Forth stage
surgeryLec-2
د.سمير الصفار
25/10/2015
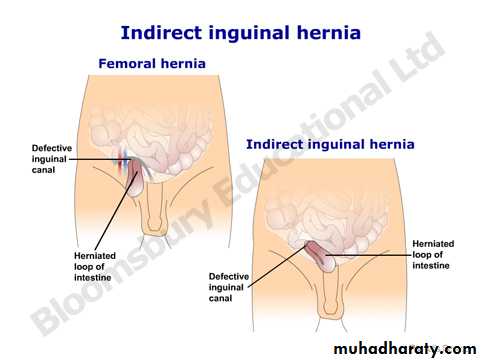
Indirect Inguinal hernia
Epigastric hernia
Epigastric herniaUmbilical hernia
Umbilical herniaSpigelian Hernia
Spigelian Hernia
Inguinal hernia
Inguinal hernia

Diagnosis:
Groin swelling that disappear with supine positionExamine erect and supine
Does not transilluminate
Expensile cough impulse
How to differentiate IIH from DIH
When the swelling localized to groinThe differential diagnosis:
Femoral hernia
Lipoma of cord
Inguinal lymphadenopathy
Incompletely descended testis
Ectopic testis
Femoral artery aneurysm
Differential Diagnosis
When the swelling is inguino-scrotal
Vaginal hydrocele
Encysted hydrocele of cord
Spermatocele
Varicocele
Epididymoorchitis
Torsion of testis
Testicular tumor
In female
Femoral hernia
Hydrocele of canal of Nuck
Inguinal lymphadenopathy
Treatment:
Operation is treatment of choice:Open surgery
The standard method
Laparoscopic hernia repair
should be reserved for bilateral or recurrent hernia
Open surgery
Herniotomy
Herniorrhaphy
Anaesthesia
LocalSpinal
General
Herniotomy
Indications:In infants, children and adolescents
Steps of surgery:
Dissection of sac
Open of sac
Reduction of contents
Transfixation of neck
Cut of reminder
Herniorrhaphy
Repair of stretched DIR and transversalis fasciaReinforcement of posterior wall by:
Shouldice repair
Mesh repair
Complications:
Bleeding
Skin bruises, SC hematoma
Scrotal hematoma
Retention of urine
Wound infection
Injury to vas deference
Ischemic orchitis
Neuralgia
-Ilioinguinal
-Iliohypogastric
-Genitofemoral
-Lateral cutaneous
Recurrence >1%
Direct Inguinal Hernia
AcquiredAdults
35% of inguinal hernia
12% bilateral
Not occur in females
Anatomy of Direct Hernia:
Hesselbach’s triangle
Inguinal ligament (base), rectus (medial), inferior epigastric vessels (lateral)
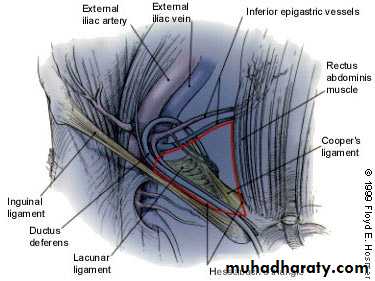
Hesselbach’s triangle
Pathogenesis:Through weak posterior wall of inguinal canal
Medial to Inferior epigastric vv
Not attain large size or descent into scrotum
Lies behind spermatic cord
Wide neck
Varieties
Dual ( Pantoloon,saddle bag)Funicular (Prevesical)
Clinical Features:
Swelling in the groin
On examination:
controlled on pressing on SIR
ECI
Treatment:
Surgical repair
Dissection of sac
Inverted
Repair of transversalis fascia
Mesh(Lichtenstein) or Shouldice repair
Strangulated Inguinal Hernia
Can occur at any timeMore liable to occur in patients with irreducible hernia.
More commonly occur in IIH
Less often in DIH
Constricting agent
Neck of sac
External inguinal ring
Adhesions within the sac
Content of hernia
Small intestine
Omentum
Both
Clinical features:
Severe pain in the groinVomiting
General upset
Fever ?
Swelling with skin discoloration in the groin
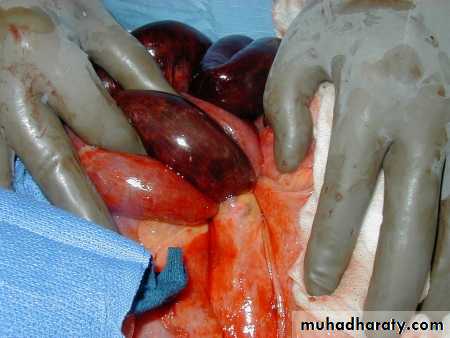
Gangrenous bowel
Gangrenous bowel
Severely tender
Abdominal signs
Treatment:
Urgent surgery
Pinciples:
-Dissection of sac
-Open the sac
-Exploration of content
-Excision of gangrenous tissues
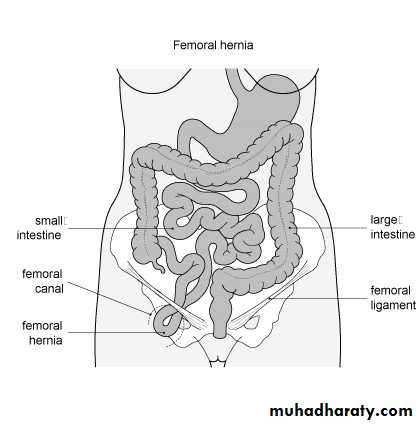
Femoral Hernia
Anatomy of the femoral canal
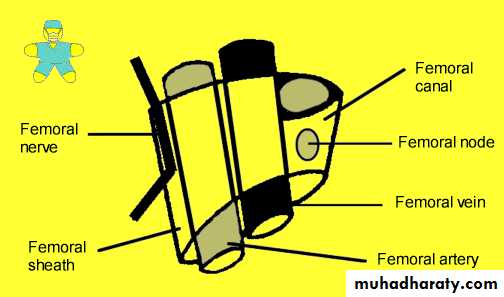
Boundaries of femoral ring
Anterior border is the inguinal ligamentPosterior border is the pectineal ligament
Medial border is the lacunar ligament
Lateral border is the femoral vein
Femoral Hernia
Women> men20% of hernias in women
More in parous
Most liable for strangulation
Clinical features
Rare before puberty
May be un-noticed by the patient
Strangulated hernia
Sudden painful swelling in the groinAbdominal symptoms
Examination
The swelling is inferior to inguinal ligament and lateral to pubic tuberculeMostly irreducible
Differential Diagnosis:
Inguinal herniaLymphadenopathy
Saphena varix
Ectopic testis
Psoas abscess
Distended Psoas bursa
Lipoma
Rupture of adductor longus
Treatment:
Uncomplicated hernia:
Operation as early as possible
Strangulated hernia
Urgent surgery
Approaches for the surgery
Low approach – Lookwood
High approach - McEvedy
Inguinal approach - Lotheissen
Principle of surgery
Dissection of sacOpen sac
Reduction of contents if healthy otherwise gangrenous tissue must be excised.
Repair of femoral ring