fourth stage
Community MedicineLec-( )
10/11/2015
DiphtheriaDiphtheria is an acute, communicable disease caused by the gram-positive bacillus Corynebacterium diphtheriae.
Infection may result in clinical disease, which has two forms — respiratory and cutaneous — or in an asymptomatic carrier state.
Epidemiology
Among non immunized populations, diphtheria most often occurs during fall and winter, although summer outbreaks have occurred.In tropical areas inapparent , cutaneous & wound diphtheria infections are more common.
Disease spreads more quickly and is more prevalent in poor socioeconomic conditions, where crowding occurs and immunization rates are low.
Race ----> No racial differences observed
Sex ------> No difference has been described for acute infection; however, in surveys from around the world, lack of immunity was more pronounced in elderly women than in men.
Age ----> Diphtheria affect children 1-5 years. in countries where wide spread immunization is practiced ,a shift in age incidence has been observed from preschool to school age.
Chain of events
Reservoir -----> Human
Mode of transmission
Direct contact with patients or carriers
Indirect
Articles
Raw milk
Incubation period ---> 2-5 days
Period of communicability
Unless treated, the period of communicability varies from 14-28 days from the onset of disease.
Carriers may remain infective for longer periods.
A case or carrier may be considered non-communicable when 2 cultures from the nose and throat ,24 hr apart, negative for diphtheria bacilli.
Susceptibility & resistance
Disease or in apparent infection not always lead to lifelong immunity
Toxoid gives prolonged but not lifelong immunity which decreased with age.
Clinical features
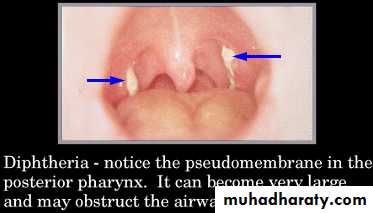
Respiratory tract form of diphtheria consist of pharyngotonsillar ,laryngotracheal ,nasal and combination of these forms.Pharyngotonsillar : sore throat, low grad fever, O/E mild pharyngeal erythema and localized exudate or grey-black adherent membrane, Attempt to remove the membrane result in bleeding

Laryngotracheal disease most often proceeded by pharyngotonsillar diphtheria, patient presented with hoarseness of voice and croupy cough.
Non-respiratory mucosal surface may be a site of infection (conjunctiva ,genital tract)
Cutaneous form common in tropical areas ,patient presented with ulcer surrounded by erythema and covered by membrane .
Diagnosis
Clinical findings
Bacteriological examination
Isolation of CoryneBacterium diphtheriae on cultures with toxigenicity testing confirm the diagnosis.
In all patients in whom diphtheria is suspected, obtain specimens from the nose and throat (i.e., nasopharyngeal and pharyngeal swab) for culture
Isolation of C .diphtheriae from close contacts may confirm the diagnosis, even if results of cultures on specimens taken from the patient are negative.
Prevention
Educational measures About the hazards of the disease and Importance of immunization
Active immunization should be initiated in infancy (DTaP, DTP)
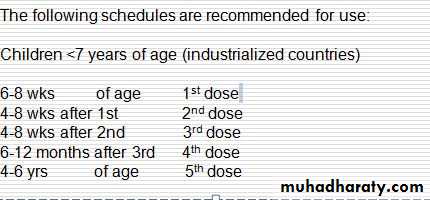

This schedule does not need to be restarted because of delay in administering the scheduled dose .
If pertusis component of DTP is contra-indicated DT should be given.
A booster dose of adult formulation Td is recommended at 11-18 years of age.
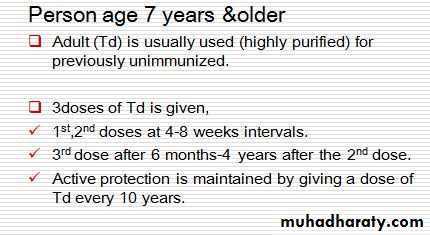
3. Protection of highly risk group ; They should be fully immunized and receive a booster dose every 10 years.
4. HIV & immunocompromised children should be vaccinated. Use the same schedule
Control
Reporting ---> obligatoryIsolation:
strict isolation for pharyngeal type, contact isolation for cutaneous.
Until 2cultures both from nose &throat
taken( not less than 24 hours apart, & not less than 24 hours after cessation of antibiotic therapy) fail to show the microorganism.
If there is no facility isolation may be end after 14 days course of appropriate antibiotic therapy.
Disinfection
4. Contacts
7 days surveillanceCultures from nose &throat
Single dose of benzathin penicillin IM (600,000units for younger persons < 6years & (1.200.000units for older persons) or 7-10 days course of erythromycin recommended for all persons with household exposure, regardless of their immunization status
5. Specific treatment
Antitoxin
Antibiotic
Antitoxin
Sensitivity testing
Single daily dose 20000 units for anterior nasal diphtheria to100000 units for extensive disease by IM route for 14 days after bacteriological specimens are taken without waiting for results.
Antibiotics
Procaine penicillin G (IM) (25 000 –50 000 units/kg/day for children and 1.2 million units/kg/day for adults in 2 divided doses)
Parental erythromycin (40-50 mg/kg/day with a maximum of 2 grams/ day in divided doses).
Recommended duration is 14 days
Prophylactic treatment of carriers
A Single dose of benzathin penicillin IM (600,000units for younger persons < 6years (1.200.000units for older persons) or 7-10 days course of erythromycin is recommended.
Epidemics measures
Immunize all <5 & highly risk groups . Repeat immunization one month later to provide at least 2 doses to the recipient.
Identify contacts, population at risk.
Carry out special investigation of reported cases to verity diagnosis &to determine biotype & toxigenicity of the organism.