18th Oct. 2015 5th year medical college Al-Mustansiriya University. First psychology lecture. Dr. Sami Adil
18th Oct. 2015 5th year medical college Al-Mustansiriya University. First psychology lecture. Dr. Sami Adil
5. Stress and Attachment
Stress refers to experiencing events that are perceived as endangering one's physical or psychological wellbeing. The cause of stress can be from outside of us (traumatic events: war, killing, sexual abuse, verbal abuse, etc..) or from inside of us (our internal conflicts: e.g. envy, jealousy, hatred, love, etc..). Some positive events also cause stress: e.g. marriage, having a new child, having a new work, having a car etc…
Stress increases the release of adrenocorticotropic hormone (ACTH), which leads to the release of cortisol, activation of the autonomic nervous system, and altered levels of neurotransmitters (e.g., serotonin, norepinephrine).
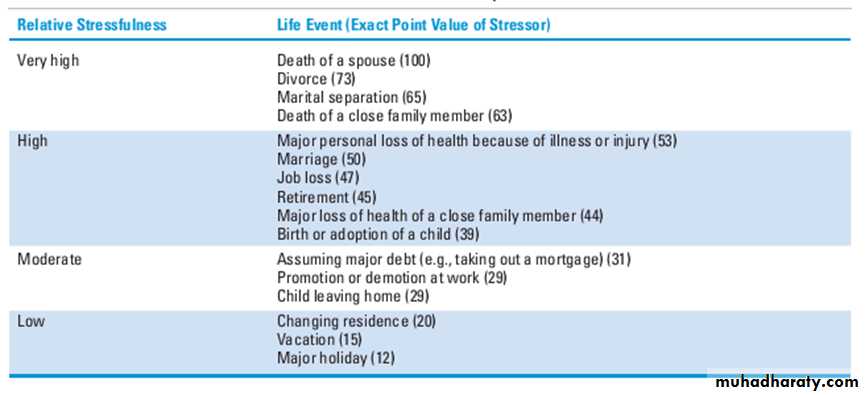
The Social Readjustment Rating Scale by Holmes and Rahe (which also includes “positive” events like holidays) ranks the effects of life events. Events with the highest scores require people to make the most social readjustment in their lives.
The need for social readjustment is directly correlated with increased risk of medical
and psychiatric illness; in studies by Holmes and Rahe, 80% of patients with a score of 300 points in a given year became ill during the next year. الجدول التالي ليس للحفظ
Stress is natural, we experience it for a reason. Usually short-lived and have benefits:
Make you active and alert.
Boost immune system and heal wounds (adrenaline and cortisol).
Chronic stress: higher rates of digestive, respiratory, circulatory, and infectious disease.
There is little or no evidence to support that stress:
is a major cause of coronary artery disease (atherosclerosis) Davidosn’s p. 581causes hypertension. Davidson’s P. 607
Nevertheless it seems that stress has some role in irritable bowel syndrome, fibromyalgia, and it may exacerbate psoriasis, and precipitate angina. And psychological stress is listed as a cause for delayed puberty and hyperprolactinemia.
Of course the word stress is used in medicine sometime not to describe psychological stress but to refer to:
Severe physiological stress, e.g. burns, multi-organ failure
Stress as in (Stress echocardiography) which refers to exercise or pharmacothcological stress.
Oxidative stress.
Glucocorticoids are double edges swords:
Glucocorticoids mobilize energy (ex. By inhibiting glucose uptake) from body organs to the muscles, help you to survive stress. They help us not to lose energy during stressful time doing: digestion, growth, reproduction, building new tissues, etc. That would be helpful for short times but not for long times. Chronic high levels of glucocorticoids are found to cause dendritic atrophy, and interruption with long term potentiation. Estrogen is protective. There is what is called as (Steroid dementia syndrome) which occur in Cushing’s disease.
Individual differences in responding to stressful life events:
Not all the people who face stressful events develop long chronic reactions. There are some factors that affect that which include:
Personality style (type A behavior increase stress) People with type A behavior are extremely competitive and achievement oriented, they have a sense of time urgency finding difficult to relax and become impatient and angry when confronted with delays or with people whom they view as incompetent, they have self-doubt, and push themselves to accomplish more and more in less and less time.Cognitive appraisal of the stress. (Our explanation to what had happened affects our stress reaction). Social isolation increases stress.
ATTACHMENT AND DEVELOPMENT
Attachment can be defined as the emotional tone between children and their caregivers which starts since first month of age and it develops gradually.
Attachment theory originated in the work of John Bowlby, a British psychoanalyst (1907–1990). In his studies of infant attachment and separation, Bowlby pointed out that attachment is an essential medium of human interaction that had important consequences for later development and personality functioning.
The term bonding concerns the mother’s feelings for her infant and differs from attachment.
Attachment is present as an instinct in animals, and there is a critical period for it early in the newborn’s development.
Harry Harlow (1905-1981) studies the emotional and behavioral effects of isolating monkeys from birth and keeping them from forming attachments. The isolates were withdrawn, unable to relate to peers, unable to mate, and incapable of caring for their offspring.
In a series of experiments, Harlow separated rhesus monkeys from their mothers during their first weeks of life. During this time, the monkey infant depends on its mother for nourishment and protection, as well as for physical warmth and emotional security—contact comfort, as Harlow first termed it in 1958. Harlow substituted a surrogate mother made from wire or cloth for the real mother. The infants preferred the cloth-covered surrogate mother, which provided contact comfort, to the wire-covered surrogate, which provided food but no contact comfort.
Insecure Attachment
Mary Ainsworth (1913–1999) described three main types of insecure attachment: avoidant, ambivalent, and disorganized.The avoidant child, due to aggressive parenting, tends to avoid close contact with people and lingers near caregivers rather than approaching them directly when faced with a threat.
The ambivalent child finds exploratory play difficult, even in the absence of danger, and clings to his or her inconsistent parents.
Disorganized children have parents who are emotionally absent with a parental history of abuse in their childhood. These children tend to behave in bizarre ways when threatened. According to Ainsworth, disorganization is a severe form of insecure attachment and a possible precursor of severe personality disorder and dissociative phenomena in adolescence and early adulthood.
Separation from mother for long periods can lead to: Failure-to-thrive syndromes, psychosocial dwarfism, separation anxiety disorder, avoidant personality disorder, depressive disorders, delinquency, academic problems, and borderline intelligence have been traced to negative attachment experiences.
What is a transitional object?
In childhood development, the term transitional object is used to refer to a physical object, which takes the place of the mother-child bond. Common examples include dolls, teddy bears or blankets. That object can give feeling of security to the child, and is usually used by the child during the period when the he is training to be separated from the mother and living independently.NORMAL ANXIETY DURING DEVELOPMENT
Bowlby’s theory of anxiety holds that a child’s sense of distress during separation is perceived and experienced as anxiety and is the prototype of anxiety. Stranger anxiety, an anxiety response to someone other than the caregiver, appears at 8 months of age. Separation anxiety is the response of a child who is isolated or separated from its mother or caretaker. It is most common at 10 to 18 months of age and disappears generally by the end of the third year. When the mother is close to the child and the child experiences no fear, the child gains a sense of security, the opposite of anxiety. When the mother is unavailable to the infant because of physical absence (e.g., if the mother is in prison) or because of psychological impairment (e.g., severe depression), anxiety develops in the infant.References:
Fadem, B. (2015) Behavioral Sciences 6th EditionDavidson’s principle and practice of medicine 22nd Ed.
Robet Sapolsky lecture at the NIH “Stress and Health: From Molecules to Societies” 2009 (from the youtube.com)
19th Oct. 2015 Monday Al-Mustansiriya Medical College. Psychiatry Lecture. Dr. Sami Adil
19th Oct. 2015 Monday Al-Mustansiriya Medical College. Psychiatry Lecture. Dr. Sami AdilTrauma and Stressor-Related disorders:
Post-traumatic stress disorder (PTSD)
Acute stress disorder (ASD)
Adjustment disorder
Reactive attachment disorder
Disinhibited social engagement disorder
PTSD and ASD
In the DSM-IV, PTSD was regarded as one of the anxiety disorders. In DSM 5 it is classified under (Trauma and Stressor-Related disorders). ASD and PTSD are characterized by severe anxiety symptoms and follow a threatening event. The threatening event is not only threatening life, but also it can be about injury, or sexual violation. Natural disasters, accidents, being kidnapped, being diagnosed with a life-threatening illness. The threat can be direct, or occurred to a close person.
In ASD the anxiety lasts less than one month but more than 2 days, while in PTSD the anxiety lasts more than one month.
Etiology/ Risk factors:
Risk Factors are: substance abuse, personality disorder (borderline, paranoid, dependent, or antisocial), childhood trauma, being a female, inadequate support, external locus of control, etc.
Psychodynamic model of the PTSD hypothesizes that the trauma has reactivated a previously quiescent ساكن، هادئ , yet unresolved psychological conflict. The revival of the childhood trauma results in regression and the use of the defense mechanisms of repression, denial, reaction formation, and undoing. Cognitive-Behavioral model of PTSD stresses the importance of avoidance, conditioning, and reinforces.
Biological Factors
The noradrenergic and endogenous opiate systems, as well as the HPA axis, are hyperactive in some patients with PTSD. Other major biological findings are increased activity and responsiveness of the autonomic nervous system, as evidenced by elevated heart rates and blood pressure readings and by abnormal sleep architecture (e.g., sleep fragmentation and increased sleep latency).
Prevalence:
The IMHS estimated the life time prevalence in Iraq to be 3.5% of the general population (1) . There are many other Iraqi studies on the prevalence of PTSD which found higher prevalence (e.g. 13.4% in the Kurdish soldiers in Iraqi army (2), 48% in the casuality staff in Mosul city (3), and 25% in secondary school students in Baghdad(4). The variability in these prevalence rates is due to the different methodology used by researchers: e.g. different sample size, or different diagnostic tools: some have used questionnaires rather than psychiatric interview). Same differences in point-prevalence rate occur in American studies about PTSD in US army in Iraq 2-20% of veterans (5).PTSD presenting symptoms are four symptom groups:
Re-experiencing of the traumatic event (nightmares, flashbacks).
Avoidance of stimuli associated with the trauma (phobic avoidance)
Increased arousal, such as increased anxiety, aggression, sleep disturbances, and Hypervigilance. reckless or self-destructive behavior
Negative thoughts and mood or feelings — For example, feelings may vary from a persistent and distorted sense of blame of self or others, to estrangement from others or markedly diminished interest in activities, to an inability to remember key aspects of the event.
There are 2 subtypse:
Preschool subtype (include similar criteria but some different details)
Dissociative subtype (include symptoms like: seeing the world unreal, dreamlike, detached from one’s own body, mind, experience. etc.)
DIFFERENTIAL DIAGNOSIS
Treatable medical contributors to posttraumatic symptomatology (head injury, epilepsy, and substance-related disorders). Symptoms of PTSD can be difficult to distinguish from both panic disorder and GAD, because all three are associated with prominent anxiety and autonomic arousal. Borderline PD can be difficult to distinguish from PTSD. The two disorders can coexist or even be causally related.Comorbidity:
Comorbidity rates are high among patients with PTSD, with about two thirds having at least two other disorders. Common comorbid conditions include depressive disorders, substance-related disorders, anxiety disorders, and bipolar disorders.ASD and PTSD treatment:
Psychoeducation is an important first step in the treatment of ASD. There is some evidence that brief CBT, including exposure and cognitive challenging. Pharmacotherapy is not generally recommended in ASD, but it is used in PTSD.Recommended treatments for PTSD focus on confronting the memories and reminders of the traumatic event, as well as addressing associated unhelpful thoughts and beliefs. They include trauma-focussed cognitive behaviour therapy (TF-CBT) which include exposure therapy (imaginary and in vivo) and eye movement desensitisation and reprocessing (EMDR).
Group psychotherapy with other survivors.
Pharmacotherapy: SSRIs (sertraline and paroxetine are FDA approved), Antidepressants, and Benzodiazepines (be aware or risk of abuse of benzodiazepines). Atypical antipsychotics have been used in this role but with limited research evidence base. Use of clonidine, prozosin, and propranolol, which are antiadrenergic agents, is suggested by the theories about noradrenergic hyperactivity in the disorder.
Onset and Course:
Symptoms usually begin immediately after the trauma, but can occur months or years later. Untreated, about 30 % of patients recover completely, 40 % continue to have mild symptoms, 20 % continue to have moderate symptoms, and 10 % remain unchanged or become worse. A good prognosis is predicted by the absence of the risk factors
Adjustment Disorders
These disorders represent a simple response to some type of life stress (whether traumatic or not). Usually the stressor less severe than PTSD. And the symptoms does not contain the four criteria of PTSD. There is no evidence that pharmacotherapy is helpful. The subtypes are: depressed mood, anxious symptoms, or disturbances in conduct.
Reactive Attachment Disorder
Due to insecure attachments, the child has a dampened خامد، مثبط، واهن positive affect — the child expresses joy or happiness in a very subdued خاضع، لطيف or restrained manner.
Disinhibited Social Engagement Disorder
It more closely resembles ADHD. It may occur in children who may have secure or insecure attachment. The child actively approached unfamiliar adults.
References:
Iraqi Mental Health Survey 2006-2007
Saman Anwar Faraj. Prevalence of PTSD among Kurdish soldiers in Iraqi army. 2008. A non-published thesis.
Zyad Tariq Afram. PTSD among staff of casuality department in Mosul city. 2007. A non-published thesis.
Yousif Salim Alwan Al-Aubaidi. Prevalence of acute PTSD among secondary school students in Baghdad. 2005. A non-published thesis.
Lisa K. Richardson, B. Christopher Frueh, and Ronald Aciemo. Prevalence Estimates of Combat-Related PTSD: A Critical Review. Aust N Z Psychiatry. 2011 January 1.