RADIOLOGY
INTRODUCTION 2
PAGE 1
Radiological signs of lung disease
It is useful to place any pulmonary shadow into one or more of the following categories:-
Air – space filling (pulmonary edema, pulmonary consolidations).
Pulmonary collapse (atelectasis).
Spherical shadows.
Line shadows.
Widespread small shadow.
Replacement of air in the alveoli by fluid, which is either transudate (pulmonary oedema)
or exudate.
The causes of exudates include infection, infarction, contusion, hemorrhage,
immunological disorders (collagen vascular disease, extrinsic allergic alveolitis).
The sign of air space filling:
a. A shadow with ill –defined border (except when the opacity is in contact with a fissure).
b. An air bronchogram shows the presence of air in the bronchi.
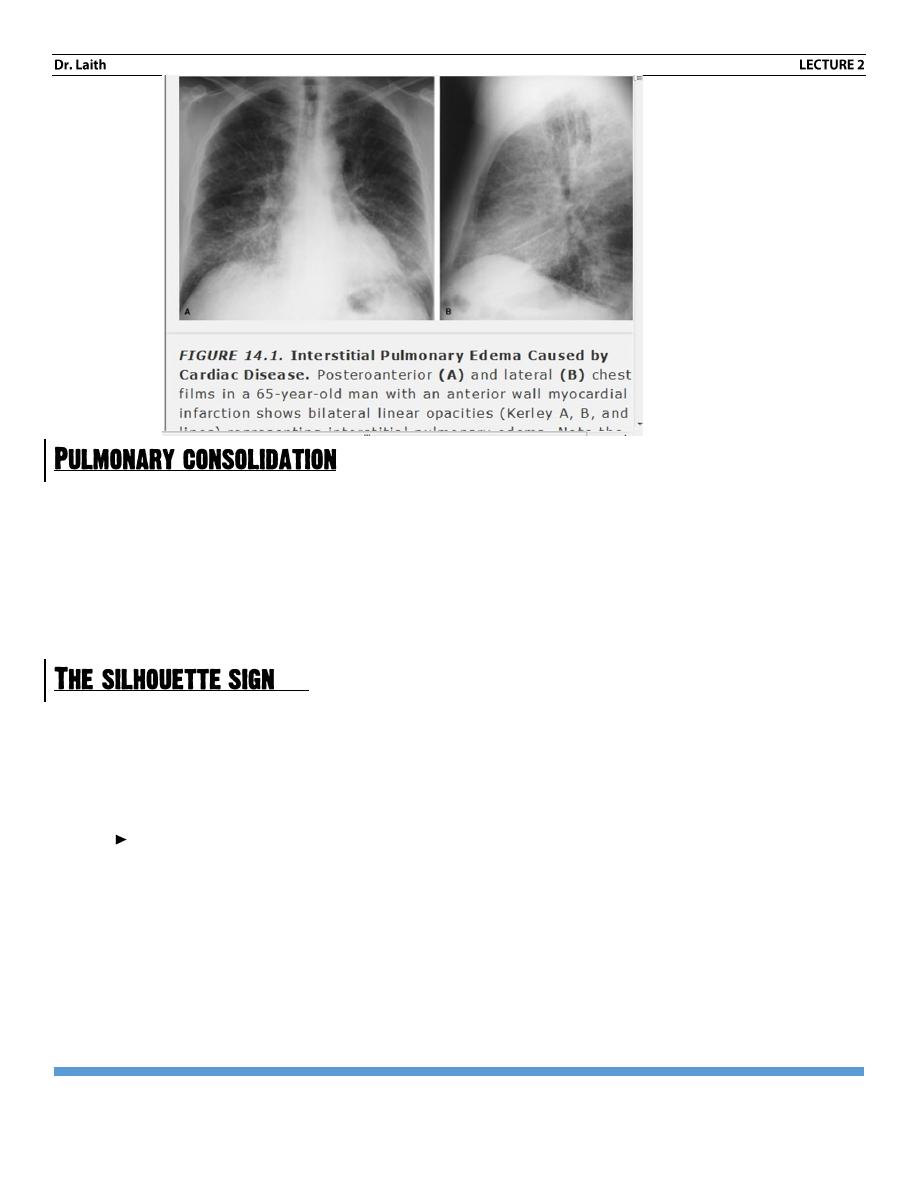
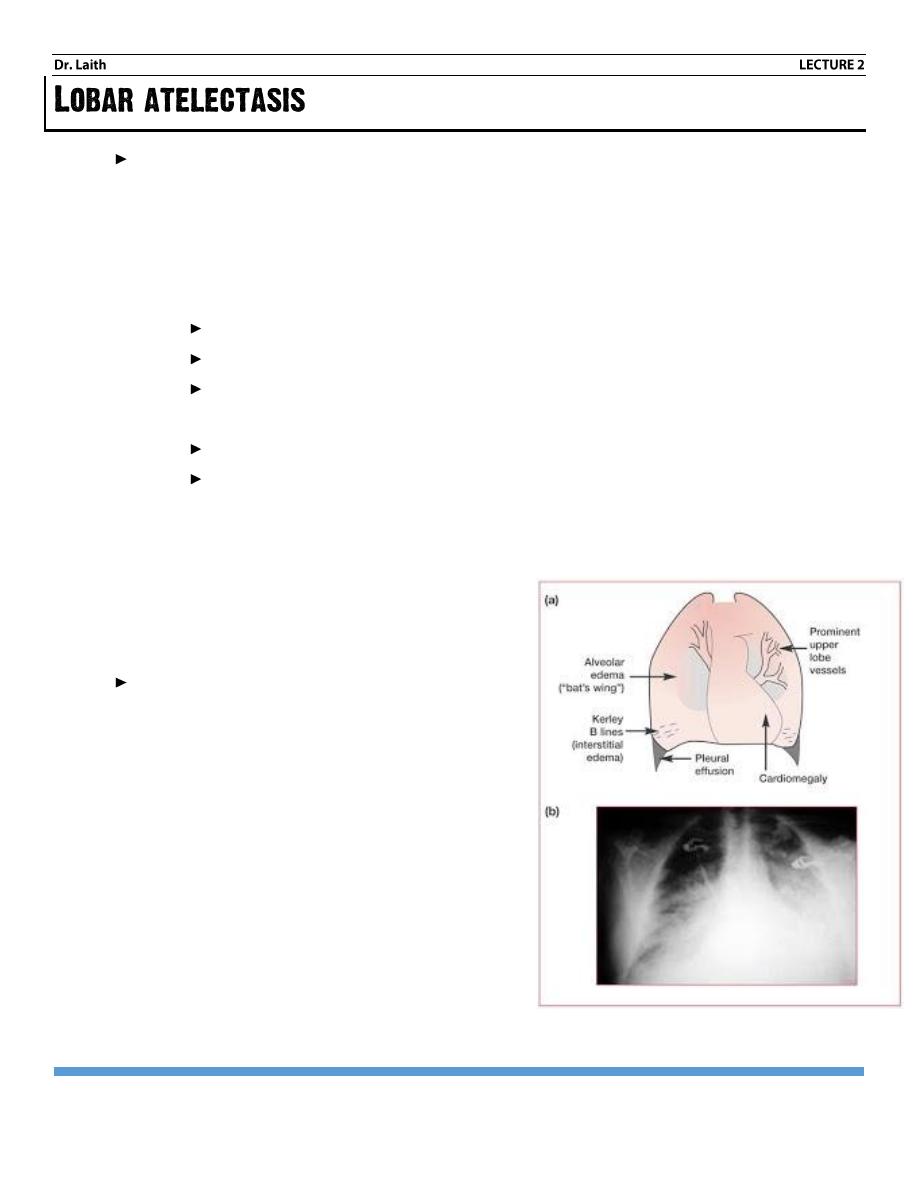
There are two radiographic pattern of pulmonary edema; alveolar and interstitial, since
edema initially collect in the interstitial tissue of lung. All patients with alveolar edema also
have intestinal edema. Alveolar edema is always acute, usually bilateral and involve all lobes
the shadow is more near the hila (bat wing appearance)
Interstitial edema cause thickening of the interstitial tissue of the lung. The hallmarks of it
are septal lines and thickening of pleural fissures.
Causes of pulmonary edema
Pulmonary edema is either:
a. Cardiogenic e.g. LVF (*Left Ventricular Failure).
b. Non – cardiogenic e.g. ARDS (acute respiratory distress syndrome), aspiration of
gastric contents or inhalation of noxious gases.
RADIOLOGY
INTRODUCTION 2
PAGE 2
1- Lobar consolidation is diagnostic of bacterial pneumonia.
2- Patchy consolidation either one or more patches of ill-defined shadow may be due to
pneumonia, infarction, contusion or immunological disease.
3- Cavitation (abscess formation) may occur with bacterial or fungal infection, also with
infarction, Wegener's granulomatosis.
An intra-thoracic lesion touching the border of the heart, aorta or diaphragm, obliteration of
that border on chest x-ray, this is the silhouette sign and it has 2 important application:
1-
Help localize a shadow: - e.g. loss of heart border, indicate that the lesion is in the
anterior half of chest.
Loss of part of the diaphragm means the disease is in the pleura or in direct contact
with the diaphragm (usually lower lobe).
2-
Sometimes it help to diagnose pulmonary consolidation or collapse even when the
presence of opacity uncertain (by decrement in the sharpness of the outline of the
mediastinum or heart by this lesion).
RADIOLOGY
INTRODUCTION 2
PAGE 3
Pulmonary collapse (atelectasis): loss of volume of a lobe or entire lung.
Causes are
I.
Bronchial obstruction.
II.
Pneumothorax or pleural effusion.
Causes of bronchial obstruction
a. Bronchial wall lesion.
Primary CA.
Other bronchial tumor e.g. carcinoid.
Endo – bronchial TB.
b. Intraluminal occlusion.
Mucous plugging.
Foreign body.
c. Adjacent mass (malignant tumor, Lymphadenopathy).
The signs of collapse
1- Shadow of collapse lung (increased opacity).
2- Displacement of structure.
3- Silhouette sign (help to localize the collapsed
lobe).
With collapse of the whole of one lung, the
entire hemithorax is opaque and there is
substantial mediastinal and tracheal shift.
صورة خارج النص توضح
BATWING SIGN + KERLEY B LINES
RADIOLOGY
INTRODUCTION 2
PAGE 4
(pulmonary nodule, coin lesion)
Usual causes
1- Tumor
Bronchial carcinoma.
Bronchial carcinoid.
Benign tumor (hamartoma).
Secondary metastasis.
2- Infection
Hydatid cyst.
Abscess.
Round pneumonia.
3- Granuloma TB, sarcoidosis.
4- Extra- pulmonary causes:
Pleural tumor.
Encysted pleural effusion
1-
Compare with previous film:
Fast rate of growth indicate malignancy.
Failure to grow over a period of 18 months indicate benign tumor or inactive
granuloma.
2-
Calcification: if substantial virtually excludes malignancy.
3-
Margin: primary Centers are nearly always rounded with lobulated, notched or
infiltrating outline.
On the contrary, if the shadow is perfectly spherical and the edge very well defined
this indicates benign tumor, hydatid cyst, metastases or granuloma (Tuberculoma).
4-
Involvement of adjacent chest will: destruction of adjacent ribs is virtually diagnostic
of invasion by cancer (especially with pancost tumor, which involves the lung apex and
invade adjacent bones).
5-
Cavitation caused by:
Lung abscess.
RADIOLOGY
INTRODUCTION 2
PAGE 5
Primary cancer.
Secondary cancer.
Differential diagnosis between lung abscess and tumor May be difficult but any
irregularity of inner outer walls
makes the diagnosis of cancer highly likely.
6-
Size: - a solitary mass larger than 4 cm with no calcification is primary CA, lung abscess,
or spherical pneumonia.
7-
Other lesions (multiple nodules, either metastasis, multiple abscesses, granuloma,
collagen vascular disease, multiple hydatid cyst).
1. The only normal lines shadows within are the lung fissures and walls of the large bronchi.
2. The transverse fissure is seen on PA view, and the oblique fissure on lateral view.
Septal lines
: are connective tissue planes contain lymph vessels they become visible on
chest x –ray only when they are thickened.
They are of two types:-
Kerley A lines
: which radiate towards the hila in the mind and upper zones.
They are much thinner than adjacent blood vessel and they do not reach the lung edge.
Kerley B lines
: they are more common than kerley A. lines.
They are horizontal lines more than 2 cm in length best seen at the periphery of the lungs
and often reach the edge of the lunge (unlike blood vessel).
Important causes of septal lines:
1. Pulmonary edema.
2. Lymphangitis carcinomatosa.
Pleuropulmonary scars
due to infection for infarction they are of no clinical significance.
Linear atelectasis
: which is due to hypoventilation (and not bronchial obstruction) it is
usually post-operative.
Emphysematous bullae
: bullae more often rounded and traversed by thin line shadow and
they have few if any normal blood vessels can be seen beyond the pleural line.
RADIOLOGY
INTRODUCTION 2
PAGE 6
The pleural edge in pneumothorax
This is seen as a line approximately parallel with chest wall no lung vessels can be seen
beyond the pleural edge.
Nodular and reticular shadow
: wide either spread small (2-3 mm) pulmonary shadows, small
round shadows (nodular) or net like pattern of small lines (reticular) or the combination of both
(reticulonodular) shadow. With this category, correlation with the clinical picture is very
important because there is a long list of differential diagnosis for these appearances.
Important questions to answer when reticulonodular shadow is present
1- Radiographic pattern (reticular, nodular, or reticulonodular).
2- Distribution: uniform or more severe in one or other zone and whether it is central or
peripheral)
3- Are there other abnormalities?
HRCT (high resolution CT scan) is of great help when one is in doubt whether diffuse lung
disease is present.
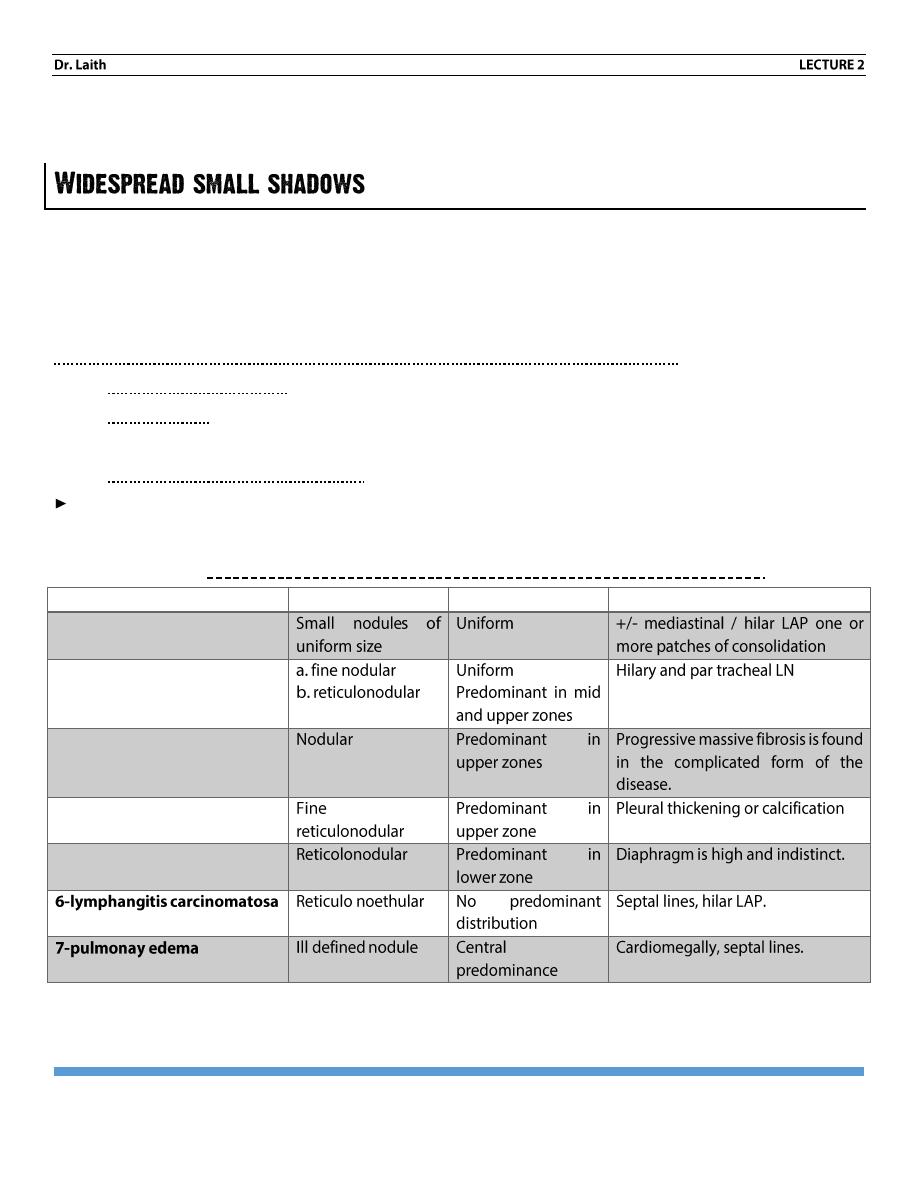
Common causes of reticular and nodular shadowing
Diagnosis
Pattern
Distribution
Other features
1. miliary TB
2. Sarcoidosis
3. coalminer’s
pneumoconiosis
4. asbestosis
5. fibrosing alveolitis
RADIOLOGY
INTRODUCTION 2
PAGE 7
Multiple ring shadow
of > 1 cm are diagnostic of bronchiectasis they represent dilated thick
walled bronchi.
Wide spread small pulmonary calcification
: may occur following pulmonary infection with
TB histoplasmosis or chicken pox.
Diaphragm outlines should be clear.
Right dome is lighter higher than left one not more than 2.5 com.
The Right is occupied by diaphragmatic hernia and congenital cyst, while the left is by pad
of fats.
Elevated left diaphragm could be due to
Lung: - splinting diaphragm (fibrosis), collapse, pneumonectomy.
Diaphragm congenital eventration, paralysis (due to phrenic nerve tumor or damage).
Below the diaphragm: splenomegaly, abscess …etc.
Elevated Right diaphragm
Due to lung causes, eventration never occur.
Bilateral elevation.
Bilateral elevation– due to increased intra-abdominal pressure (like ascites tumor,
pregnancy – etc.).
Bilateral depression…. Like asthma, emphysema.
In the lower angle, we look for mass, pleural effusion etc.
Hilar shadow
C shaped represent pulmonary arteries and veins. It should be-
Equal in size and density on both sides.
Left Hilum is higher than right Hilum due to over –crossing of left pulmonary artery
(superior and posterior) on the left main bronchus while on the right side the pulmonary
artery pass anterior to the right main bronchus.
Normal lymph nodes are not detected but when lymph nodes are enlarged, they will be
seen as hilar mass.
RADIOLOGY
INTRODUCTION 2
PAGE 8
Abnormality affecting it
1- Pulmonary hypertension.
2- Post-stenotic arterial dilation.
3- Pulmonary artery aneurism.
4- Arterial atresia.
5- Lymphadenopathy.
6- Bronchogenic carcinoma.
Compare two sides of the lung.
Each lung is divided in to 3 zones.
: is the (anterior 2 ribs), diseases affecting it mainly
1- TB.
2- Pancost tumor: it presents at the Rt upper apex and associated with rib erosion
(missing) use MRI for diagnosis of neural canal and nerve involvement.
3- Pneumothorax (Hair line)
4- Loculated phenral effutan.
: between 2
nd
and 4
th
anterior ribs
: below 4
th
anterior rib
أنتهى الصراع مع املحاضرة اىل هنا
MLJ
Mustafa Jasim