & speech - the development of language
• Personal & social - integration of acquired abilities to reflect understanding of environment.
Developmental Milestones Principles
• Development progresses from generalized reflexes to stimuli to voluntary discrete actions that are asymmetric and precise toward stimuli (eg, grasping with one hand and examining with the other).• Developmental control progresses from cephalic to caudal and from proximal to distal.
• Development is continuous and lifelong, but most dramatic early in life
• Developmental outcome is product of active interplay between individual’s genetic make-up and unique environmental influences (nature vs nurture)
Developmental Milestones Principles
Physical features of the baby can be identified as identical to that of parents, like eyes from father & the hair color from mother-----Nature
However, personality and talents may have come not from parents. The environment where a child grew up may have a lasting effect or influence on that way the child talk, behave and respond to the things around----Nurture
Sexual Maturation
• Differentiation of the bipotential fetal gonad and development along either male or female phenotype;• Maturation (puberty) with the attainment of secondary sexual characteristics and the capacity for fertility; and
• The psychological concept of sexuality.
Physical Development
Body size, body proportions, appearance, brain development, motor development, physical health.
Cognitive Development
Thought processes and intellectual abilities including attention, memory, problem solving, imagination, creativity, academic and everyday knowledge, and language.
Social/Emotional Development
• self-knowledge (self-esteem, sexual identity, ethnic identity), moral reasoning, understanding and expression of emotions, self-regulation, temperament, understanding others, interpersonal skills, and friendships.
Primary primitive reflexes
Reflexes: Involuntary, physical responses to stimuliMaintain adequate supply of oxygen (hiccup, sneeze, spit-up)
Maintain constant body temperature (cry, shiver, tuck legs)
Ensure adequate nourishment (sucking, rooting, swallowing)
One month-Reflexes
Primary Primitive reflexes
Rooting reflex; when gently touched on the cheek, the baby's head turns as if in search of the nipple
Swallowing and sucking reflexes: when anything is put in the mouth, the baby immediately sucks and swallows
normal root abn. Root
Primary Primitive reflexes
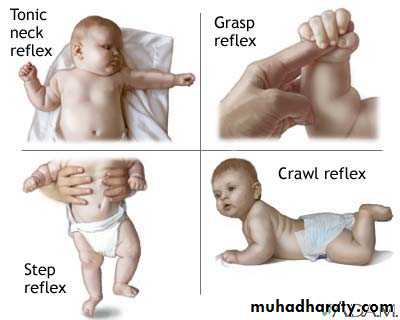
The grasp response is elicited by placing a finger or object in the open palm of each hand. Normal infants grasp the object, and with attempted removal, the grip is reinforced.Walking (stepping) reflex: when held upright with the feet touching a firm surface, the baby will make walking movements.
Grasp response, normal stepping, abn. stepping
Primary Primitive reflexes
Moro reflex : any sudden movement which cause head extension (gives the baby the feeling that he may be dropped) causes extension following by flexion of the arms and legs.An asymmetric response may signify a fractured clavicle, brachial plexus injury, or a hemiparesis on the side of the poorly abducted arm).
Absence response in a term newborn is ominous, suggesting significant dysfunction of the CNS. Abn.
moro in 6mo
Primary Primitive reflexes
The Galant reflex (trunk incurvation) is obtained by placing the baby in ventral suspension, then stroking the skin on one side of the back. The baby’s trunk and hips should swing towards the side of the stimulus. this reflex is absent in transverse spinal cord lesions or injuries.Primary Primitive reflexes
The tonic neck reflex is produced by manually turning the head to one side while supine. Extension of the arm occurs on that side of the body corresponding to the direction of the face, while flexion develops in the contralateral extremities.An obligatory tonic neck response, by which the infant remains “locked” in the fencer's position, is always abnormal and implies a CNS disorder.
Secondary (Postural) reflexes
Become apparent after the newborn period, indicating proper maturation of appropriate brain structures, the development of postural reflexes is essential for independent sitting and walking.
Lateral propping occurs when the baby is falling to one side or the other and he extends the arm laterally to catch himself.
it appears at age of 6-8 months, fully developed at age of 10-11 month and never disappear
Asymmetric lateral propping can be an early sign of hemiparesis, the baby will prop on one side but on the paretic side he will not extend the arm to catch himself with the infant sitting
Secondary (Postural) reflexes
Parachute reflex is the last of the postural reflexes to develop. It usually appears at 8 to 9 months of age. demonstrated by suspending the child by the trunk and by suddenly producing forward flexion as if the child were to fall. The child spontaneously extends the upper extremities as a protective mechanism. Asymmetry of the reflex is abnormal and may indicate paresis in the non-extended extremity. No parachute in 6 moAlthough many primitive reflexes have been described, the Moro, grasp, tonic neck, and parachute reflexes are the most important.
Reflexes and Responses
• Primitive reflexes• Appearance
• Disappearance
• Sucking
• Birth
• Persist
• Stepping, placing
• Birth
• 1-2 mo
• Rooting
• Birth
• 3-4 mo
• Palmar grasp
• Birth
• 3-5 mo
• Moro reflex
• Birth
• 4-6 mo
• Asymmetric tonic neck
• Birth to 2 wk
• 6-7 mo
• Plantar grasp
• Birth
• 9-12 mo
• Galant (trunk incurvation)
• Birth
• 9-12 mo
Reflexes and Responses
• Postural responses
• Appearance
• Disappearance
• Lateral propping
• 6-8 mo
• Remain throughout life
• Forward parachute
• 8-9 mo
• Remain throughout life
Clinical Pearl
A delay in achieving milestones does not always indicate an abnormality, most late talkers and walkers turn out to be normal. Likewise, achieving a milestone at a given time does not always indicate normalcy. E.g. a child with cerebral palsy or Down syndrome may meet early milestones on schedule.Developmental testing is not a substitute for the physical examination.
Testing is merely an adjunct to aid in forming a complete picture about the patient.
Social smiles
Hold head erects in mid-position.
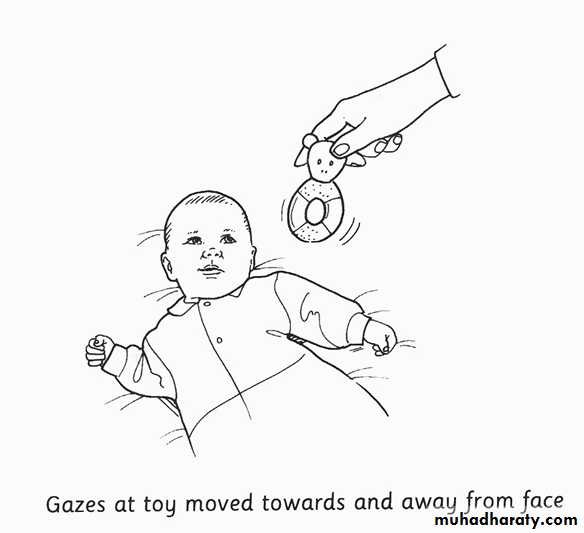
Fixes & follows
At 3 months;