The oesophagus
IntroductionAnatomy
Physiology
Clinical features
Investigations
Diseases
Congenital
Acquired
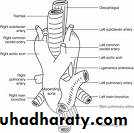
Surgical Anatomy
The esophagus is a muscular tube approximately 25 cm long.The musculature of the upper 5%, including the upper esophageal sphincter, is striated; the middle 40% has mixed striated and smooth muscle, the distal 55% is entirely smooth muscle.
There are an upper and a lower esophageal sphincters.
The parasympathetic nerve supply is mediated by the vagus.
Physiology
The main function of the esophagus is to transfer food from the mouth to the stomach.
The initial movement of food from the mouth is voluntary.
The upper esophageal sphincter is normally closed at rest and serves as;
* A protective mechanism against regurgitation of esophageal contents into the respiratory passages.
* Also it serves to stop air entering the esophagus.
The lower esophageal sphincter(LOS) is a physiological sphincter, about 3-4 cm in length and has a pressure of 10-25 mmHg.
The tone of it is influenced by many things including food, gastric distension, smoking, and GI hormones.
Its main function is to prevent gastric and duodenal contents from refluxing into the lower oesophagus.
Clinical featuresSymptoms
Dysphagia
is the term used to describe difficulty, but not necessarily pain, on swallowing.
The type of dysphagia is important; it may be dysphagia for solids or fluids, intermittent or progressive.
Odynophagia
It refers to pain on swallowing.
Regurgitation and reflux
Regurgitation strictly refers to the return of esophageal contents from above an obstruction in the esophagus.
Reflux is the passive return of gastroduodenal contents to the mouth.
Chest pain
Chest pain similar in character to angina pectoris may arise from an esophageal cause.
Other symptoms of esophageal disorders include; loss of wt, anaemia, cachaxia, change of voice, and cough.
Investigations
Radiography
Plain X ray; may show opaque foreign bodies.
Contrast radiography (Barium swallow) is a useful investigation for demonstrating narrowing, space-occupying lesions, anatomical distortion or abnormal motility.
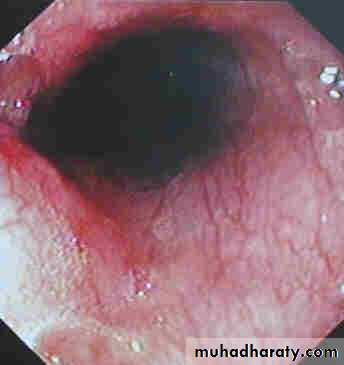
Endoscopy
Is the investigation of first choice for most esophageal disorders.
It is either for diagnostic or for therapeutic purposes.
Diagnosis is by visual inspection of the inside of esophagus and also by taking a biopsy or cytology specimen.
For therapy, can be used for;
Removal of FB
Dilatation of strictures
esophageal varices
There are two types of endoscopy;
Rigid oesophagoscopy; which is now virtually obsolete.
Disadvantages:
Needs general anaesthesia, difficult to introduce, and carry high risk of perforation
Fibre-optic endoscopy
It has virtually supplanted the rigid instrument.
It is done under local anaesthesia on an out-patient basis, easy to enter, and carry low risk of perforation.
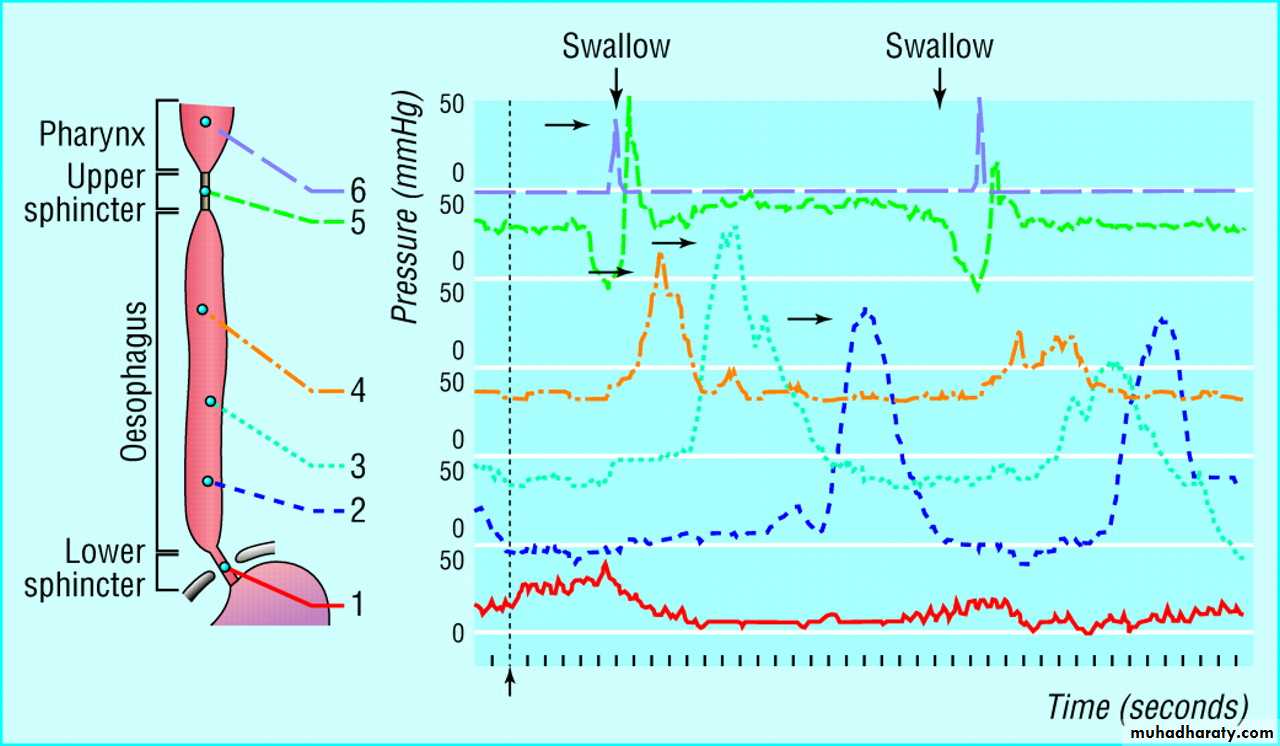
Esophageal manometry
Is widely used to diagnose esophageal motility disorders.
Recordings are usually made either by;
Multilumen catheter
Catheters with solid-state transducer
24-hour pH recording
Prolonged measurement of esophageal pH is now accepted as the most accurate method for the diagnosis of gastrooesophageal reflux.
Diseases of oesophagus
Congenital abnormalities
Atresia and tracheo-oesophageal fistula
Oesophageal stenosis
Dysphagia lusoria
Foreign bodies in the oesophagus
A lot of things may become arrested in the oesophagus such as coins, pins, dentures. The commonest impacted material is food.Plain radiographs are the most useful examination.
Endoscopy is good tool for the dx specially of non-opaque FB.
Treatment:
Flexible endoscopy is now the method of choice and the majority of objects can be extracted with suitable grasping forceps, a snare or a basket.
An impacted food bolus will often break up and pass on if the patient is given fizzy drinks and confined to fluids for a short time
Perforation of the oesophagus
Iatrogenic (50%)Spontaneous
Traumatic
Perforation of the oesophagus is a serious condition that requires prompt diagnosis and treatment.
Causes:
Iatrogenic (50%)
Spontaneous
Traumatic
Iatrogenic Perforation of oesophagus
Instrumental perforation
Spontaneous Perforation of oesophagus
Pathological perforation
Perforation of ulcers, such as a Barrett’s ulcer or tumours.
Barotrauma _ Boerhaave’s syndrome
*Barotrauma _ Boerhaave’s syndrome
is usually due to severe barotrauma when a person vomits against a closed glottis.Boerhaave’s syndrome
Usually the perforation at the lower third
The clinical history is of severe pain in the chest or upper abdomen following a meal or a bout of drinking.
Traumatic Perforation of oesophagus
Penetrating injury
*Foreign bodies
Diagnosis
Beware and beware of perforationChest pain
Subcutaneous emphysema in the neck
Emphysema around the pericardium can be detected on auscultation as a mediastinal crunch
Chest XR may show gas in the mediastinum
Contrast swallow using barium suspension
Treatment
Prompt dx and treatment is essential for the best results
There are two options:
Operative
Non-operative
Management options in perforation of the oesophagus
Factors that favour
Nonoperative Operative
Small septic load Large septic load
Minimal CV upset Septic shock
Perforation confined to Pleura breached
Mediastinum
Endoscopic perforation Boerhaave syndrome
Perforation of cervical Perforation of abdominal
Oesophagus oesophagus
Nonoperative management
Analgesia
Nil by mouth
Antibiotics
General supportive care…IV fluids
When stable…enteral or paenteral nutrition
Nasogastric tube is not recommended
Operative management
It involves thoracotomy and repair of the perforation
This is best done within a few hours of perforation
Gastro-oesophageal reflux disease
Pathophysiology:Competence of the gastro-oesophageal junction is dependent into:
*Physiology of LOS;
basal tone, length, intra-abdominal length
*Anatomy of the cardia
Diaphragmatic hiatus-Sliding hiatus hernia
There are two types of reflux:
Physiological reflux
It may occurs after meals
Physiological reflux occurs during transient lower oesophageal sphincter relaxations(TLOSRs)
Pathological reflux
Is by far the commonest condition affecting the upper GI tract.
Its incidence increased during the last years;
Which is attributed to Improvement of socioeconomic conditions, eradication of H.pylori , decrease incidence of DU
Obesity
Clinical features
Retrosternal burning pain( heartburn)Epigastric pain
These are usually provoked by food, particularly fatty food.
Unpleasant acidic taste
In advanced cases there is a history of pain and reflux when lying flat or on stooping.
Odynophagia
Less typical symptoms;
Angina-like chest pain
Pulmonary or laryngeal symptoms
Dysphagia
Diagnosis of GORD
In the majority of cases the dx is assumed rather than proven and treatment is empirical
Endoscopy;
To exclude serious pathology
Reflux oesophagitis
Peptic stricture
Barrett’s oesophagus
Oesophageal manometery
24-hours oesophageal pH recording
Is the gold standard for the dx of GORD
Barium swallow and meal;
Gives the best appreciation of G-O anatomy but it is not important for the dx of GORD
Diffrential Dx
Achalasia and GORD are easily confused
Gall stones
Duodenal Ulceration
Management of uncomplicated GORDNon-operative management
Medical management
Simple medications; like
Antacids, H2 receptor anagonists
Simple measures; like
Advice about wt loss, smoking, excessive consumption of alcohol, tea or coffee, and a modest degree of head up tilt of the bed
Proton pump inhibitors;
Omeprozole, Lansoprazole and pantoprazole are by far the most effective drug treatment for GORD
Operative management
Surgery
Indications:
In uncomplicated GORD-
Failure of medical therapy..PPI
patient choice
Disadvantages of surgery:
1- Mortality (0.1-0.5%)
2- Failed operation (5-10%)
3-Side effects; dysphagia, gas bloat(5-10%)
What operation
There are many antireflux operations for GORD;Total fundoplication …Nissen 360
Disadvantage of Nissen:
Overcompetent cardia….Dysphagia, gas bloat syndrome
Partial fundoplication …Belsy 240
Disadvantage; high recurrence rate
Hill operation
Other antireflux procedures
Angelchik prosthesis
Silastic prosthetic collar
Partial gastrectomy with Roux-en Y reconstruction
What operative approach
Abdominal
Thoracic
Minimal access surgery…Laparoscopic approach
Complications of GORD
Reflux oesophagitis is a complication of GORD that occur in a minority of sufferers
Stricture …reflux induced stricture
Usually affect middle aged and elderlyD.Dx from malignant stricture
Treatment:
Dilatation
Long-term PPI
In younger and fit patients. May consider Antireflux surgery
Oesophageal shortening
Reflux oesophagitis…longitudenal contraction…secondary hiatus herniaThe main problem is during antireflux operation
Collis gastroplasty which produce neo-oesophagus around which a fundoplication can be done (Collis-Nissen operation)
Barrett’s oesophagus
(columnar-lined lower oesophagus)
Barrett’s oesophagus is a metaplastic change in the lining mucosa of the oesophagus in response to chronic gastro-oesophageal reflux
Risk of Barrett’s oesophagus
Barrett’s ulcer
Dysplasia…Carcinoma
Diagnosis of Barrett’s
OGD with biopsy

Dull red of the metaplastic columnar epithelium contrasts sharply with the pale glossy normal squamous lining
Treatment of Barrett’s oesophagus
The primary aim is to prevent Barrett's oesophagus from turning into oesophageal cancer.Of the underlying GORD
Ablation of abnormal mucosa by :
Laser
Photodynamic therapy
Argon beam plasma coagulation
Follow up: yearly OGD
Barrett’s ulcer
Is an ulcer in the columnar-lined portion of a Barrett’s oesophagus.Barrett’s ulcers may be deep and prone to bleeding or, rarely, perforation
Paraoesophageal (rolling) hiatus hernia
Is a true hernia that is prone to complications
True(pure) paraoesophageal hernia
Mixed paraoesophageal hernia
Sometimes the whole of the stomach lies in the chest and may undergo volvulus with perforation or gangrene.
Clinical features
Commonly occurs in the elderly, but it also may occur in young fit people
The symptoms are
Dysphagia
Chest pain
Symptoms of GORD
Investigations:
Plain X-ray of the chest
Barium meal
Endoscopy
Treatment
Rolling hernias always require surgical repair as they are potentially dangerousThe principle of surgery is :
Reduction of the hernia
Gastropexy
Some surgeons may perform a fundoplication
Neoplasms of the oesophagus
Benign tumours
Are rare
Leiomyoma is the commonest
Oesophageal polyps
Squamus cell polyp

Malignant tumours
Sarcoma are rareLeiomyosarcoma
Rhabdomyosarcoma
Malignant melanoma
Is rare
May be secondary
Poor prognosis
Carcinoma of the oesophagus
Is the sixth most common cancer in the world.
A disease of mid to late adulthood
Carry a poor prognosis, 5-year survival is only 5-10%
Pathology
Histologic types:
Squamous cell carcinoma (95%)
World-wide is the commonest tumour
Affect the upper 2/3rd
Adenocarcinoma (4%)
70% from Barrett esophagus
Is the commonest in westernised countries accounts for 60-75% of all oesophageal cancers.
Affect the lower 1/3rd
Radiological types
polypoid/fungating form (most common)
sessile/pedunculated tumor with lobulated surface
"applecore" lesion
ulcerating form
infiltrating form
gradual narrowing with smooth transition (DDx: benign stricture)
varicoid form: superficial spreading carcinoma
thickened nodular tortuous longitudinal folds (DDx: varices)
The poor prognosis of oesophageal cancer is proof of its ability to spread
This may be locoregional or systemic
Aetiology
Epidemiology
South africa
Northren Iran and china
The cause in endemic areas
Fungal contamination of food….carcinogenic mycotoxin
Nutritional deficiences
In non-endemic areas
Tobacco and alcohol are the major factors in the occurrence of squamous cancer.
High risk factors for oesophageal carcinoma
Alcohol and smoking
Long history of dyspepsia
Barrett’s oesophagus
Achalasia cardia
Stricture “ Corrosive,radiation”
Scleroderma
Plummer-Vinson syndrome
Hyperkeratosis(tylosis)
Clinical features
Patients with early disease may present with rather nonspecific dyspeptic symptoms or a vague feeling of “something that is not quite right” during swallowing.
Features of advanced disease
Dysphagia, is the usual presenting feature
Loss of weight
Hoarsenece of voice
Haematemesis or melaena
Palpable cervical lymphadenopathy
Diagnosis
Endoscopy; is the most important diagnostic tool and its widespread use is the major contributor to early diagnosis;
when the disease at a relatively early stage
when the chances of cure are greater.
It should be emphasised that biopsies should be taken of all lesions no matter how trivial they appear.
Contrast radiology “Barium swallow”;
The tumour appears as a filling defect in the lumen of oesophagus.
Not helpful for the diagnosis of early disease.
Gives a good assessment of the length of the lesions.
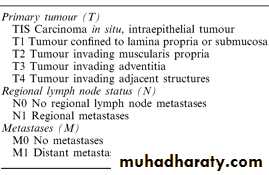
Staging:
Once a diagnosis of oesophageal carcinoma is made, staging of the disease is necessary to establish the appropriate method of treatment.
A careful search for metastatic disease
Chest X-ray
Ultrasonography
CT scan of chest and abdomen
MRI
Endoscopic ultrasonography
Bronchoscopy
Laparoscopy
Staging system
TNM classification system
T for tumour extent
N for lymph nodes assessment
M for distant metastases
General assessment
Assessment for fitnessNutritional assessment
Treatment of oesophageal cancers
The treatment depends on:the staging of the disease
the general condition of the patient.
The treatment options available are:
Surgerical excisionRadiotherapy
Chemotherapy
Intubation
Laser coagulation
Combined modality treatment
The treatment is either Radical or Palliative
Radical treatment;
Indicated for potentially curable disease in fit patients
Curative treatment involves;
Radical surgery
Radical radiotherapy
Radical Surgical Resection
Is the treatment of choice for tumours of the lower two-thirds of the oesophagus provided:
1-The patient is fit for major surgery
2-Preoperative staging tests indicate that the tumour is resectable and there is no metastatic disease.
The principle of surgical treatment
Resection of the tumour with safety margins.
Restoration of the continuty, usually gastro-oesophageal anastomsis
Radical Radiotherapy
Radiotherapy may be a useful alternative to surgery especially in unfit patients.
5year survival 9-19%(average10%) while following surgical treatment 20-35% (20%)
Chemotherapy
Improved after the introduction of newer drugs like cis-platinum.
Chemotherapy never cures the disease
Best results are seen in SCC
Multimodality treatment
Adjuvant radiotherapy either pre- or post- operative
Radiochemotherapy
Palliative Treatment
Simple procedures that will produce worthwhile relief of dysphagia with minimal disturbance to the patient
Intubation
Traction tubes
Pulsion tubes
Traction tubes
Celestin
Pulsion tubes
Atkinson tube
Metal stent
Endoscopic Laser
Used to core a channel through the tumour
Brachytherapy
intraluminal radiation
Carcinoma of the oesophagus
Squamous cell usually affects the upper two-thirds;
adenocarcinoma usually affects the lower third
Common aetiological factors are tobacco and alcohol
(squamous cell) and GORD (adenocarcinoma)
The incidence of adenocarcinoma is increasing
Lymph node involvement is a bad prognostic factor
Dysphagia is the most common presenting symptom, but
is a late feature
Accurate pretreatment staging is essential in patients
thought to be fit to undergo ’curative’ treatment
Oesophageal Motility disorders
Achalasia
Pathology:
Loss of the inhibitory ganglion cells in Auerbach’s plexus.
Aetiology:
Unknown
Neurotropic viruses, Varicella zoster
Trypanosoma Cruzi cause Chagas disease
Incomplete or absent relaxation of the lower oesophageal sphincter and absent peristalsis in the body of oesophagus.
It results in
Retension of food in oesophagus
Dilatation….Megaoesophagus
Clinical features
Is commonest in middle life
Typically presents with dysphagia
Long standing cases…overspill into the trachea at night Retrosternal discomfort
Diagnosis
Endoscopy
Contrast radiology:
Dilated oesophagus
Tapering stricture…bird’s beak
Absent gas bubble
Oesophagial Manometry
Treatment
Forceful dilatation
Disadvantages:
PerforationReflex
Repeated sessions
Heller’s cardiomyotomy
Open Laparotomy
Laparoscopic
Botulinum toxin
Drugs
Calcium channel antagonists
Other oesophageal motility disorders
Cricopharyngeal achalasia
Diffuse oesophageal spasm
Nutcracker oesophagus
Eosinophilic oesophagitis

Oesophageal diverticula
Pulsion diverticula
Traction diverticula
Zenker’s diverticulum (Pharyngeal pouch)
it protrudes posteriorly above the
cricopharyngeal sphincter through the natural weak point (the
dehiscence of Killian) between the oblique and horizontal
(cricopharyngeus) fibres of the inferior pharyngeal constrictor
Symptoms:
Pharyngeal dysphagia
Halitosis
Oesophagial Dysphagia
Diagnosis:
Endoscopy
Barium swallow

Treatment:
Endoscopic: stapler creating diverticulo-oesophagostomyOpen surgery:
Pouch excision
Pouch suspension
Myotomy