


D R . A M M A R T A L I B A L - Y A S S I R I
C O L L E G E O F M E D I C I N E / B A G H D A D
U N I V E R S I T Y
Injuries of elbow and forearm
bones
FRACTURES OF THE LATERAL CONDYLE
Mechanism of injury and pathology
The child falls on the hand with the elbow extended and forced
into varus.
A large fragment, which includes the lateral condyle, breaks off
and is pulled upon by the attached wrist extensors
C/F:
The elbow is swollen and deformed.
tenderness over the lateral condyle.
Passive flexion of the wrist (pulling on the extensors) may be
painful.

X-ray
Two types of fracture are recognized and classified by Milch:
TYPE I(A fracture lateral to the trochlea): the elbow joint is not
involved and is stable.
Type II( A fracture through the middle of the trochlea): this
injury is more common; the elbow is unstable
the fragment (partly cartilaginous) is much larger than it
seems on x-ray.

Treatment
if there is no displacement
the arm can be splinted in a backslab with elbow flexed 90 degrees,
the forearm neutral and the wrist extended
it is essential to repeat the x-ray after 5 days to make sure that the
fracture has not displdced,
The splint is removed after 2weeks and
exercises are encouraged.
dispaced fracture
requires accurate reduction and internal fixation (if merely hinged )by
closed reduction and percutaneous pins. If this fails, and for all
separated fractures ORIF
The arm is immobilized in a cast; cast and pins are removed after 3-
4wks

Complication
Non-union and malunion
Nonunion lead to cubitus valgus deformity and the ulnar nerve
palsy can develop
Recurrent dislocation
Occasionally Condylar displacement results in posterolatertl
dislocation of the elbow.
The only effective treatment is reconstruction of the bony and soft
tissues on the lateral side.

SEPARATlON OF THE MEDIAL
EPICONDYLE
Mechanism of injury
falls on the out stretched hand with the wrist and elbow
extended; the elbow is wrenched into valgus.
The unfused epicoudylar apophysis is avulsed
If the elbow subluxates (even momentarily), the small
apophysial fragment may be dragged into the joint.
With more severe injuries the joint dislocates laterally,
C/F:
pain, swelling and bruising on the medial side of the elbow.
Sensation and power in the fingers should be tested

X-ray
In the AP view the medial epicondylar epiphysis may be tilted
or shifted downwards;
A lateral view may show the epicondyle looking like a loose
body in the joint.
treatment
Minor displacement may be disregarded.
lf the epicondyle is trapped: Manipulation with the elbow in
valgus and the wrist hyperextended
if there is valgus instability then reduction and pinning is
recommended

Complications
EARLY
Ulnar nerve damage is not uncommon. Mild symptoms recover
spontaneously
LATE
Stiffness of the elbow is common and extension often limited for
months; but, provided movement is not forced, it will eventually
return.

FRACFURES OF THE MEDlAL CONDYLE
Mechanism of injury
a direct blow to the point of the elbow
a landing on the outstretched hand with the elbow forced into
valgus
Clinical features and x-ray
pain and swelling
ln older children the metaphyseal component is usually easily
visualized on x-ray
in young children epicondylar ossific centre is seen in a
displaced position on x-ray

Tratment
Undisplaced: by splintage
Displaced: closed reduction + percutaneous pinning or ORIF
Postop as in lat. Cond.
Complications:
Early
Lat. Dislocation of the elbow
Ulnar n. damage
Late
stifness
FRACTURED NECK OF RADIUS
Mechanism of injury and pathology
A fall on the outstretched hand forces the elbow into valgus and
pushes the radial head against the capitulum
C/F
pain in the elbow.
localized tenderness over the radial head
pain on rotating the forearm
X-ray fracture line is transverse.
either situated immediately distal to the physis or
there is true separation of the epiphysis with a triangular fragment
ofshaft La Salter-Harris II injury).
The proximal fragment is tilted distally, forwards and outwards.

Treatment
Up to 30 degree tilt and 3mm of displacement arm rested in
collar and cuff and exercises commenced after a wk.
> 30 degree need reduction (closed or open)
Fractures that are seen a week or longer after injury should be
left untreated (except for light splintage)
Following operation, the elbow is splinted in 90 degrees of
flexion for a week or two and then movements are encouraged.

SUBLAXATION OF THE RADIAL HEAD
(’PULLED ELBOW')
In young children the elbow may be injured by
pulling on the arm, usually with the forearm
pronated
A child aged 2 or 3 years is brought with a painful,
dangling arm: there is usually a history of the child
being jerked by the arm and crying out in pain.
The forearm is held in pronation and extension, and
any attempt to supinate it is resisted.
There are no x-ray changes,
A dramatic cure is achieved by forcefully supinating
and then flexing the elbow
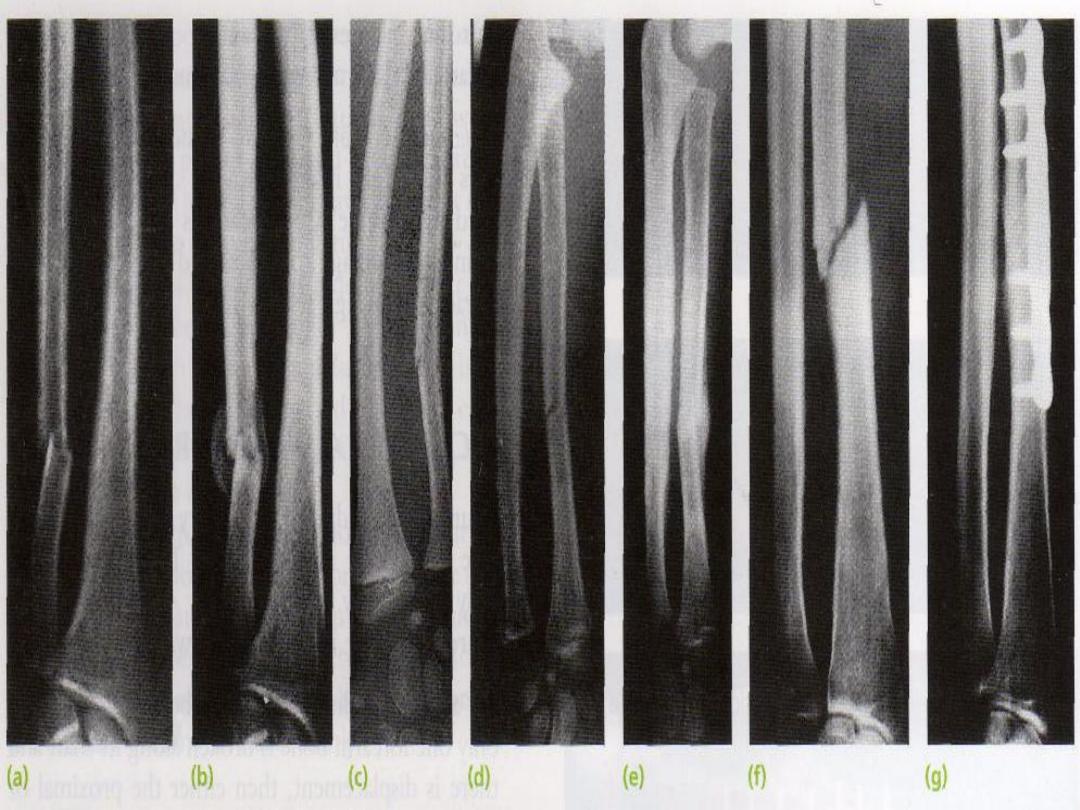
Fracture of the radius and ulna
Mechanism of injury
Twisting force lead to spiral fracture with bone broken at
different level
Angulating force cause transverse fracture at the same level
Direct force cause transverse fracture of one bone usually the
ulna
Additonal rotation deformity caused by the pull of the attached
muscles

C/F:
The fracture is quite obvious
The hand is examined for vascular and neural deficit
X-ray: both bones are broken either
transverse at the same level
Or oblique at different level with radius usually higher
In children it is incomplete and only angulated (greenstick)

Treatment
In children
closed reduction with the fragment held by full length well molded
cast (axilla to metacarpal shaft)
Splintage is retained for 6-8wk
Operation is required if the reduction failed or unstable
Adults
ORIF with plate and screws
Open fractures
wound excision with fixation of the fracture with external fixation
as a temporary measure then changed to plate and screws (bone
graft sometimes is needed)

Complications
Early
Nerve injury
Vascular injury
Compartment syndrome
Late
Delayed union and nonunion
Bone grafting and internal fixation
Malunion
With closed reduction
Angulation, rotational deformity, cross union or shortening of one
bone with disruption of distal RA joint
Mobility my be improved by corrective osteotomy
Complication of plate removal
FRACTURE
OF
A
SINGLE
FOREARM
BONE
very rare
usually caused by a direct blow - the 'nightstick fracture'.
They are important for two reasons:
An associated dislocation may be undiagnosed
Non-union is liable to occur
C/F: Ulnar fractures are easily missed even on x-ray. If
there is local tenderness, a further x-ray a week or two
later is wise.
X-ray
The fracture line is transverse and displacement is slight.
In children('plastic deformation').
Treatment
Isolated fracture of the ulna :a forearm brace leaving the
elbow free can be sufficient. (8 weeks)
Isolated fracture of the radius:
to achieve reduction in children the forearm needs to be supinated
for upper third fractures, neutral for middle third fractures and
pronated for lower third fractures.
sometimes difficult to hold in children and just about impossible
in adults ORIF
Middle/distal third fractures of the radius in children above-
elbow cast in supination, if failed ORIF

MONTEGGIA FRACTURE-DISLOCATION OF
THE ULNA
described by Monteggia in the early nineteenthth
century (without benefit of x-rays!)
fracture of the shaft of the ulna associated with
dislocation of the proximal radio-ulnar joint; the
radio-capitellar joint is inevitably dislocated or
subluxated as well.
Classification:
Type I apex ant+ radial head displaced ant
Type II apex post+ radial head displaced post
typeIII apex lat+ radial head displaced lat

Mechanism of injury: fall on the hand with forcibly pronate
the forearm. Sometimes the causal force is hyperextension.
C/F:
deformity
swelling.
pain and tenderness on the lateral side of the elbow.
signs of injury to the radial nerve.
X-ray
the head of the radius (which normally points directly to the capitulum)
is dislocated forwards, and there is a fracture of the upper third of the
ulna with forward bowing.
Backward or lateral bowing of the ulna (which is much less common) is
likely to be associated with, respectively, posterior or lateral
displacement of the radial head.
Trans-olecranon fractures, also, are often associated with radial head
dislocation.

Treatment
The key to successful treatment is to restore the length of the
fractured ulna
In adults, ORIF
In children
Incomplete ulnar fractures can often be reduced closed then
immobilized in a cast with the elbow in flexion and supination, for
3 weeks.
Complete fractures : ORIF

Complications
Nerve injury Nerve injuries can be caused by over-enthusiastic
manipulation of the radial dislocation or during the surgical
exposure.
Malunion :In children, no treatment is advised. In adults,
osteotomy of the ulna or perhaps excision of the radial head
may be needed.
Non-union : Non-union of the ulna should be treated by
plating and bone grafting
GALEAZZI FRACTURE-DISLOCATION OF THE
RADIUS
Mechanism of injury: fall on the hand; probably with a
superimposed rotation force
C/F
Prominence or tenderness over the lower end of the ulna is the
striking feature
(the 'piano-key sign')
test for an ulnar nerve lesion
X-ray: A transverse or short oblique fracture is seen in
the lower third of the radius, with angulation or overlap.
The distal radioulnar joint is subluxated or dislocated
TREATMENT:In children, closed reduction is often
successful; in adults, reduction is best achieved by ORIF

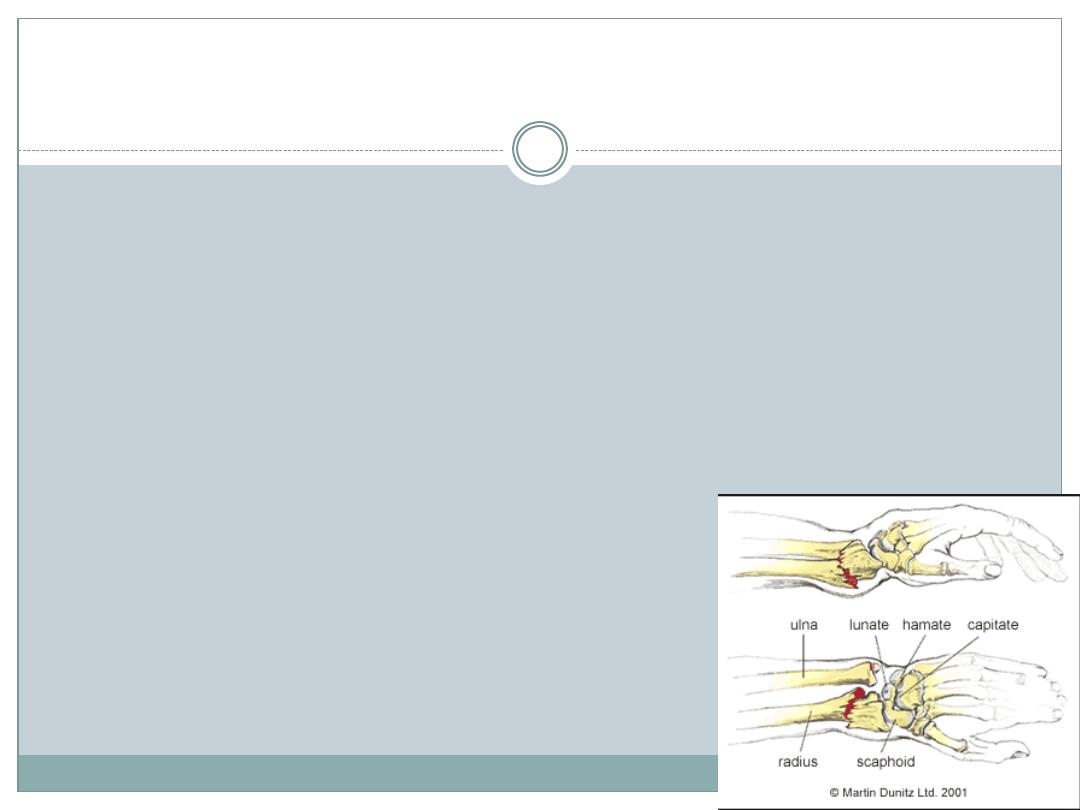
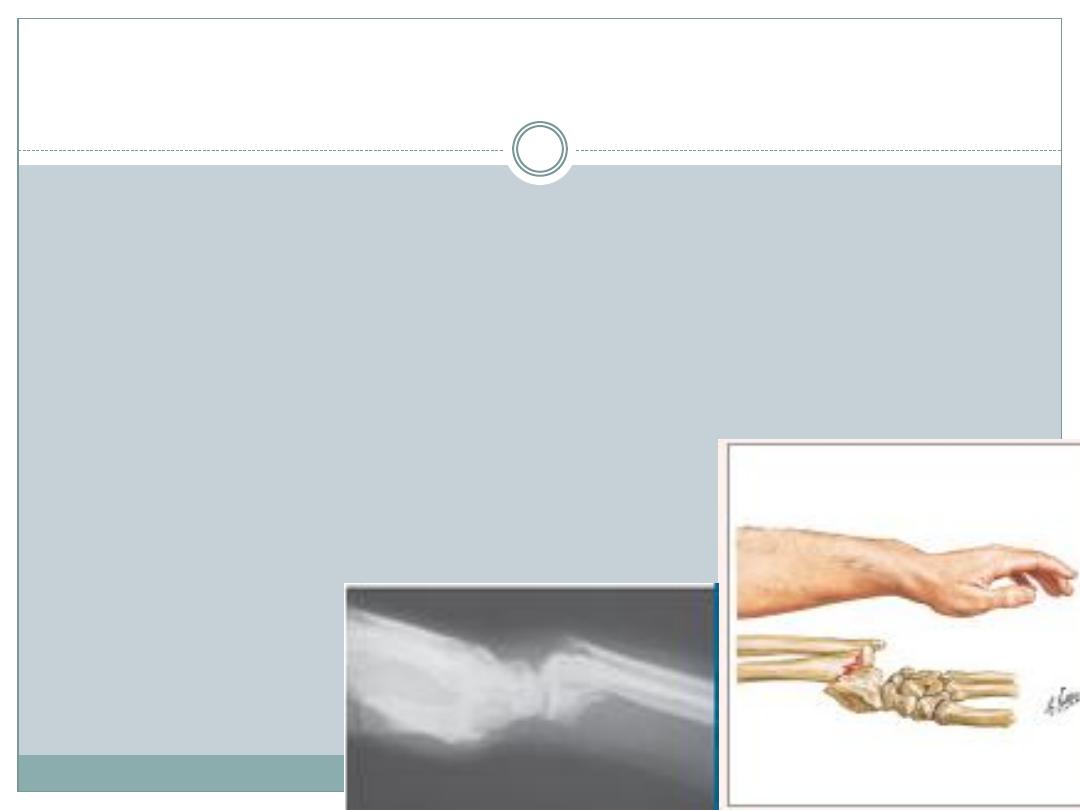
COLLES' FRACTURE
transverse fracture of the radius just above the wrist,
with dorsal displacement of the distal fragment
The most common of all fractures in older people
Mechanism of injury and pathological anatomy
Force is applied in the length of the
forearm with the wrist in extension
the distal fragment collapses into
extension, dorsal displacement,
radial tilt and shortening
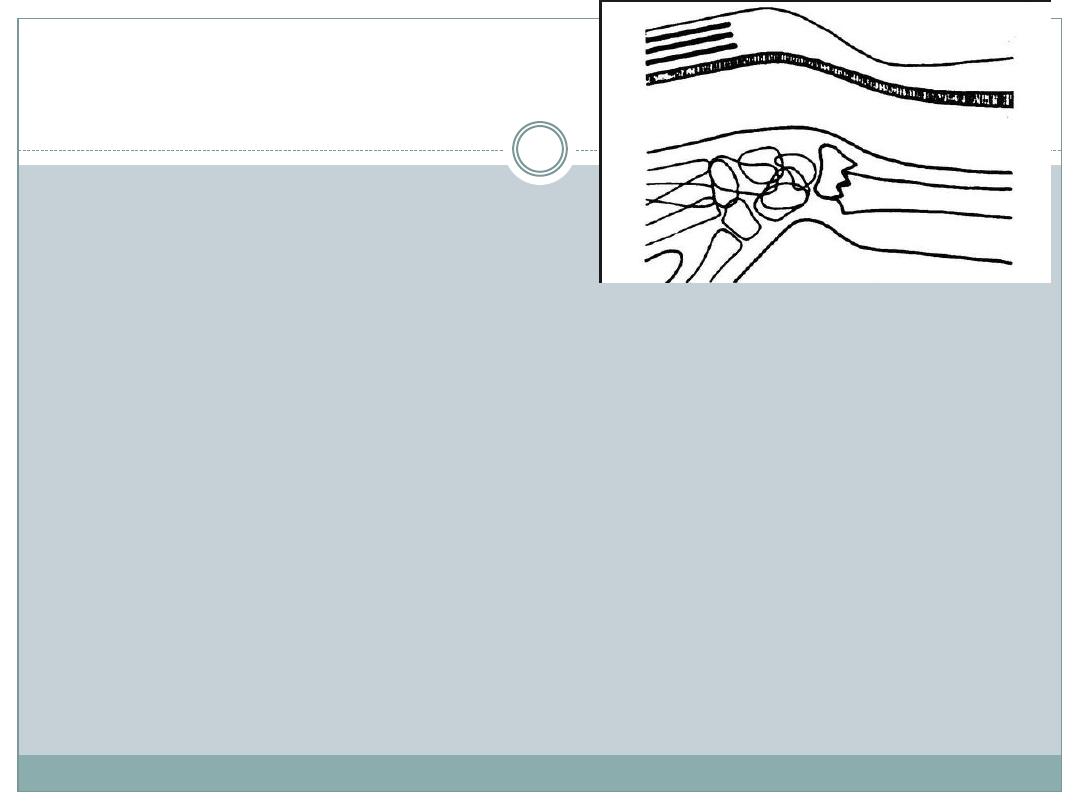
Clinical features
'dinner-fork' deformity
local tenderness and pain on wrist movements.
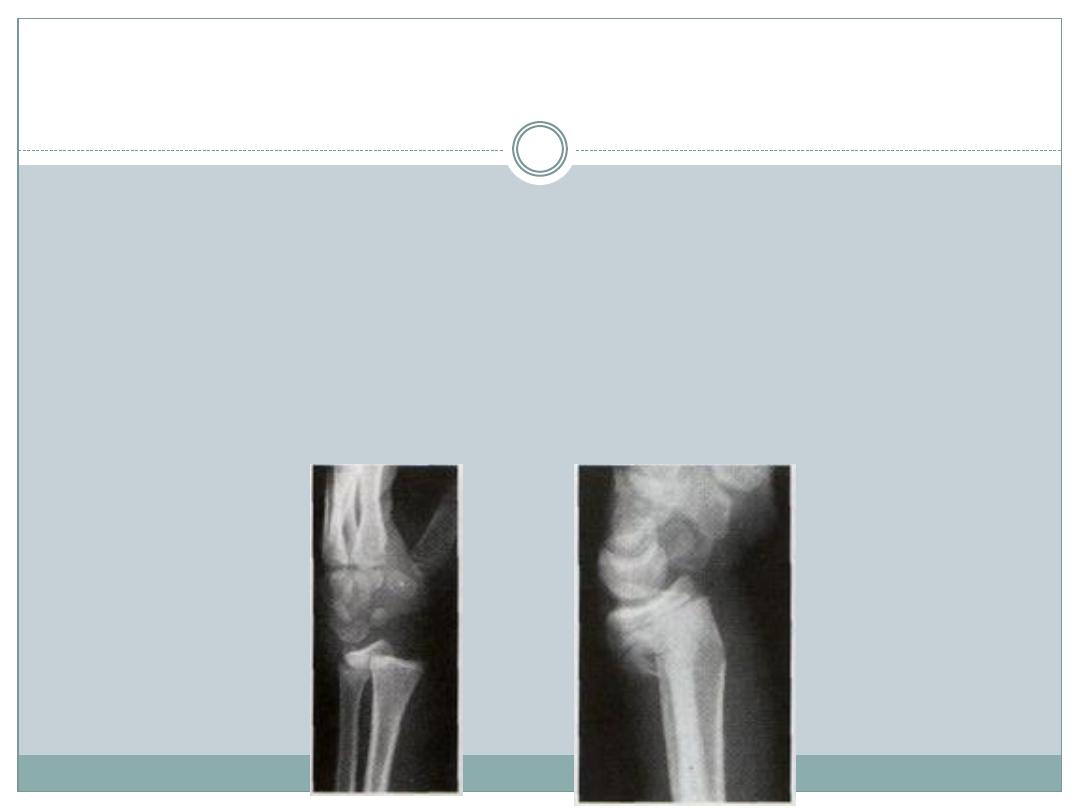
X-ray
There is a transverse fracture of the radius at the
corticocancellous junction,
the ulnar styloid process is broken off.
The radial fragment is impacted into radial and backward tilt
Treatment
UNDISPLACED FRACTURES
a dorsal splint is applied for 1-2 day until the swelling has resolved,
then the cast is completed.
An x-ray is taken at 10-14 days
the cast can usually be removed after
four weeks to allow mobilization.
DISPLACED FRACTURES
reduced under anaesthesia
dorsal plaster slab is applied for 6 wks
IMPACTED OR COMMINUTED FRACT.
CR+ percut. pins or ext. fix. for 5-6 wks
ORIF 'volar locking plate'
Complications
EARLY
Circulatory problems
Nerve injury
Reflex sympathetic dystrophy (Sudeck's atrophy)
TFCC injury
LATE
Malunion: common
Delayed union and non-union :rare
Stiffness
Tendon rupture (extensor pollicis longus)
SMITH
'
S
FRACTURE
distal fragment is displaced anteriorly “reversed
Colles”
a fall on the back of the hand
C/F: a wrist injury+a 'garden spade' deformity.
X-ray a lateral view shows that
the distal fragment is displaced
and tilted
anteriorly

Treatment
The fracture is reduced by traction, supination and extension
of the wrist, and the forearm is immobilized in a cast for 6
weeks
X-rays should be taken at 7-10 days.
Unstable fractures should be fixed with percutaneous wires or
a volar plate

DISTAL FOREARM CHILDREN
The distal radius and ulna are among the commonest
sites of childhood fractures.
Either through the physis or in the metaphysis
Mechanism of injury
the usual injury is a fall on the outstretched hand with the
wrist in extension (displaced post.)
Sometimes the wrist in flexion (displaced ant.)
Lesser force may do no more than buckle the metaphyseal
cortex
C/F: The wrist is painful,swollen; sometimes there is
an obvious 'dinner-fork' deformity.
X-ray
Physeal fractures Salter-Harris type I or II with the epiphysis
shifted and tilted backwards and radially
Metaphyseal injuries may appear as mere buckling of the
cortexas angulated greenstick fractures or as complete
fractures with displacement and shortening.

Treatment
Physeal fractures are reduced, under anaesthesia, by pressure on the distal
fragment. The arm is immobilized in a full-length cast with the wrist slightly
flexed and ulnar deviated, and the elbow at 90 degrees (4 weeks).
Buckle fractures 2 weeks in plaster, followed by another 2 weeks of restricted
activity.
Greenstick fractures in children under 10, up to 30 degrees and in children over
10, up 15 degrees are accepted. If the deformity is greater, the fracture is reduced
by thumb pressure and the arm is immobilized in a full-length cast with the wrist
and forearm in neutral and the elbow flexed 90 degrees. The cast is changed and
the fracture re-x-rayed at 2 weeks; if it has redisplaced a further manipulation
can be carried out. The cast is finally discarded after 6 weeks.
Complete fractures. The fracture is manipulated in the same way as a Colles'
fracture; the reduction is checked by x-ray and a full-length cast is applied with
the wrist neutral and the forearm supinated. After 2 weeks, a check x-ray is
obtained; the cast is kept on for 6 weeks. If the fracture slips, especially if the
ulna is intact, it should be stabilized with a percutaneous K-wire.

Complications
EARLY
Forearm swelling and threatened compartment syndrome.
LATE
Malunion
Radio-ulnar discrepancy Premature fusion of the radial epiphysis
may result in bone length disparity and subluxation of the radio-
ulnar joint.

THANK YOU