



Injuries of the wrist and hand
By
Dr. AMMAR TALIB AL-YASSIRI

objectives
•
Radio-carpal fractures
•
Carpal bones fracture
•
Fractures of the bones of the hand

FRACTURED
RADIAL
STYLOID
•
Mechanism of injury: forced radial deviation of the
wrist
–
a fall
–
when a starting handle 'kicks back' - 'chauffeur's fracture'.
•
The fracture line is transverse, extending laterally from
the articular surface of the radius.
• Often undisplaced.
•
Treatment
–
If there is displacement it is reduced, and the wrist is held
in ulnar deviation by a plaster slab
–
if closed reduction is imperfect the fragment should be
screwed back, or held with K-wires.

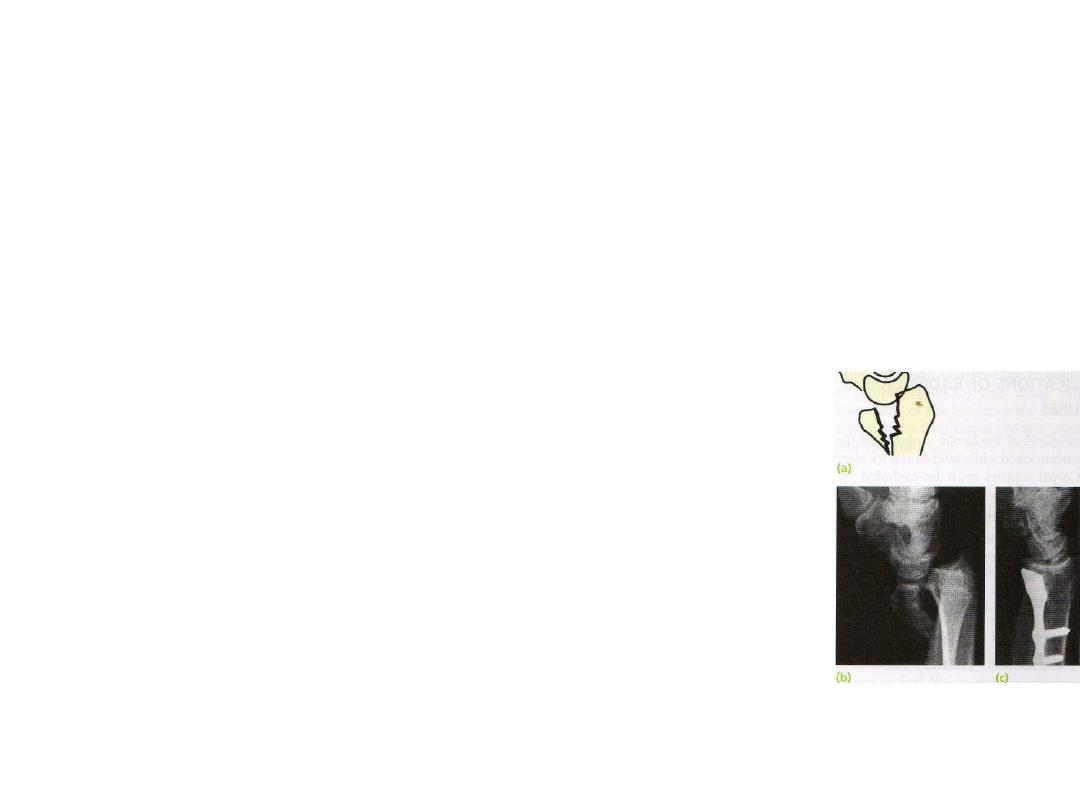
FRACTURE
-
SUBLUXATION
(
BARTON
'
S
FRACTURE
)
•
VOLAR SUBLUXATION
–
The true Barton's injury is a volar fracture of the distal
radius associated with volar subluxation of the carpus
–
the fracture line runs obliquely across
the volar lip of the radius into the wrist
joint; the distal fragment is displaced
anteriorly carrying the carpus with it
–
Inherently unstable
–
TREATMENT: Internal fixation, using a small
anterior buttress plate, is recommended

•
DORSAL SUBLUXATION
–
the line of fracture runs obliquely across the
dorsal lip of the radius and the carpus is carried
posteriorly
–
reduced closed and the forearm is immobilized in
a cast for 6 weeks If it re-displaces, closed K-wiring
or open reduction and plating is advisable.
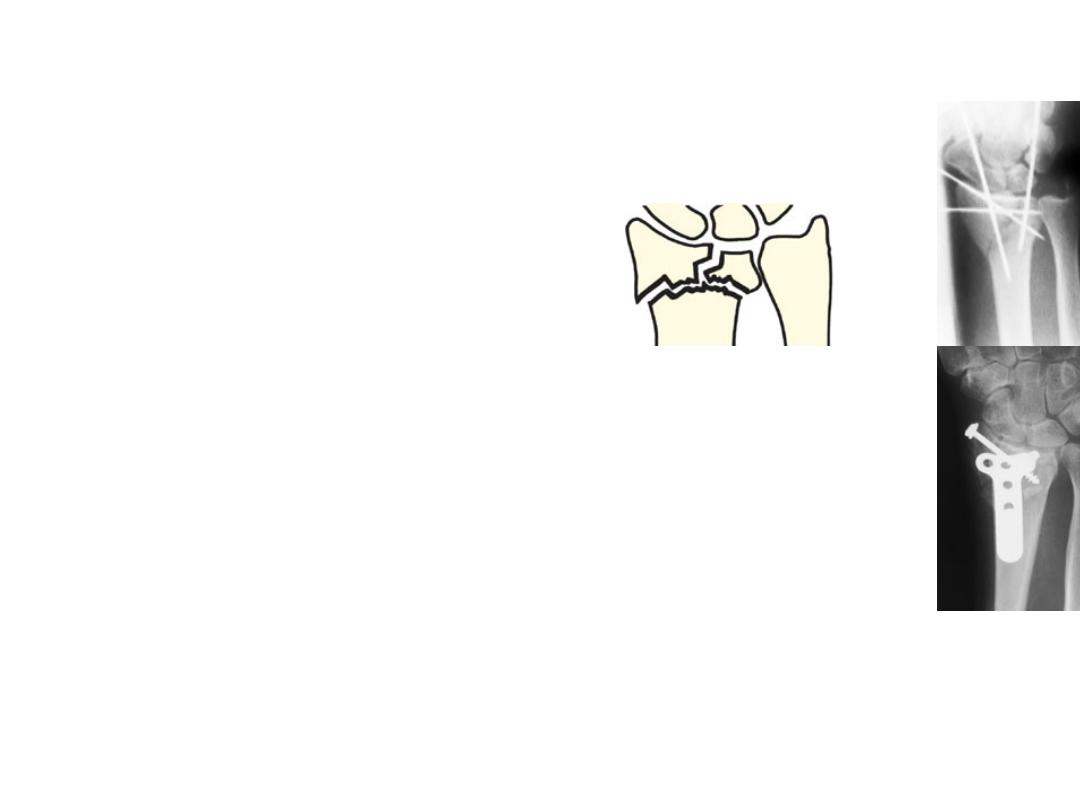
COMMINUTED INTRA-ARTICULAR
FRACTURES IN YOUNG ADULTS
•
a high energy injury
•
A poor outcome will result unless
–
intra-articular congruity,
–
fracture alignment
–
length are restored
–
and movements started as soon as possible.
•
posteroanterior and lateral x-rays, oblique views
•
CT scans are useful to show the fragment alignment.
•
Treatment:
–
manipulation and cast.
–
If the anatomy is not restored, then an open reduction
and a combination of wires, plates, screws and bone grafts
COMPLICATIONS OF RADIO-CARPAL
FRACTURES
•
Associated injuries of the carpus: Injuries of the carpus are
easily overlooked while attention is focussed on the radius.
•
Re-displacement : There is a strong tendency for Barton’s
fracture to re-displace if it is held in a cast;
•
Carpal instability: The patient may present years later with
chronic carpal instability.
•
Secondary osteoarthritis: Fractures into the joint and carpal
instability may eventually lead to secondary osteoarthritis.
Warning symptoms are
–
restricted wrist movement
–
loss of grip strength.
Treatment:
If pain and weakness interfere significantly with
function, arthrodesis of the wrist may be need.
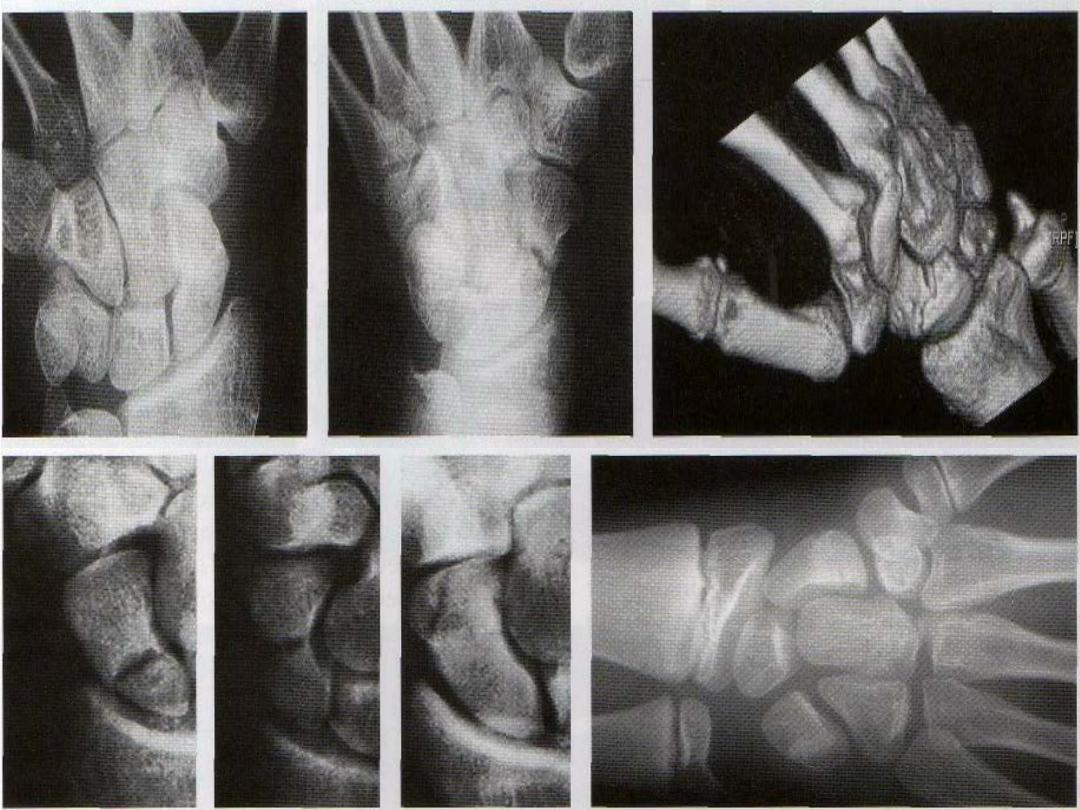
FRACTURED
SCAPHOID
•
75 % of all carpal fractures.
•
rare in the elderly and in children.
•
Mechanism of injury
–
combination of forced carpal movement and
compression,as in fall on the dorsifiexed hand
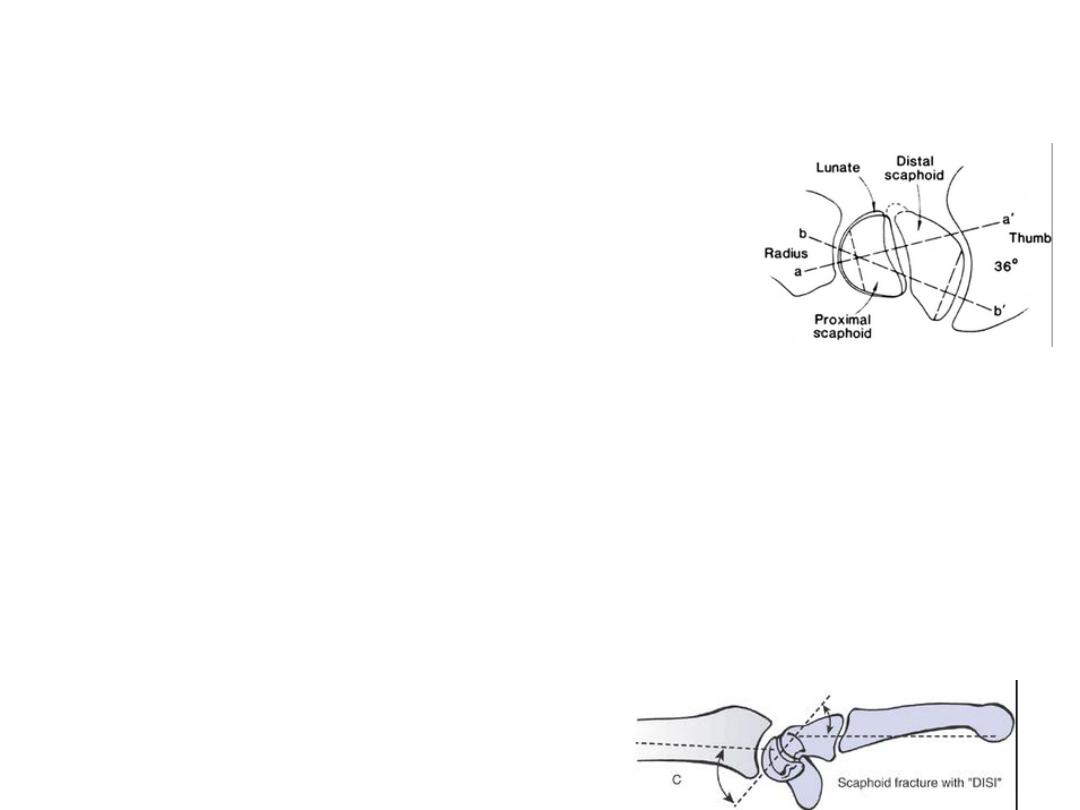
–
Most scaphoid fractures are stable with unstable fractures
the fragments may become displaced
–
The distal fragment, unrestrained by the scapho-lunate
ligament, flexes and the proximal fragment tilts dorsally
with the lunate
–
The blood supply of the scaphoid diminishes proximally

•
C/F:
–
fullness in the anatomical snuffbox;
–
precisely localized tenderness in the same place
–
Proximal pressure along the axis of the thumb may be painful.
•
X-ray
–
AP, lateral and oblique views are all essential
–
recent fracture shows only in the oblique view.
–
Usually the fracture line is transverse, and through the narrowest
part of the bone (waist)
–
proximal pole fracture.
–
Sometimes only the tubercle of the scaphoid is fractured.
–
subtle signs of displacement or instability
–
Signs of nonunion
–
sclerosis of the proximal fragment is pathognomonic of avascular
necrosis.
•
Treatment
–
Fracture of the scaphoid tubercle needs no splintage and should
be treated as a wrist sprain
–
Undisplaced fractures need no reduction and are treated in
plaster for 8 weeks
•
CT scan is the most reliable means of confirming union if in doubt
•
After 8 weeks the plaster is removed and the wrist examined clinically
and Radiologically
•
If there is no tenderness and the x-ray shows signs of healing, the
wrist is left free;
•
If the scaphoid is tender, or the fracture still visible on x-ray, the
cast is reapplied for a further 4 Weeks
•
Then either the fracture healed or
•
there is delayed union which hastened
internal fix + bone graft
–
Displaced fractures :ORIF comp.screw

•
Complications
–
Avascular necrosis: Bone grafting, as for delayed
union, may be successful,
–
Non-union: By 3 months it may be obvious that
the fracture will not unite. Bone grafting should be
attempted
–
Osteoarthritis Non-union or avascular necrosis
may lead to secondary osteoarthritis of the wrist
•
excising the radial styloid
•
proximal row carpectomy or four-corner fusion

LUNATE AND PERILUNATE
DISLOCATIONS
•
A fall with the hand forced into dorsiflexion may tear
the tough ligaments that normally bind the carpal
bones.
•
(perilunate dislocation).
•
(lunate dislocation).
•
(trans-scaphoid perilunate dislocation).
•
Clinical features
–
painful
–
swollen
–
Held immobile.
–
If the carpal tunnel is compressed
X-ray:
•
In the antero-posterior view
–
the carpus is diminished in height
–
bone shadows overlap abnormally.
–
One or more of the carpal bones may be fractured
–
If the lunate is dislocated, it has a characteristic triangular shape.
•
In the lateral view.
–
The dislocated lunate is tilted forwards and is displaced in front of the
radius, while the capitate and metacarpal bones are in line with the
radius.
–
With a perilunate dislocation the lunate is tilted only slightly and is not
displaced forwardsforwards, and the capitate and metacarpals lie
behind the line of the radius
–
if there is an associated scaphoid fracture, the distal fragment may be
flexed.

•
Treatment
–
Closed reduction
–
A plaster slab is applied holding the wrist neutral.
–
Percutaneous K-wires may be needed to hold the
reduction.
•
Open reduction: Reduction is imperative, and
if closed reduction fails open reduction is
performed.

Metacarpal fractures
•
Mechanism of injury: Blows, falls upon the
hand, or the longitudinal force of the boxer's
punch
•
the bones may fracture at their base, in the
shaft or through the neck
•
Angular deformity is usually not very marked,
and even if it persists, it does not interfere
much with function, Rotational deformity,
however, is serious

•
FRACTURES
OF
THE
METACARPAL
SHAFT
–
Mechanism of injury
•
A direct blow may fracture one or several metacarpal
shafts transversely.
•
A twisting or punching force may cause a spiral
fracture.
–
C/F: There is local pain and swelling, and
sometimes a dorsal 'hump'.

•
Treatment
–
Oblique or transverse fractures with slight displacement
require no reduction. Splintage also is unnecessary
–
Transverse fractures with considerable displacement are
reduced by traction and pressure
•
if stable held by a plaster slab extending from the
forearm over the fingers (only the damaged ones). The
slab is maintained for 3 weeks
•
these fractures are usually unstable and should be fixed
surgically
–
Spiral fractures are liable to rotate if so, they should be
perfectly reduced and fixed with lag screws and a plate, or
percutaneous wires.

•
FRACTURES
OF
THE
METACARPAL
NECK
–
A blow may fracture the metacarpal neck, usually
of the fifth finger (the 'boxer's fracture') and
occasionally one of the others
–
C/F: local swelling, with flattening of the knuckle.
–
X-rays show an impacted transverse fracture with
volar angulation of the distal fragment

–
Treatment
•
In the fifth and fourth fingers
–
a flexion deformity of up to 40 degrees can be accepted; as long
as there is no rotational deformity,
–
The hand is immobilized in a gutter splint with the MCP joint
flexed and (IP) joints straight until discomfort settles - a week or
two - and then the hand is mobilized
•
index and middle fingers, which function mainly in extension,
–
no more than 20 degrees of flexion at the fracture is acceptable.
–
reduced finger is held with a gutter splint moulded at three
points to support the fracture; the MCP joints are flexed and the
IP joints are straight
–
these fractures are usually fairly unstable because of the tone of
the flexor tendons and the palmar comminution of the fracture. If
there is a tendency to redisplacement, fixation should be used.

•
FRACTURES
OF
THE
METACARPAL
HEAD
–
These fractures occur after a direct blow.
–
They are often quite comminuted and sometimes
'open'.
–
Operative reduction is usually required and
fixation with small headless buried screws is ideal
–
joint is so badly damaged that primary
replacement is considered (Silastic, pyrocarbon or
polythene-metal).

•
FRACTURES
OF
THE
METACARPAL
BASE
–
these are usually stable injuries which can be treated
by ensuring that rotation is correct and then splinting
the digit in a volar slab extending from the forearm to
the proximal finger joint. The splint is retained for 3
weeks and exercises are then encouraged.
–
Displaced intra-articular fractures of the base of the
fourth or fifth metacarpal: reduced by traction on the
little finger and then held with a percutaneous K-wire
or compression screw.
•
FRACTURE
OF
THE
THUMB
METACARPAL
Three types of fracture are encountered:
•
impacted fracture of the metacarpal base;
•
Bennett's fracture-dislocation of the carpo-metacarpal
(CMC) joint; and
•
Rolando's comminuted fracture of the base.

•
Impacted fracture
–
A boxer may, while punching, sustain a fracture of the base of
the first metacarpal
–
Localized swelling and tenderness are found,
–
x-ray : a transverse fracture about 6 mm distal to the CMC joint,
with outward bowing and impaction.
–
Treatment If the angulation < 20-30 degrees a plaster of Paris
cast extending from the forearm to just short of the (IP)thumb
joint with the thumb fully abducted and extended. The cast is
removed after 2-3 weeks and the thumb is mobilized.
–
If the angulation >30 degrees, should be reduced then plaster
cast is applied. If the fracture is still unstable, then a
percutaneous K-wire is inserted or low profile plate

•
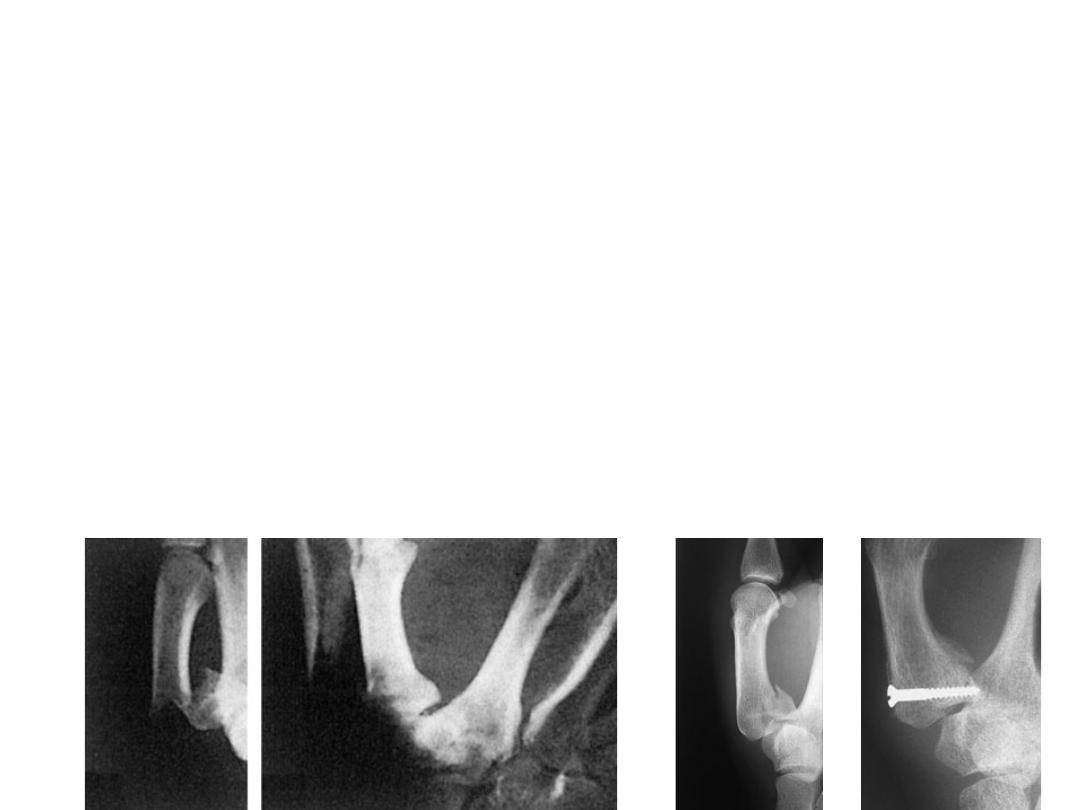
Bennett's fracture-dislocation
–
is commonly due to punching;
–
the fracture is oblique, extends into the CMC joint and is
unstable.
–
The thumb looks short and the carpo-metacarpal region
swollen.
–
X-rays show that a small triangular fragment has remained
in contact with the medial edge of the trapezium, while
the remainder of the thumb has subluxated proximally
–
Treatment :closed reduction+percut. Pinning or ORIF

•
ROLANDO'S FRACTURE
–
This is an intra-articular comminuted fracture of
the base of the first metacarpal with a T or Y
configuration.
–
Closed reduction and K-wiring or open reduction
and plate fixation can be used. With more severe
comminution, external fixation is needed

FRACTURES OF THE PHALANGES
FRACTURES OF THE PROXIMAL AND MIDDLE PHALANGEAL
SHAFTS
•
Transverse fracture of the shaft, often with forward
angulation.
•
Spiral fracture of the shaft, from a twisting injury.
•
Comminuted fracture, usually due to a crush injury and
often associated with significant tendon damage and skin
loss.
•
Avulsion of a small fragment of bone.
•
Metaphyseal fracture at the base of the proximal phalanx,
commonly seen in osteopaenic bone.
•
Intra-articular fractures: At the distal end of the phalanx,

Treatment
•
UNDISPLACED FRACTURES: ‘functional splintage’.
for 2–3 weeks
•
DISPLACED FRACTURES:
–
must be reduced and immobilized.
–
It is essential to check for rotational correction by
•
noting the convergent position of the finger when the MCP
joint is flexed,
•
seeing that the fingernails are all in the same plane.
•
Most need simple manipulation and can then be
held in a splint. If a reduction cannot be achieved,
or if it is unstable then surgery is needed.
FRACTURES OF THE TERMINAL
PHALANX
•
Fracture of the tuft
–
The tip of the finger may be struck by a hammer or caught in a door,
and the bone shattered.
–
The fracture is disregarded and treatment is focused on controlling
swelling and regaining movement.
–
The painful haematoma beneath the finger nail should be drained by
piercing the nail with a hot paper clip.
•
Mallet finger injury
–
After a sudden flexion injury (e.g. stubbing the tip of the finger) the
terminal phalanx droops and cannot be straightened actively.
–
Three types of injury are recognized:
•
avulsion of the most distal part of the extensor tendon;
•
avulsion of a small flake of bone from the base of the terminal phalanx; and
•
avulsion of a large dorsal bone fragment,
–
treatment: The TIP joint should be immobilized in slight
hyperextension,using a special mallet-finger splint

To take home massage
•
Carpal fractures and wrist injuries can be
missed in radiocarpal fractures
•
recent Scaphoid fracture shows only in the
oblique view
•
Minimize splintage to the least possible time
and limit it to the affected finger if this can be
allowed
•
Treatment is focused to the soft tissue as in
fracture tuft of the terminal phalanx

references
•
Apley system of orthopaedics and fractures
•
Campbell’s operative orthopaedics