1
4th stage
Obstetrics
Lec. 4
Dr.Wildan
3/11/2015
Fetal circulation & Amniotic fluid
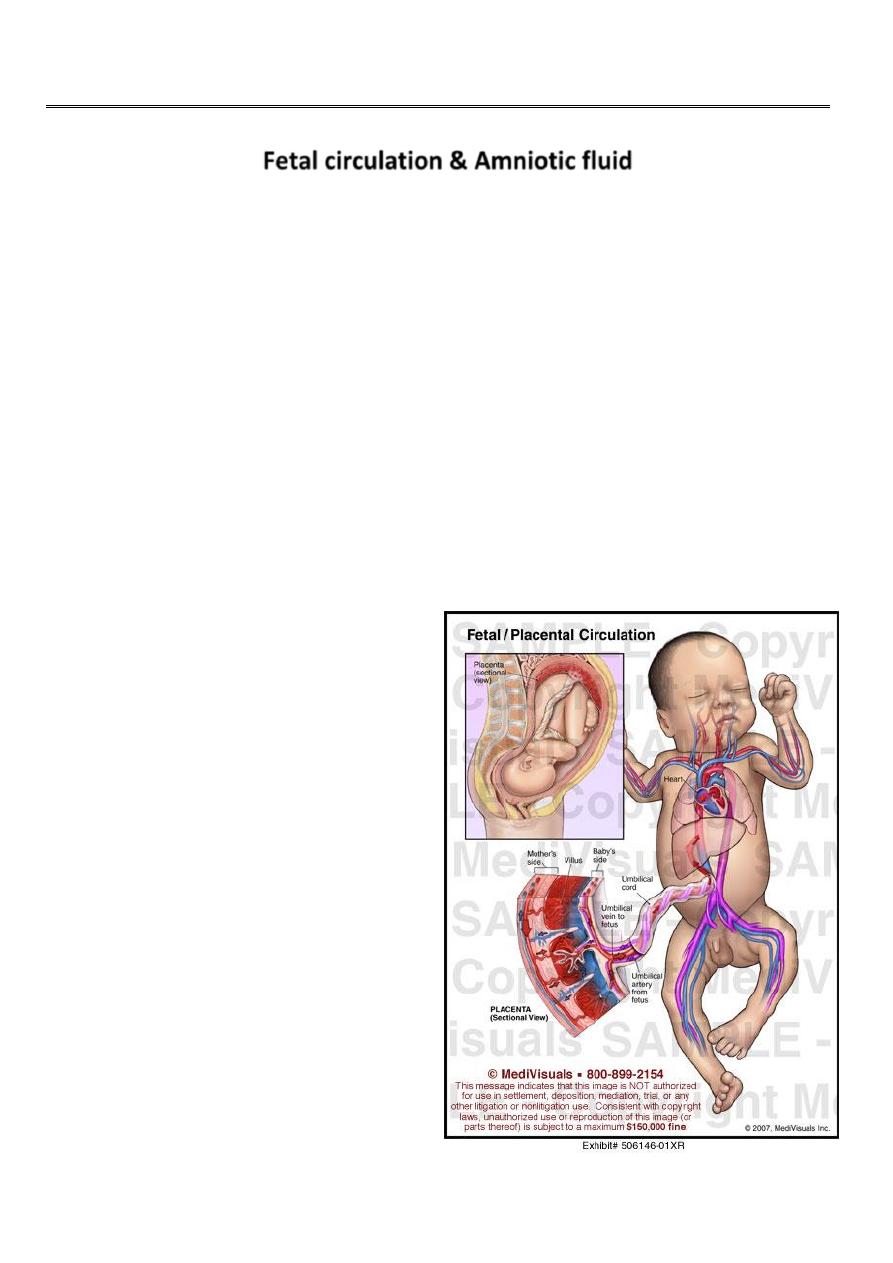
The fetal circulation :
The fetal circulation is quite different from that of the adult and functions smoothly
until the moment of birth.
Its distinctive features are:
Oxygenation occurs in the placenta.
The right & left ventricle work in parallel rather than series.
The heart, brain & upper body receive blood from the left ventricle (highly
oxygenated blood), while the placenta & lower body receive blood from both Rt
& Lt ventricle.
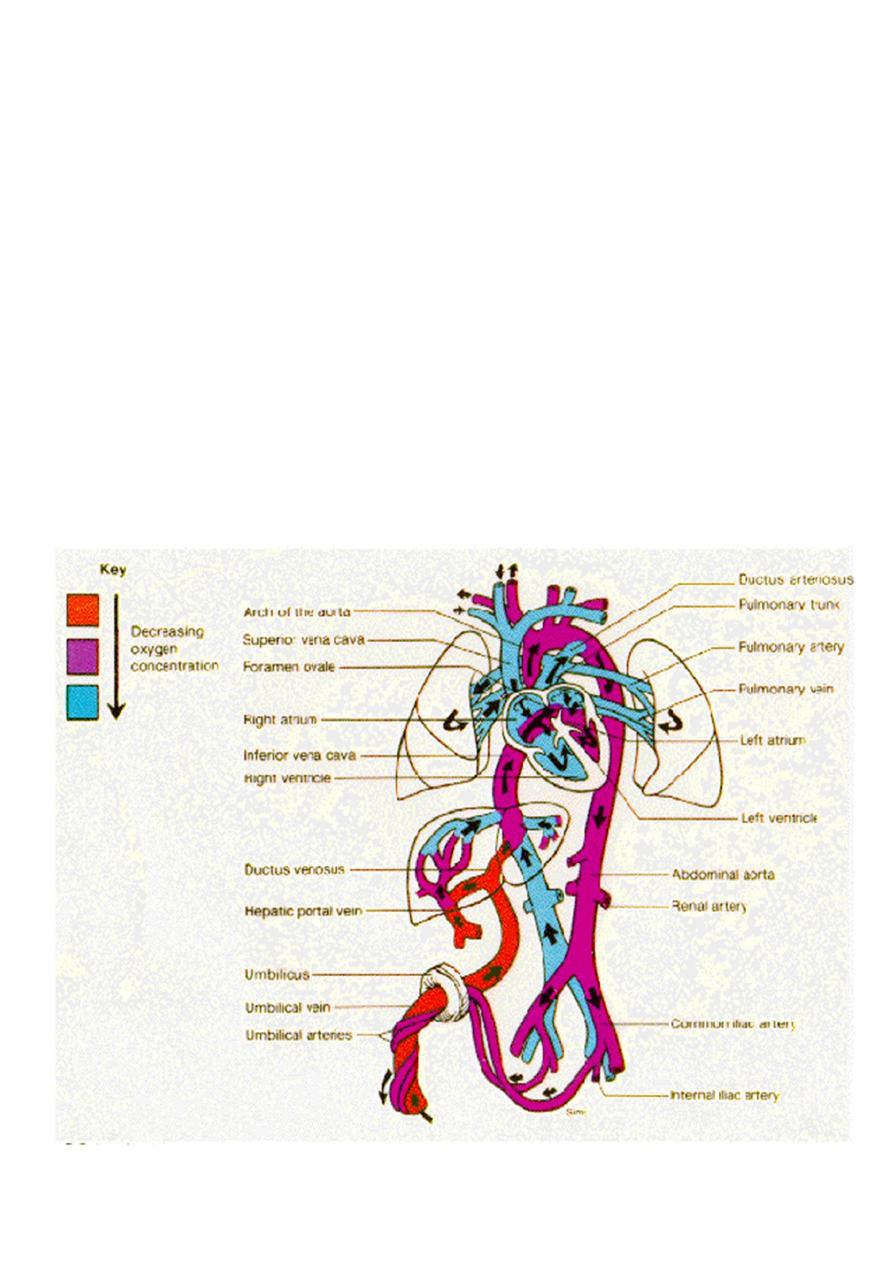
Oxygenated blood is brought from the placenta to the fetus by the umbilical vein
(80%). The vein then divides into; the ductus venosus and portal sinus.

2
The ductus venosus, which is the major part and traverses the liver to enter the
inferior vena cava directly. The ductus venosus doesn’t supply oxygen to the
intervening tissues, so it carries a well oxygenated blood (80%) directly to the heart.
In contrast the other division, the portal sinus, carries blood to the hepatic vein, where
oxygen is extracted. This relatively deoxygenated blood from the liver then flows to
the inferior vena cava, which also receives less oxygenated blood retaining from the
lower part of the body.
Blood flowing to the heart from the inferior vena cava, therefore, consist of arterial-like
blood that pass directly from the ductus venosus, and less oxygenated blood from the
lower part of the body (below the diaphram). The oxygen content of the blood
reaching the heart (70%) is therefore less than that leaving the placenta.
The well oxygenated blood will enters the left ventricle (supply the heart and the
brain). The less oxygenated blood enters the right ventricle (supply the rest of the
body).
The two separate circulations are maintained by the structure of the right atrium,
which effectively directs blood to the left atrium or the right ventricle depending on its
oxygen content.
Once the blood enter the atrium, the configuration of the upper interatrial septum
(crista dividens) is such that it shunts the well oxygenated blood to the left atrium and
the less oxygenated to right ventricle.
This separation is also facilitated by the pattern of blood flow in the inferior vena cava,
when the well oxygenated blood flow along the medial aspect and the less
oxygenated blood along the lateral aspect, facilitating blood shunting to the opposite
side of the heart.
The well oxygenated blood pass from the right atrium to left atrium through the
foramen ovale, & from thence it passes into left ventricle & out into the ascending
aorta. By this arrangement the coronary arteries & the brain receive the most
oxygenated blood.
3
Blood returning from the head & upper limbs through the superior vena cava streams
towards the tricuspid valve to enter the right ventricle.
The less oxygenated blood coursing along the lateral aspect of the inferior vena cava,
reaching the right atrium and then passes through the tricuspid valve to the right
ventricle. The major part 87% of the right ventricle blood is shunted through the
ductus arteriosus to the descending aorta (60%).
On the other hand only 13% of the right ventricular out put is passed to the lung, this is
because of high vascular resistance at the pulmonary circulation and lower resistance
at the ductus arteriosus and the umbilical-placental vasculature.
About 1/3 of the blood flow through the ductus arteriosus pass to the body ,and the
other 2/3 is passed to the placenta through the two hypogastric arteries (distally
become the umbilical artery) then the blood comes back from the placenta by the
umbilical vein.

4
Changes in the fetal circulation after birth:
After birth the umbilical vessels, ductus arteriosus,foramen ovale,and ductus
venosus normally constrict or collapse. With the functional closure of the
ductus arteriosus and expansion of the lung, the blood leaving the right
ventricle will preferentially enter the pulmonary circulation to be oxygenated
before it return to the left heart.
The heart ventricles which was working in parallel will work in series.
The distal portion hypogastric artery (umbilical artery) will be atrophied and
obliterated within 3-4 days forming the umbilical ligaments.
Intra-abdominal reminant of the umbilical vein form the ligamentum teres.
Ductus venosus constrict by 10-96 hours after birth, anatomically become closed
by 2-3 weeks (ligamentum venosum).
The oxygen supply to the fetus :
As the fetus grows it requires increasing amounts of oxygen. This is achieved by :
Increase in placental transfer of oxygen due to reduction in the diffusion
distance.
Increase in the Hb contents of fetal blood .
Fetal haemoglobin (HbF) (made in the liver and spleen not in the bone marrow)
has different structure from adult HbA.
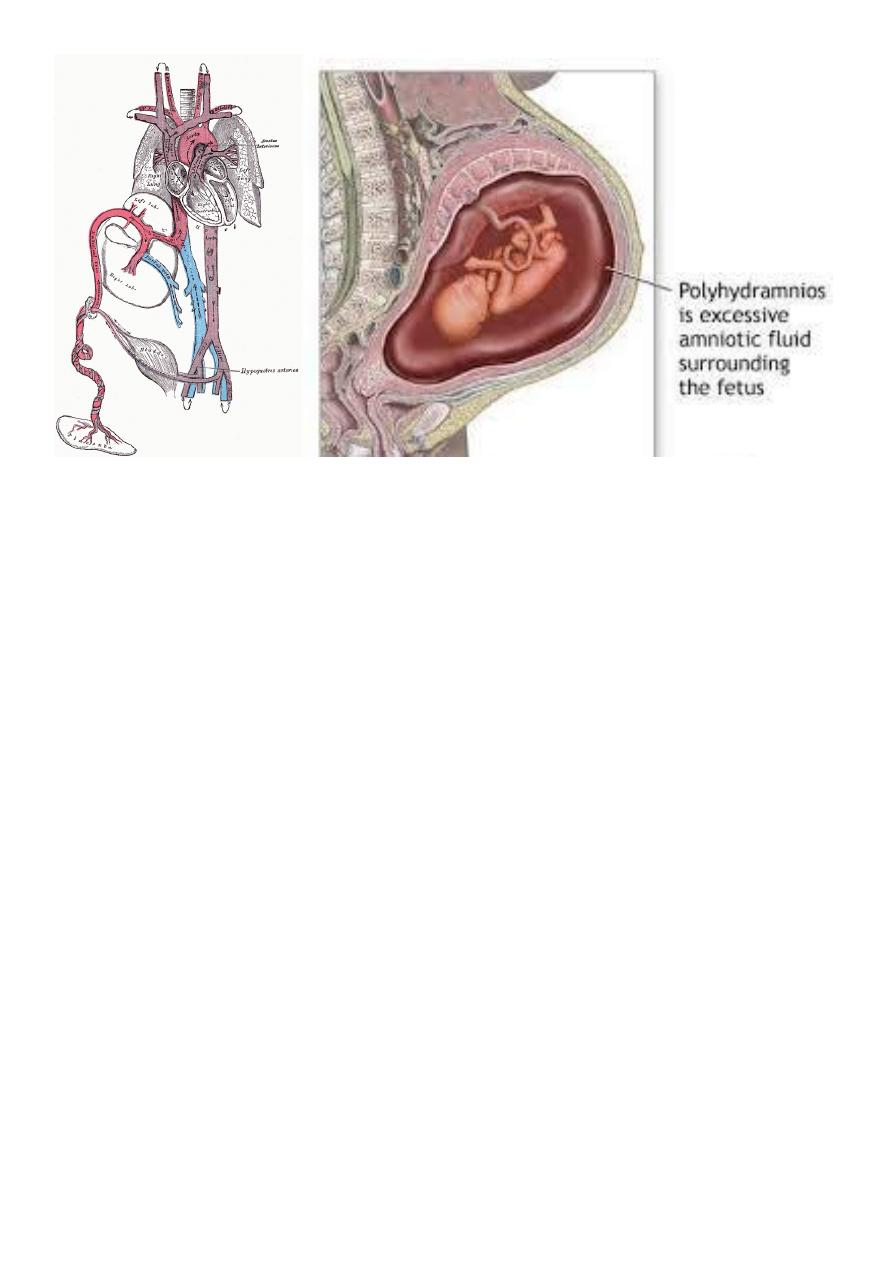
The amniotic fluid :
The amniotic fluid has a mixed origin and has heterogeneous composition. It's
slightly turbid from the mixture of solid particles derived from fetal skin and
amniotic epithelium.
May stained a green or brown if it contain meconium.

5
The solid matter composed langue hairs, epithelial cells, sebaceous material from the
fetal skin, and cast- off amniotic epithelial cells.
The volume of the amniotic fluid at term is about 800 ml ( range 400-1500 ml).
10 weeks 30ml
12 weeks 50ml
20 weeks 300ml
30 weeks 600ml
The rate of increase is about 30ml/week,This rate decrease near term (the maximum
amount relative to the fetal size is at 30 week).
At term the specific gravity of the fluid is 1010.
It has organic, inorganic and cellular constituents. Some concentration of
important contents near term are:
sodium 130mmol/l
urea 3-4mmol/l
protein 3 g/l
lecithin 30-100mg/l
alpha-fetoprotein 0.5-5 mg /l
It’s mildly bacteriostatic ,contain traces of steroid, non steroid hormones and
enzymes.
PH = 7.
Production of amniotic fluid :
It’s of both maternal and fetal origin, the relative importance of both mechanisms
alters as pregnancy progresses.
In early pregnancy it is from the maternal plasma (ultra filtrate).
By the 2
nd
trimester diffusion through the fetal skin.
After 20 weeks, the fetal kidneys play an increasing role in the production of the
amniotic fluid.( at term 500ml/day).
Pulmonary fluid contributes a small portion.

6
Disposal of the amniotic fluid :
It’s partly by the absorption through the amnion in to maternal plasma and partly
fetal swallowing and absorption by the fetal intestine to enter the fetal plasma.
Functions of the amniotic fluid :
1. Guards the fetus against mechanical shocks, and equalizes the pressure exerted by
uterine contractions.
2. Room for fetal movement.
3. Maintain the temp. of the fetus. so the fetus is not subjected to heat loss.
4. It can hardly regarded as a source of nutrition since it contain small amounts of salts
and protein.( swallowing).
5. The forewater bag form a wedge which with uterine contraction dilates the internal
os and the cervical canal.
6. At the rupture of the membrane during labour the fluid flushes the lower genital
tract( aseptic and bactericidal).
7. The amnion produce a variety of bioactive compounds including vasoactive peptides,
growth factors, and cytokines which modulates chorionic vessels flow or promotes
cell replication and calcium metabolism.
Investigation of the amniotic fluid:
Samples of amniotic fluid can be obtained during pregnancy for various diagnostic
purposes by abdominal amniocentesis, and a variety of chemical estimations for
normal and pathological constituents can be made. Fetal amniotic cells can be
obtained for tissue culture and chromosomal study.
7