RADIOLOGY
INTRODUCTION
PAGE 1
Introduction to chest radiology
Investigation
a- Patients complain with normal x ray.
b- Early asthma
c- Early bronchiectasis
d- bronchitis
e- Early interstitial lung disease.
f- Early secondary metastases …
g- Early staging of malignancy.
h- Collapse of lung tube.
i- For hilar abnormality.
a. Hilar mass to differentiate between lymph glands and blood vessels (lymph glands
appear moderate density while B.V. appear black).
b. Vascular lesions (like bronchogenic carcinoma).
c. Staging of malignancy (like bronchogenic carcinoma).
It has a limited role see the objects in the chest wall or very close to be because air in the lung
prevent U/S from penetrating it, so we see:
a- Hydatid cyst
b- Lesion of pleura (no air between it).
c- Emphysema.
totally replaced by CT and MRI.
inject a contrast material into the nose to the trachea (to make it visible),
CT. replaces it.
RADIOLOGY
INTRODUCTION
PAGE 2
It is the first investigation to be done to the patient.
Used in
a- Pre-operative.
b- Pre-employment.
c- Patients complain from respiratory symptom.
d- Patient complains from cardio vascular symptom.
Views of x-ray
PosteroAnterior PA view.
Lateral view and lateral decubitus (in which the patient put on the suspected side
and x –ray is taken (such as in pleural of effusion).
Thoracic inlet view to see hilar shadows, cardiophrenic angle shadow and right
middle lobe collapse.
Lordotic view.
Routine examination include P.A and lateral view other supplementary views are done
according to the case, so all patients admitted to hospital should have PA X ray in standing
erect view in complete inspiration.
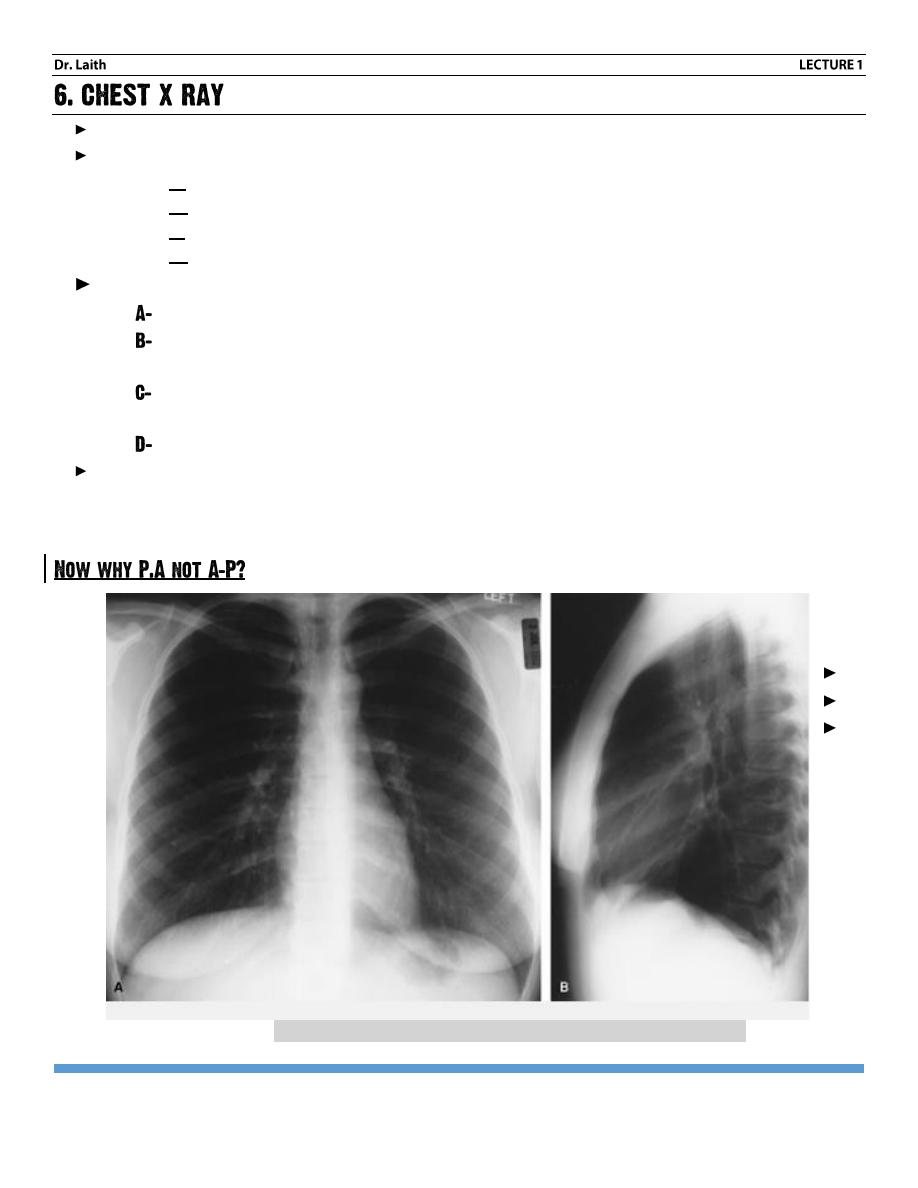
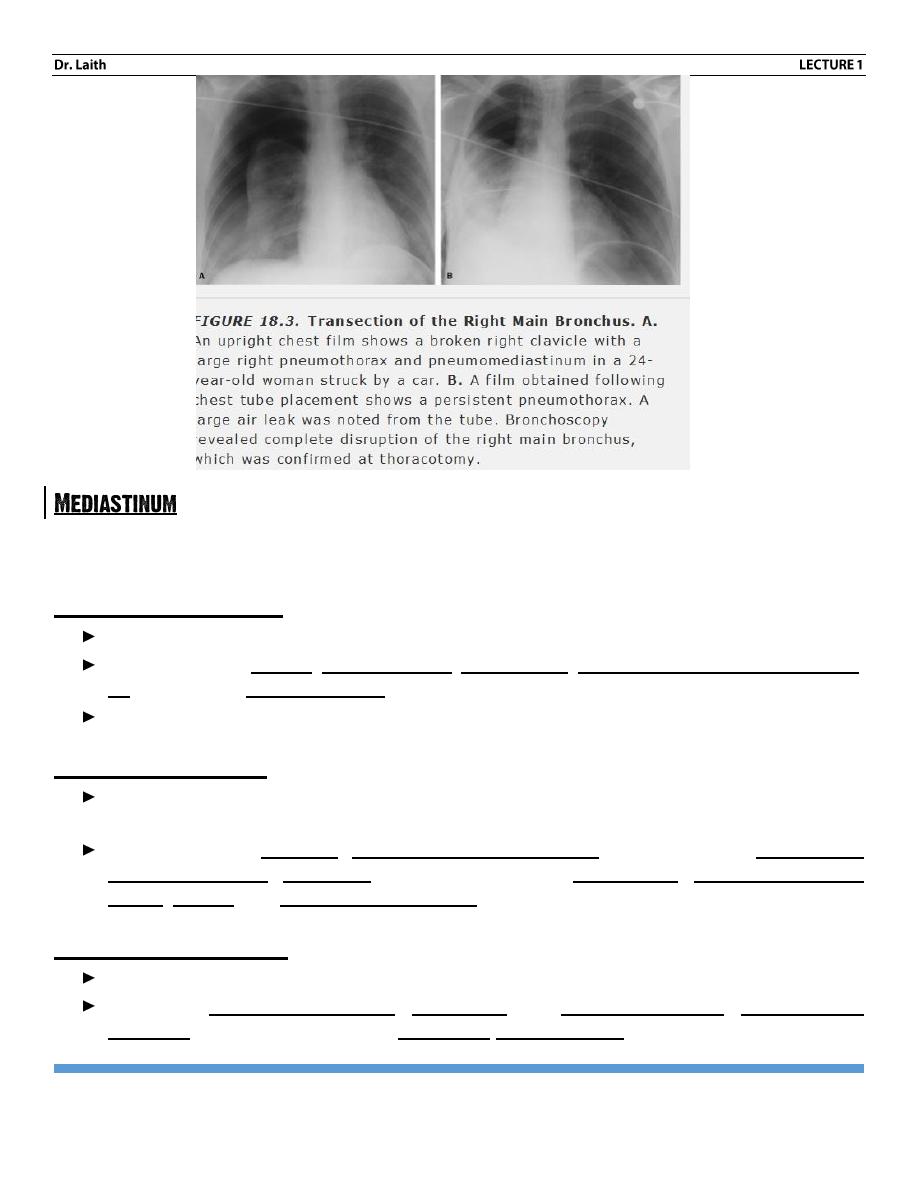
Normal PA (A) and LATERAL (B) chest x ray views
RADIOLOGY
INTRODUCTION
PAGE 3
Most CXR one taken in PA position, that is the patient stand in front of the X ray film
cassette with their chest against the cassette and their back to the radiographer the
X ray beam passes through the patient back to front (i.e. PA) on to the films. The
heart and mediastinum are thus closest to the film and therefore not magnified.
When an x –ray a taken in an (AP) position, such us when the patient is unwell in
bed, the heart and mediastinum are distant from the cassette and are therefore
subject to X-ray magnification. As a result, it is very difficult to make an accurate
assessment of the cardio mediastinal contour on an AP film.
In lateral X ray
1- Check two spaces: the anterior (retrosternal) space, and the posterior (retro cardiac) space.
They should be of equal density.
2- The vertebral bodies are more translucent as we go downwards.
3- Check the two hemi-diaphragm.
Assessment of adequacy of in inspiratory effort
The difference in inspiration and expiration views: - There would be opacities in lung during
expiration, should not be considered as disease, but rather normal during expiration.
How to know it is full inspiration
The Right dome of the diaphragm should reach the anterior 6
th
rib in full inspiration. In another
world, the adequacy of inspiration is ascertained by counting either the number of visible
anterior and posterior ribs: (if six complete anterior or ten posterior ribs are visible then the
patient has taken and adequate inspiratory effort).
How to know the patient is not rotated and in exact right posture (erect posture)?
The spinous processes of dorsal vertebrae should be aligned together same level with
medial end of the clavicle symmetrically if this is not the case then the patient is rotated
either to the right or to the left.
If there is rotation, the side to which patient rotated is assessed by comparing the densities
of two hemi thoraces.
The increase in blackness of one hemi-thorax is always on the side to which the patient
rotated, irrespective of whether the CXR had been taken anteroposterior or posteroanterior.
RADIOLOGY
INTRODUCTION
PAGE 4
Note:-
Exposure amount of x-ray is > in obese person from thin on.
Certain markers should be written on x-ray including for example (dextro-cardiac patient,
side and date important to compare recent with old one).
We have tube (from which x –ray is produced) and local film. The distance between them
is constant (180 cm) and we have two factors KV = 70 kilovolt, in 70 kg body weight and MAS
=50 kilo for 70 kg body wt. increase or decrease in association with weight.
Now for chest x-ray we took for the following (from outer to inner side).
1- Soft tissue.
Includes skin, subcutaneous tissue, breast, thyroid, supraclavicular and axillary area, so
look for a calcification, air (surgical emphysema) tumor and mastectomy, etc.
2- Bony structures.
This include ribs, clavicle, scapula, and spines (thoracic range).So we look for
Increase bone density: like paget is disease, congenital osteopetrosis (marble bone disease).
myelosclerois (secondary to carcinoma of pro state
Decrease bone density: like osteoporosis, osteomalacia …etc.
Multiple facture.
Other system disease affecting the bone disease like thalassemia (long bone bulging and
course trabeculation)
Multiple metastasis (multiple osteolytic lesions).
3- Trachea.
Normally it is transparent line in the middle slightly deviated to the Right, so we look
for:
Deviation to the same side
a- Collapse.
b- Upper lobe fibrosis.
c- Pneumonectomy.
Deviation to the opposite side
a- Tension pneumothorax
b- Massive pleural effusion.
Deviation due to mediastinal mass (retrosternal goiter)
Tracheostomy tube.
Intra-tracheal tumor.
RADIOLOGY
INTRODUCTION
PAGE 5
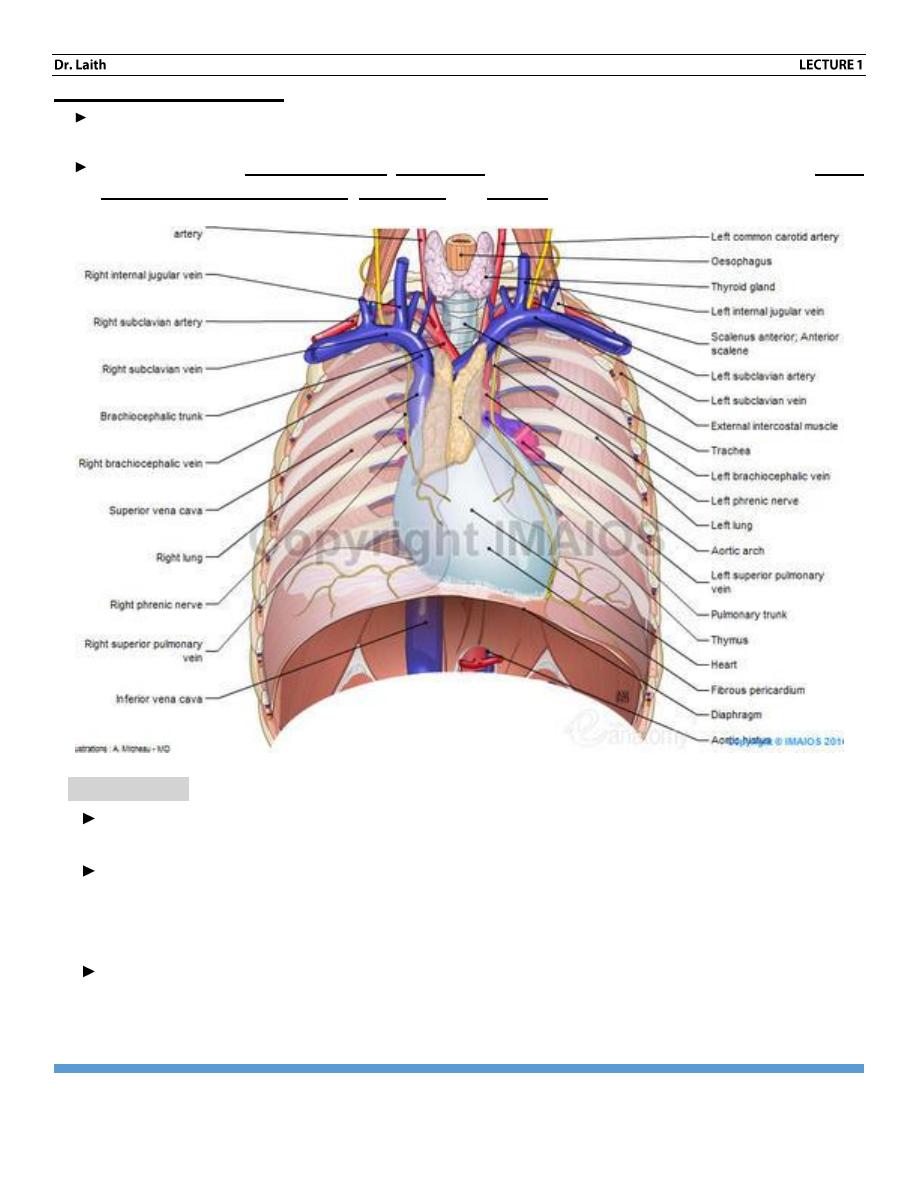
Extending from upper part where the great vessels, till lower part of the heart. Knowledge of the
mediastinal content can aid in your differential diagnosis.
Anterior mediastinum
Borders: The sternum anteriorly, and ventral cardiac surface posteriorly.
Content include thymus, ascending aorta, lymph nodes, internal mammary artery and vein,
fat and adjacent boney structures (ribs + sternum )
So look for LAP, congenital tumors, dermoid, lipoma, liposarcoma.
Middle mediastinum
Borders: the anterior mediastinal compartment anteriorly, and anterior Surface of the spine
posteriorly.
Content include the heart, proximal pulmonary arteries and veins (hila) superior and
interior vena cava, esophagus (usually not visible), vagus nerve, Recurrant laryngeal
nerves, trachea, and proximal bronchial tree.
Posterior mediastinum
Borders: the anterior surface of spine posteriorly to the ribs.
Content: the descending aorta, the azygos and hemi-azygos veins, adjacent bony
structures (the spine and ribs) and spinal cord with nerve root.
RADIOLOGY
INTRODUCTION
PAGE 6
Superior mediastinum
Borders: The lower border is a horizontal line drawn from the angle of Louis posteriorly to
the spine.
Content include the thyroid gland, aortic arch and great vessels, proximal portions of vagus
and recurrent laryngeal nerve, esophagus and trachea.
4- The heart:
The transverse diameter of the heart should be < 50% of the internal thoracic diameter
(thoracic outlet at left most and right most – if it is more than 50% then it is enlarged heart).
The right heart border is occupied by the right atrium. The left superior border is occupied
by aortic knuckle, pulmonary artery, and left aortic auricle, the left inferior border is
occupied by left ventricle (LV). While the inferior border and anteriorly occupied by right
ventricle, and part of left ventricle.
Right enlargement it causes.
1- Increase in curvature of left heart border (goes laterally)
2- Enlargement of SVC.
RADIOLOGY
INTRODUCTION
PAGE 7
Left enlargement
It has 3 stages:-
1- Straightening of cardiac border.
2- Bulging of left auricle below the main pulmonary art.
3- Double line of right cardiac border (double contour)
In massive enlargement, the left main bronchus is pushed upward. The posterior margin of left
atrium is best evaluated on lateral View.
RV enlargements: its causes:-
1- Elevation of cardiac apex of diaphragm
2- Anterior enlargement on lateral view lead to loss of retrosternal air space
3- Increase contact of RV against the sternum.
4-
LV enlargement: - it causes-
1. Displacement of cardiac apex inferiorly and posteriorly.
2. Increase out word lower bulge.
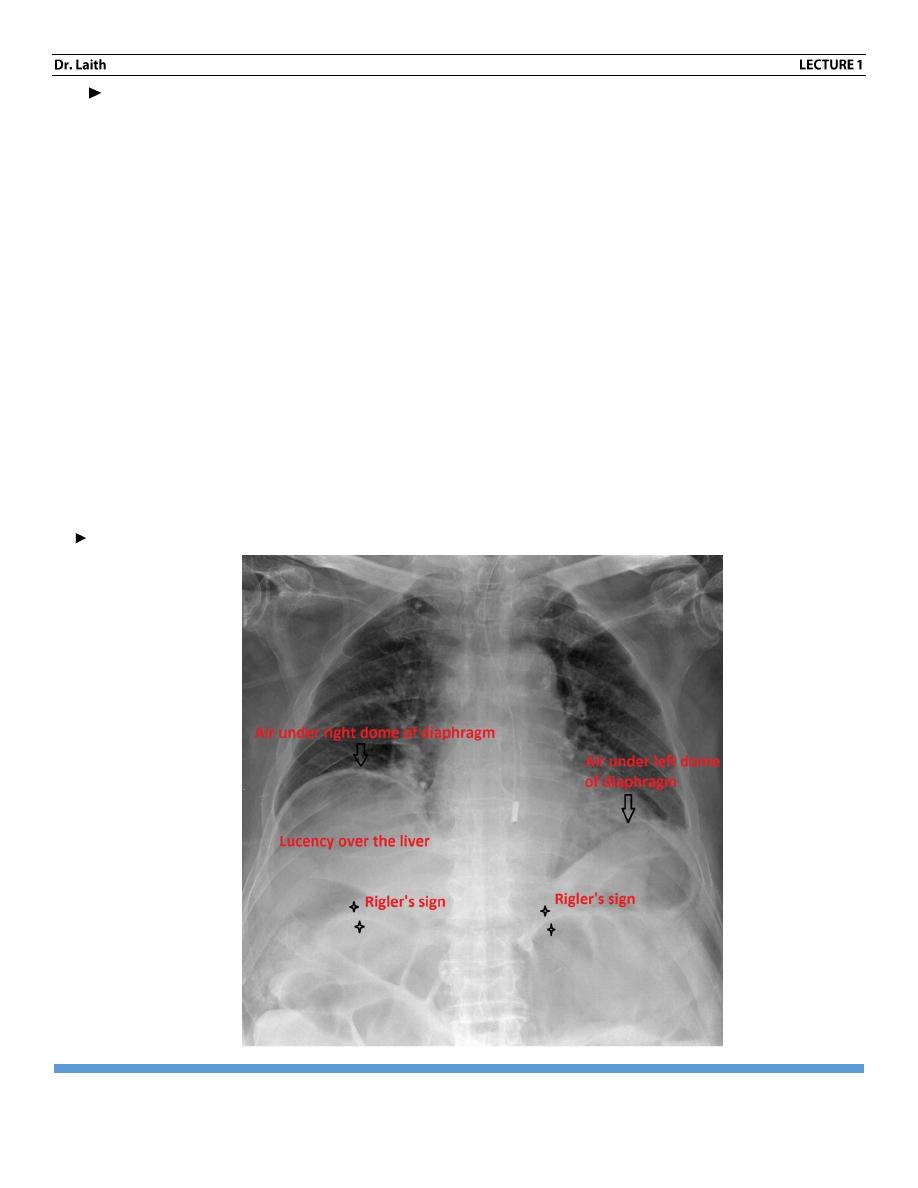
3. On lateral film, from junction of IVC and heart at the level of diaphragm measure 1.8
cm posteriorly and 1.8 com superiorly.
If cardiac shadow extend beyond this
<<<
LV enlargement (Rigler’s sign).
RADIOLOGY
INTRODUCTION
PAGE 8
Left atrial enlargement
1- Mitral stenosis.
2- Left atrial tumor example: myxoma.
3- Mitral incompetence.
Right atrial enlargement
1- Right ventricular failure.
2- Tricuspid stenosis
3- Tricuspid incompetence
Left ventricular enlargement
1- Aortic and mitral incompetence.
2- Aortic stenosis and systemic hypertension only after left ventricular decompensation
has occurred.
3- Ischemic heart disease and cardiomyopathy of many types, once substantial muscle
damage has occurred.
4- Patent ductus arteriosus and ventricular septal defect in cases with large left to right
shunt.
Right ventricular enlargement:-
1- Atrial septal defect.
2- Tricuspid stenosis and pulmonary hypertension only after right ventricular
decompensation has occurred.
5- The diaphragm:
Diaphragm outlines should be clear.
Right dome is lighter higher than left one not more than 2.5 com.
The Right is occupied by diaphragmatic hernia and congenital cyst, while the left is by
pad of fats.
Elevated left Diaphragm could be due to
Lung: - splinting diaphragm (fibrosis), collapse, pneumonectomy.
Diaphragm congenital eventration, paralysis (due to phrenic nerve tumor or damage).
Below the diaphragm: splenomegaly, abscess …etc.
RADIOLOGY
INTRODUCTION
PAGE 9
Elevated Right diaphragm
Due to lung causes, eventration never occur.
Bilateral elevation.
Bilateral elevation– due to ↑intra-abdominal pressure (like ascites tumor, pregnancy –
etc).
Bilateral depression…. Like asthma, emphysema.
In the lower angle we look for mass, pleural effusion etc.
6- Hilar shadow:-
c- Shaped represent pulmonary arteries and veins. It should be-
Equal in size and density on both sides.
Left Hilum is higher than right Hilum due to over-crossing of left pulmonary artery
(superior and posterior) on the left main bronchus while on the right side the pulmonary
artery pass anterior to the right main bronchus.
Normal lymph nodes are not detected but when lymph nodes are enlarged, they will be
seen as hilar mass
Abnormality affecting it:-
1. Pulmonary hypertension.
2. Post-stenotic arterial dilation
3. Pulmonary artery aneurism.
4. Arterial atresia.
5. Lymphadenopathy LAP.
6. Bronchogenic carcinoma.
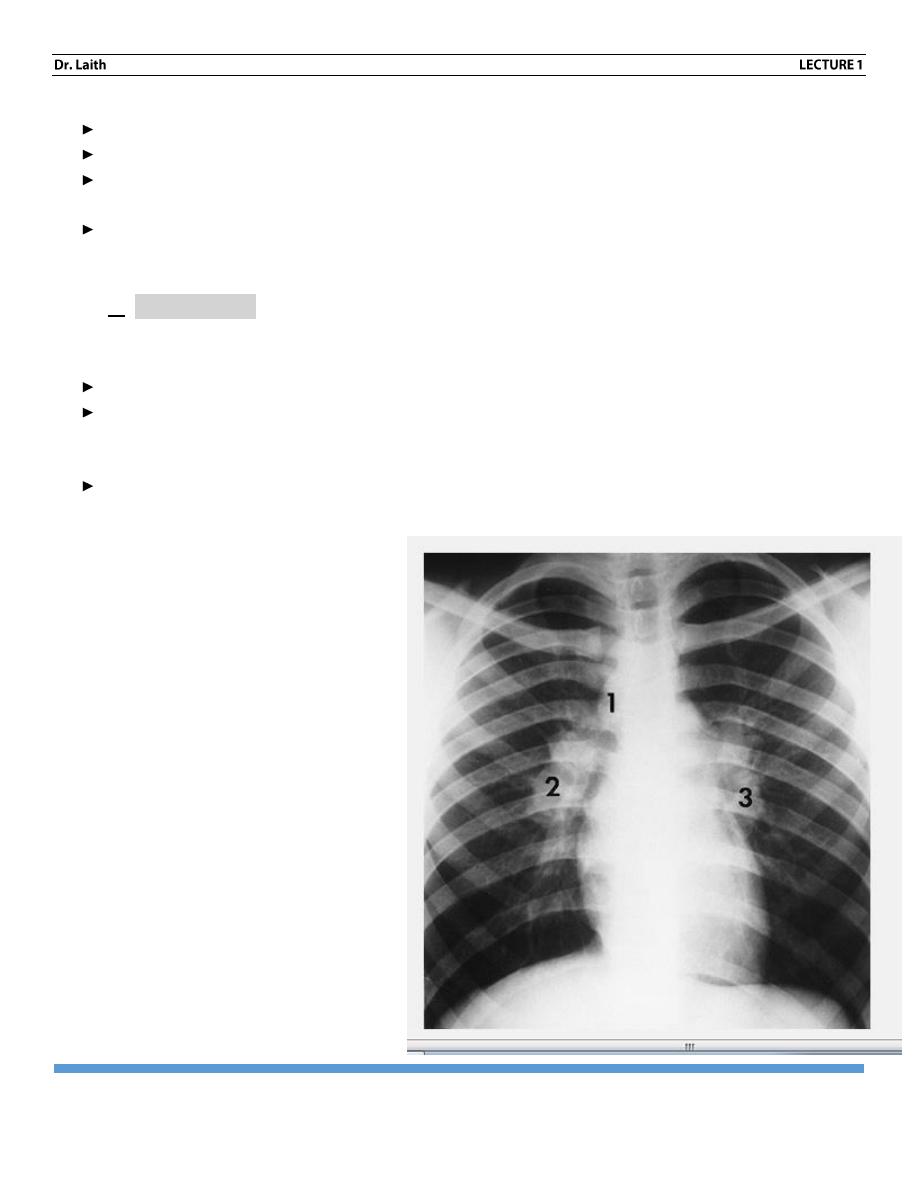
Hilar LAP
1. 1 para-tracheal
2. 2 Right hilar
3. 3 Left hilar LNs