Eruption of teeth
Lec: 2Eruption
Is the movement which takes a tooth from its developmental position(in the alveolar bone) to the oral cavity until it reaches the occlusion with its antagonist dentition.
Phases of tooth eruption:
Pre eruptive tooth phase: made by the deciduous and permanent tooth germs within tissues of the jaw before they begin to erupt.
Eruptive phase: starts with initiation of root formation and made by teeth to move from its position within bone of the jaw to its functional position in occlusion. Has an intraosseous and extraosseous components.
Post eruptive phase: takes place after the teeth are functioning to maintain the position of the erupted tooth in occlusion while the jaws are continuing to grow and compensate for occlusal and proximal tooth wear.
Dentition:
There are two sets of dentition in humans: Primary vs Permanent dentition
Mixed dentition: presence of two dentition
Teeth in primary dentition are smaller and fewer in number than permanent dentition to conform to the smaller jaw size
Primary dentition: ~ 2 to 6 years of age.
Mixed dentition: ~ 6 to 12 years.
Permanent dentition: > 12 years.
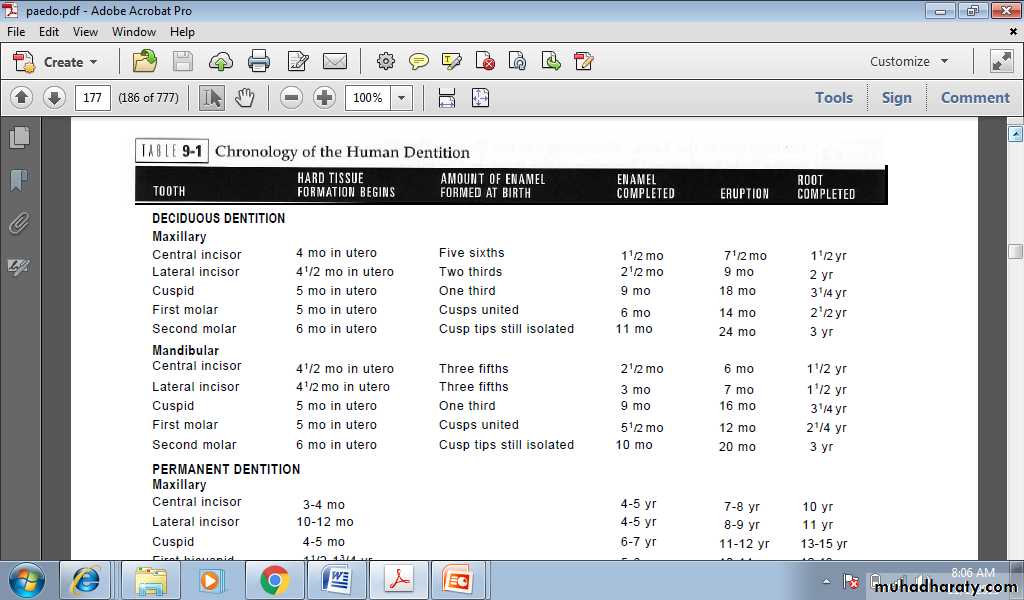
Chronology of human primary dentition
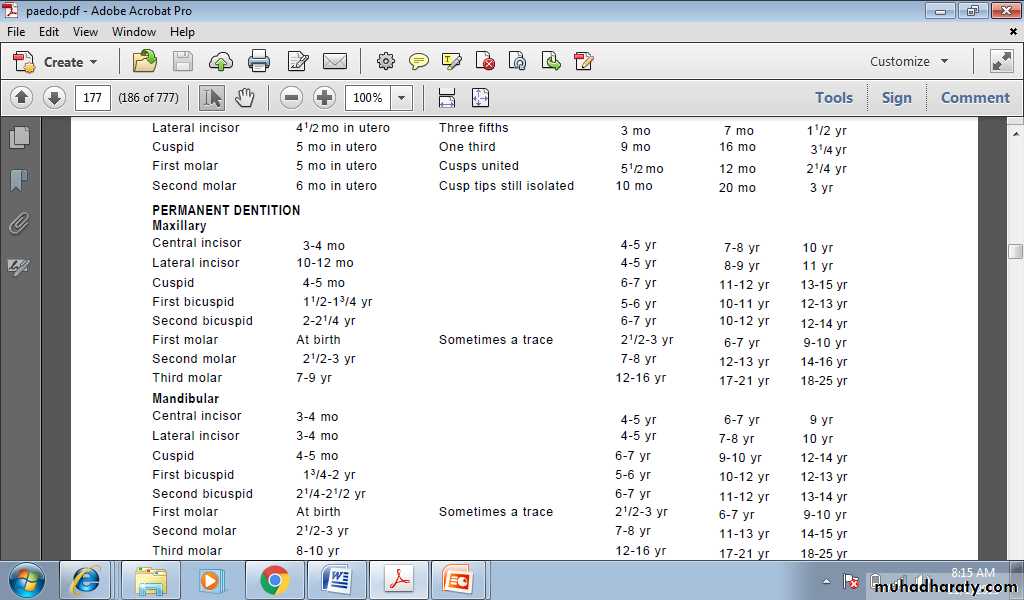
Chronology of human permanent dentition
Variation in the sequence of eruption
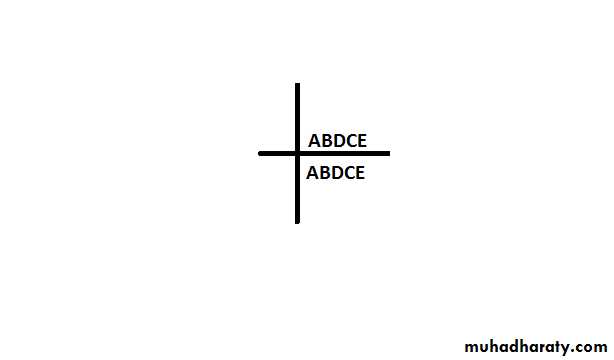
Sequence of eruption of primary dentition
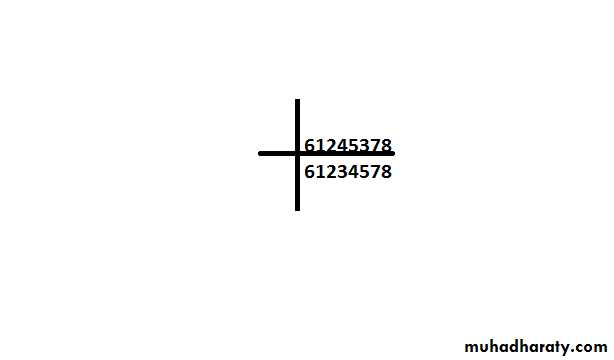
Sequence of eruption of permanent dentition
Influence of premature loss of primary molars on eruption time of their successors
Eruption of the premolar teeth is delayed in children who lose primary molars at 4 or 5 years of age and before.
If extraction of the primary molars occurs after the age of 5 years, there is a decrease in the delay of premolar eruption.
At 8, 9, and 10 years of age, premolar eruption resulting from premature loss of primary teeth is greatly accelerated.
Lingual eruption of mandibular central incisor
It is often a source of concern for parents when they discover a double row of teeth for their child. The primary teeth may have undergone extensive root resorption and may be held only by soft tissues. In other instances the roots may not have undergone normal resorption and the teeth remain solidly in place. It is common for mandibular permanent incisors to erupt lingually, and this pattern should be considered essentially normal. It is seen both in patients with an obvious arch length inadequacy. and in those with a desirable amount of spacing of the primary incisors. In either case the tongue and continued alveolar growth seem to play an important role in influencing the permanent incisors into a more normal position with time. Although there may be insufficient room in the arch for the newly erupted permanent, its position will improve over several months.RX
It is unnecessary to subject the child to the trauma of extraction of the primary teeth because the problem is always self-correcting within few months. While for older children(7.5 years of age and more) with the radiograph shows no root resorption for the primary teeth, self-correction has not been achieved and the corresponding primary teeth should be removed. The molding action of the tongue and the lips improve their relationships within months.
Teething and difficult eruption
Teething is the physiologic process of the eruption of primary teeth through the gums. In most children the eruption of primary teeth is preceded by:
increased salivation.
itching sensation and the child will want to put the hand and fingers into the mouth.
The child feels restlessness.
Inflammation of gingival tissue.
No evidence of high fever, diarrhea, facial rash, or sleep problems.
Management
Eruption takes place over a period of two years.
Reassurance of parents regarding teething signs and symptoms
Giving the child object to bite on, cold object may cause pain relief through pressure of biting and may accelerate tooth eruption
Cold vegetables like chilled carrots or chewy toys
Topical medication(If the child is having extreme difficulty, the application of topical anesthetic may bring temporary relief. The parent can apply the anesthetic to the affected tissue three or four times a day. Caution must be exercised, because systemic absorption of the anesthetic agent is rapid, and toxic doses can occur if it is misused.
Systemic medication like antipyrol 4-6 hours.
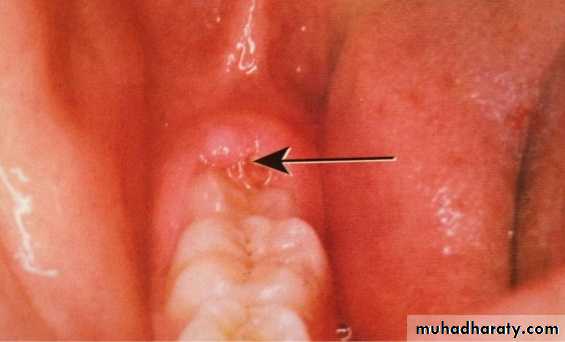
Eruption haematoma (eruption cyst)
A bluish purple, elevated area of tissue.
Occasionally develops a few weeks before the eruption of a primary or permanent tooth.
Result from trauma to the area and a hemorrhage on follicle of erupted tooth.
Subsides after eruption.
Mainly associated with 6s and Es region.
The condition is always self-limiting and the treatment is rarely necessary, however, surgically uncovering the crown may occasionally be justified.
Reassuring the parents that the lesion is not serious.

Eruption sequestrum
The eruption sequestrum is seen occasionally in children at the time of the eruption of the first permanent molar.Tiny spicule of nonviable bone overlying the crown of an erupting tooth just before or immediately after the emergence of the tips of the cusps through the oral mucosa.
Should be removed to control local inflammation.
Treatment
Topical anesthesia should be given to prevent discomfort that associated with its removal from gingival tissue.
Early eruption
Natal and Neonatal teeth
Natal teeth: (teeth present at birth).
Neonatal teeth: (teeth that erupt during the first 30 days).
Most of the time, the two lower front teeth are the only ones present. They are usually “wobbly,” not firmly attached like normal “baby teeth.” Sometimes they are normal teeth that have erupted (come up) early; at other times they are extra (supernumerary) teeth.
Early eruption of primary teeth seems to be familial, A radiograph should be made to determine the amount of root development and the relationship of a prematurely erupted tooth to its adjacent teeth.
Management
Most prematurely erupted teeth (immature type) are hyper mobile because of the limited root development. Some teeth may be mobile to the extent that there is danger of displacement of the tooth and possible aspiration, in which case the removal of the tooth is indicated.
In some cases, the sharp incisal edge of the tooth may cause laceration of the lingual surface of the tongue (Riga-Fede disease), or interfere with nursing and the tooth may have to be removed.
The preferable approach, however, is to leave the tooth in place because of its importance in the growth and uncomplicated eruption of the adjacent teeth. Within a relatively short time the prematurely erupted tooth will become stabilized, and the other teeth in the arch will erupt.
Epstien Pearls, Bohn Nodules, Dental lamina cysts
Small, white or grayish white lesions on the alveolar mucosa of the newborn
may on rare occasions be incorrectly diagnosed as natal teeth.
The lesions are usually multiple but do not increase in size.
No treatment is indicated, since the lesions are spontaneously shed a few weeks after birth.
Clinical appearance
1. Epstein pearls are formed along the midpalatine raphe. They are considered remnants of epithelial tissue trapped along the raphe as the fetus grew.
2. Bohn nodules are formed along the buccal and lingual aspects of the dental ridges and on the palate away from the raphe. The nodules are considered remnants of mucous gland tissue and are histologically different from Epstein pearls.
3. Dental lamina cysts are found on the crest of the maxillary and mandibular dental ridges. The cysts apparently originated from remnants of the dental lamina.
Local and systemic factors that influence eruption
Local factors:Infection around the tooth.
Supernumerary teeth
Trauma
Gingival fibromatosis
Ankylosed teeth
Ankylosed teeth
The tooth is in a state of static retention, whereas in the adjacent areas eruption and
alveolar growth continue. The mandibular primary molars are the teeth most often observed to be ankylosed, ankylosis of anterior teeth does not occur unless there has been trauma.
Diagnosis of ankylosed teeth
Eruption has not occurred.Alveolar process has not developed in normal occlusion.
The opposing tooth is out of occlusion.
Even with extensive root resorption, the tooth is not mobile.
Diagnosis is by tapping with a blunt instrument.(Ankylosis can be partially confirmed by tapping the suspected tooth and an adjacent normal tooth with a blunt instrument and comparing the sounds. The ankylosed tooth will have a solid sound, whereas the normal tooth will have a cushioned sound because it has an intact periodontal membrane that absorbs some of the shock of the blow.
Radiographically, a break in the continuity of the periodontal membrane.
Treatment of ankylosed teeth
Early diagnosis is important
Treatment may involve surgical removal
Loss of arch length is evident, the dentist may choose to keep the tooth under observation
The tooth that is definitely ankylosed may undergoes root resorption and be normally exfoliated.
Systemic factor
Mongolism( downs syndrome)
Cleidocranial dysplasia
Hypothyroidism
hypopitutarism
Achondroplastic dwarfism
Mongolism (down syndrome)
Etiology:
Extra chromosomal that is trisomy 21. i.e. , the presence of Three chromosomes in number 21 rather than the normal two.
Characteristic facial pattern and oral manifestation:
The orbits are small, the eyes slope upward, and the bridge of the nose is more depressed than normal.Mental retardation.
Delay eruption of the teeth frequently occurs.
The eruption often follows an abnormal sequence.
Some of the primary teeth may be retained until 15 years
Retardation in the growth of the maxillae and mandible .
The smaller jaws contribute to a tendency for protrusion of the tongue and dental crowding.
The tongue also tends to be larger than normal.
Higher prevalence of periodontal disease
High prevalence of necrotizing ulcerative gingivitis
Low caries susceptibility in both primary and permanent dentition.
Cleidocranial dysplasia
A rare congenital syndrome which has also been referred to as cleidocranial dysostosis. Transmission of the condition is by either parent to a child of either sex
The diagnosis is based on the finding of an absence of clavicles.
The fontanels are large, and radiographs of the head show open sutures
The patients exhibited mandibular prognathism caused by increased mandibular lengths and short cranial bases.
The development of the dentition is delayed.
Complete primary dentition at 15 years of age resulting from delayed resorption of the deciduous teeth and delayed eruption of the permanent teeth is not uncommon
presence of supernumerary teeth.
Hypothyroidism
Congenital Hypothyroidism (Cretinism) occur at birth and during the period of most rapid growth, It result from absence or underdevelopment of the thyroid gland and insufficient levels of thyroid hormone
An inadequately treated child with congenital hypothyroidism is a small and disproportionate person, with abnormally short arms and legs. The head is large, and obesity is common.
The dentition is delayed in all stages, including eruption of the primary teeth, exfoliation of the primary teeth, and eruption of the permanent teeth. The teeth are normal in size but are crowded in jaws that are smaller than normal.
The tongue is large and may protrude from the mouth.
The abnormal size of the tongue and its position often cause an anterior open bite and flaring of the anterior teeth.
The crowding of the teeth, malocclusion, and mouth breathing cause a chronic hyperplastic type of gingivitis.
Hypopitutarism
An early hypofunction of the pituitary gland result in Pituitary dwarfism.
Deficiency in secretion of the growth hormone result in decrease in the growth of the bones and soft tissues of the body.
Delayed eruption of the dentition is characteristic. In severe cases the primary teeth do not undergo resorption but instead may be retained throughout the life of the person. The underlying permanent teeth continue to develop but do not erupt. Extraction of the deciduous teeth is not indicated, since eruption of the permanent teeth cannot be assured.
Achondroplastic dwarfism
The etiology of Achondroplastic dwarfism is unknown, it is clearly an autosomal dominant disorder
diagnosed at birth demonstrates a few dental findings.
Growth of the extremities is limited because of a lack of calcification in the cartilage of the long bones.
The head is large, although the trunk is normal in size. The fingers may be of almost equal length, and the hands are plump.
The fontanels are open at birth.
The upper face is underdeveloped, and the bridge of the nose is depressed.
The maxilla may be small, with resultant crowding of the teeth and a tendency for open bite. A chronic gingivitis is usually present .
Development of dentition is slightly delayed.