Stomatitis
Is a general term used to describe an inflammation of the whole lining of the mouth.Viral infection: Herpes simplex
Bacterial: Gingivitis, periodontitis and actinomycosis.
Fungal: candidiasis (thrush).
Spirochaetes: Vincent's angina.
Miscellaneous: Aphthus, Behcets syndrome, pemphigus and pemphigoid.
Oral Ulceration
1- Aphthus
Recurrent ulceration of the oral mucosa of unknown aetiology. Viral, psychogenic, endocrinal and autoimmune factors have been suggested. Sometimes aphthus is due to deficiency of iron, folate or B12. Persistent aphthus ulceration especially in young males, must bring to mind the possibility of AIDS.
Clinical Picture
It's started as a small vesicle, which soon ulcerates leaving an ulcer which varies in size. This ulcer is typically quite sensitive and painful. It has a central necrotic base with a surrounding red circumference and it disappears after a few days.
Aphthus ulcers are of two types.
The minor form, which is more common, the ulcers are multiple and 3-6 mm in size. They heal within 7-10 days with no scars.
The major form, ulcers are 1-2 cm in size, less common, long lasting and heal with a scar.
Treatment: is symptomatic:
Oral antiseptic: like chlorhexidine gurgle.
Topical application of local analgesic like xylocaine.
Topical steroids e.g. Kenalog in orabase. Systemic steroids should be used only in major aphthus ulceration.

Aphthus ulcer
2- Acute Necrotizing Gingivitis (Vincent's Angina)It's a gingivitis affecting the interdental papillae producing ulceration and necrotic membrane. This entity was called "Trench Mouth" because of its prevalence in soldiers fighting in the trenches during world war I.
Aetiology:
Infection with spirochaete Borrelia vincenti and an anaerobic organism Bacillus fusiformis.Clinical Picture
This condition occurs in debilitated patients who have poor dental hygiene. The patient feels ill, pyrexial complaint from sore throat with tender lymphadenopathy.
Examination
The lesions originate around the interdental papillae and gums and may spread to involve the tonsil and oropharyx. The ulcers are painful, associated with foetor (fishy odor), whitish grey in colour and covered by a slough. It can be diagnosed by bacteriological study with gram stain and culture.
Treatment
Oral hygiene.Antibiotics like penicillin + metronidazole for anaerobes.
Vincent,s angina
Herpetiform ulcerationsThese ulcers are not necessary herptic in otigin, although they are similar in appearance to herpetic ulcers. They are more common in females. They don't respond to steroid therapy, but the use of tetracycline mouthwashes is effective.
Trauma
Persistent irritation of an area of the mucosa by ill-fitting dentures or sharp teeth can case oral ulceration. Treatment is that of the underlying cause.
HIV infection
Oral manifestations of AIDS are: Oral candidiasis, Herpes virus infection and Bacteral infection, like atypical mycobacterial infection.Ludwig's Angina
It is acute cellulitis of the floor of the mouth and submandibular space secondary to soft tissue infection. The infection is limited by the attachment of the fascial spaces, so that tension rises rapidly and laryngeal oedema occasionally occurs.
Aetiology
Root abscess of the lower premolar and molar teeth (80%). The most usual organisms are streptococcus viridans and E. coli.
Tonsillar infection.
Submandibular sialadenitis.
Clinical Picture
The patient is ill, toxic > 38 oC with odynophagia and salivation.
On examination there is an indurated and usually non-fluctuant swelling below the angle of the jaw. The floor of the mouth becomes very oedematous with the tongue pushed upwards.
Potential complications
Airway compromise due to laryngeal oedema.
Spread into the parapharyngeal and retropharyngel spaces.
Septicaemia.
Aspiration pneumonia.
Treatment
Early stages (early cellulitis): Heavy antibiotics covering aerobes and anaerobes..
Drainage: If the state progress and the swelling increases. Fluctuation should on no account be awaited because it seldom occurs. Draining is by a curved incision 2 cm below the angle of the jaw.
Endotracheal intubation and tracheostomy may be required if laryngeal oedema supervenes.

Ludwig,s angina
Pharyngitis
Acute PharyngitisIt is acute inflammation of the mucous membrane of the pharynx occurring primarily in winter months. Pharyngitis must be differentiated from tonsillitis although the latter may be associated with generalized inflammation of the pharynx, and the oropharynx is the site mainly affected.
Aetiology
The majority are caused by viral infection( mostly adenovirus and rhinovirus). Bacterial infections mostly Pneumococci, Haemophilus influenza and group A beta-hemolytic streptococci (S. Pyogens) can occur primarily or secondary to viral infection. Recurrent pharyngitis can be caused by post-nasal drip, smoking or gastro-esophageal reflux disease (GERD).
Pharyngitis may be part of the clinical picture of measles, scarlet fever, infectious mononucleosis and typhoid fever.
Symptoms
Sore throat accompanied by a feeling of coldness.
Pyrexia, headache and joint pain.
Sings
Redness and injection the mucous membrane of the pharynx.
Hypertrophy and proliferation of lymphoid tissue on the posterior pharyngeal wall with particular aggregates in the lateral pharyngeal bands.
Edema of uvula.
Tender and palpable cervical lymphadenopathy.
Treatment
Simple pharyngitis is usually a self-limiting disease, lasting for 3-4 days; so treatment is only symptomatic by bed rest, analgesics and increase fluid intake. Antibiotics are given if bacterial infection is suspected. The antibiotic of choice is penicillin group like amoxicillin, or augmented amoxicillin. Macrolides can be given to penicillin allergic patients.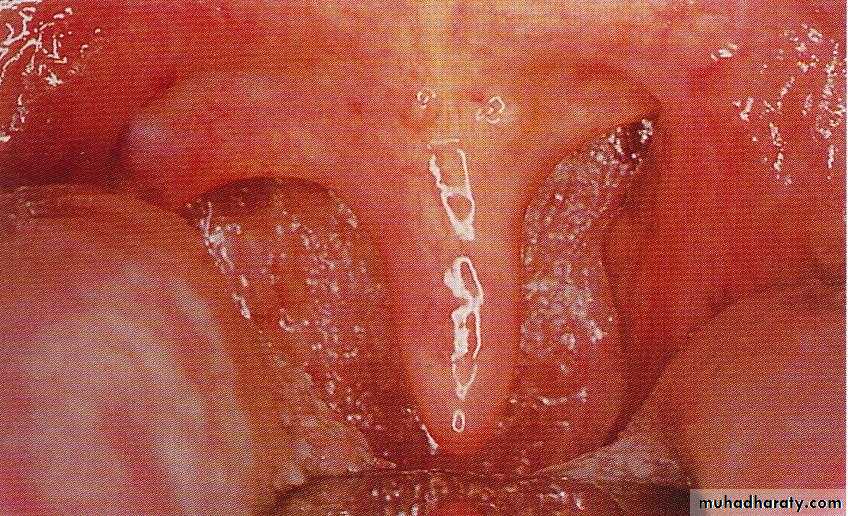
Acute pharyngitis
Acute TonsillitisThis is a generalized inflammation of the mass of the tonsil which is usually accompanied by a degree of inflammation of the pharynx. Acute tonsillitis may affect any age group, but its most frequently found in children.
Aetiology
The infecting agents may be bacteria and/or viruses. It is considered that bacterial infections are often secondary opportunistic invaders following a virus infection. The most common bacteria isolated were group A B-haemolytic streptococcus, pneumococcus, staphylococcus and Haemophilus influenzae. Anaerobes have been found, but there significance is not fully known.
Symptoms
Sore throat which is made worse by swallowing (odynophagia).
Constitutional symptoms are more severe than acute pharyngitis especially in children.
Referred otalgia and abdominal pain due to mesenteric adenitis.
Examination
The tongue is furred and the breath is offensive (halitosis).
The tonsils are enlarged red and swollen. The crypts become filled with pus producing the follicular appearance (follicular tonsillitis). These follicles may coalesce forming a patchy membrane on the surface of the tonsil (membranous tonsillitis).
The cervical lymph nodes are enlarged and tender.
Differential Diagnosis
Scarlet fever: is streptococcal infection in which the streptococcus produces the erythrogenic toxin which results in an erythematous rash. Here the tongue has a strawberry appearance and the whole skin is hot and soon develops a punctate erythema.
Glandular fever: infectious mononucleosis.
Agranulocytosis and leukaemia.
Acute diphtheria.
Vincent's angina.


Acute tonsillitis Scarlet fever
Complications
local
a. peritonsillar abscess(quinsy): is collection of pus between the tonsil and its bed.
b. Retropharyngeal abscess.
c. Parapharyngeal abscess.
d. Acute otitis media: following extension of infection to the middle ear through the Eustachian tube.
General
Rheumatic fever and glomerulonephritis which follow B-haemolytic streptococcal tonsillitis of Lancet group A.
Subacute bacterial endocarditis.
c. Septicaemia: in untreated conditions.
Treatment
I-Medical
1. Bed rest, soft diet and encourage fluid intake.
2. Antipyretics and analgesics. Paracetamol, NSAI drugs.
3. Antibiotics: Penicillin for 7-10 days starting by paranteral benzylpenicillin to be continued by oral penicillin. If the patient is allergic to penicillin erythromycin. Lack of response may suggest the presence of B-lactamase producing organism or even an anaerobic one, in which augmentin and metronidazole will be the antibiotic of choice.
II-Surgical: tonsillectomy.
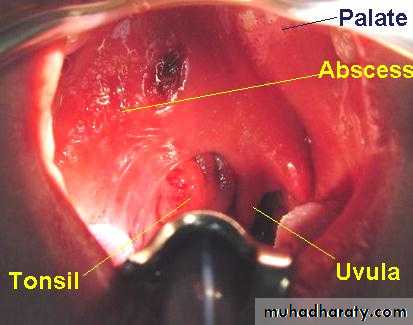
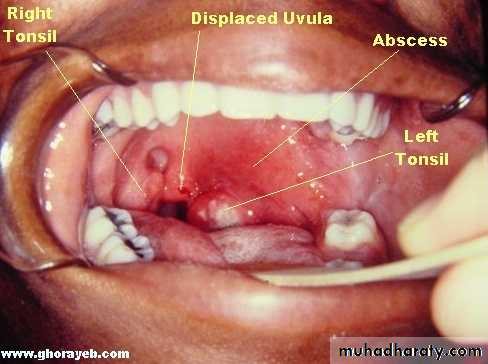
Peritonsillar Abscess (Quinsy)
Is a collection of pus between the fibrous capsule of the tonsil and the superior constrictor. It’s usually unilateral and most frequently affects adult males. Quinsy generally arises as a complication of acute tonsillitis.
Clinical Picture
1. The patient looks ill, feverish with rigor .
2. Acute sore throat radiating to the ear (referred otalgia) with painful swallowing (odynophagia). This makes the saliva dribbles from the month.
3. Trismus due to irritation of the pterygoid muscles .
4. Thick and muffled voice often called “hot potato voice”.
Examination
It may be difficult because the patient can not open his mouth.
1. The tonsil is congested and pushed medially with the soft palate bulging downward and forward. The uvula may be pressed against the opposite tonsil.
2. Red and enlarged anterior tonsillar pillar.
3. Tender and enlarged cervical lymph nodes.
Differential Diagnosis
1. Dental abscess of the upper molar tooth.
2. Parapharyngeal swelling.
Treatment
I. Medical (as acute tonsillitis): Effective in early peritonsillar cellulitis.
II. Surgical : when considerable swelling is present or in case of failure to medical treatment.
Incision of the abscess: this is undertaken at the point of maximum swelling of the soft palate. The classical site is at a point where an imaginary line through the base of the uvula is intersected by a perpendicular line from the junction of the anterior tonsillar pillar with the tongue.
Tonsillectomy may be indicated 6-8 weeks following quinsy.
2. Abscess tonsillectomy