Motivation &Substance Abuse
Al Mustansiriya5th and 6th Dec. 2015
Sami Adil
Motivation
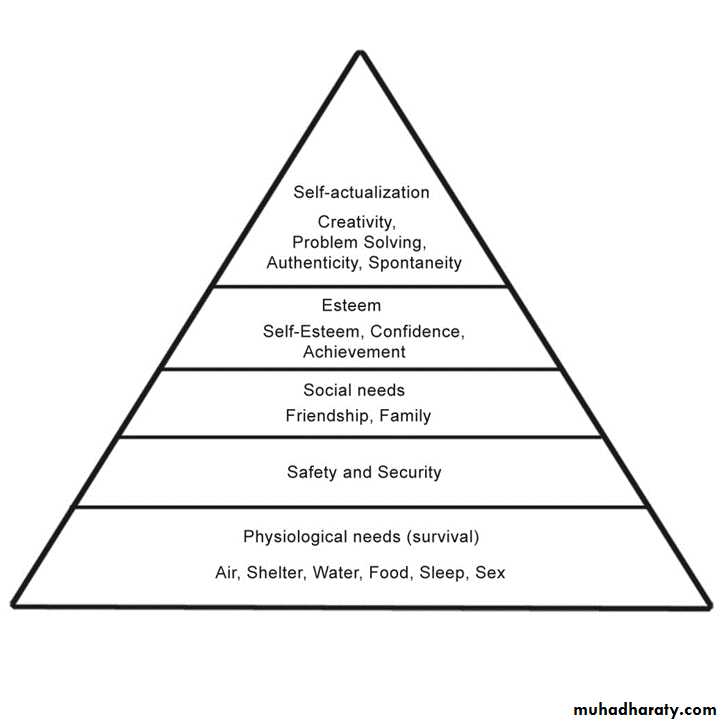
What energize and direct behaviorMost are learned
Arise from two sources: internal drives, and external incentive factors
Hunger, thirst, sex, aggression
• Reward System …. mesolimbic
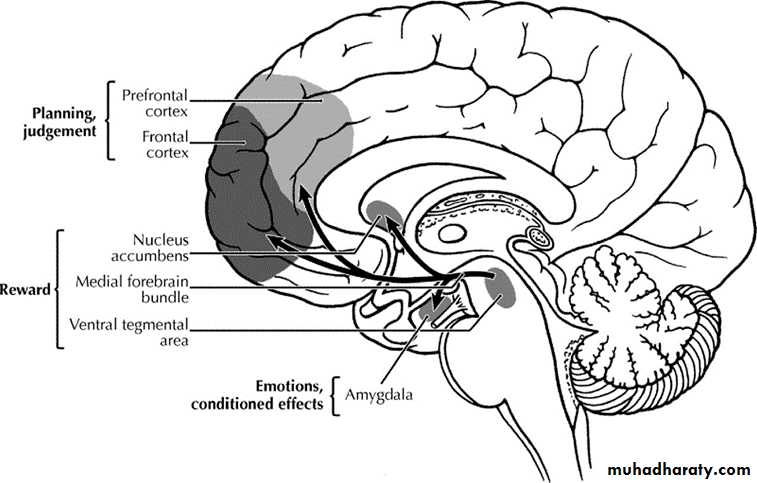
Mesolimbic pathway disturbed in schizophrenia, mania, and depression
Antipsychotic drugs therapeutic effectDeep brain stimulation in depression and Nas
Addiction
Placebo
Homeostasis
• It is the tendency to preserve of a constant internal state and it occurs in all organisms. Homeostasis motivates us sometimes without us understanding it. (e.g.Addison’s …. Develop preference to eat salty )• Addiction and homeostasis (Tolerance and withdrawal).
• Set point of hunger, thirt… hypothalamus
• Complex drives…. Hypothalamus, signals from other body parts, cultural factors (eating.. Anorexia nervosa)


• Most abused substances can be classified as stimulants, sedatives, opioids, or hallucinogens, and related agents.
Substance abuse is a pattern of abnormal substance use that leads to impairment of occupational, physical, or social functioning.
Substance dependence is substance abuse plus withdrawal symptoms, tolerance, or a pattern of repetitive use.
Withdrawal is the development of physical or psychological symptoms after the reduction or cessation of intake of a substance.
Tolerance is the need for increased amounts of the substance to achieve the same positive psychological effect.
Cross-tolerance is the development of tolerance to one substance as the result of using another substance.
Epidemiology differs from a country to another but usually it is more common among young adult males.
Any substance abuse life time prevalence according to the IMHS is 0.9% (1.5% in males, and 0.25 in females) in Iraq. More common in young than older, urban than rural (1).
In study 2014 all over Iraq lifetime prevalence of drug use: Tobacco: (29.0%); Alcohol, (8.6%); Licit drug misuse (2.5%,) and Illicit drug use (0.4%) (2) . This study also found that:
Anabolic steroids are the most widely used licit drug in Iraq followed by bnz & benzhexol. In the North of Iraq, there are concerns of increasing misuse of tramadol.
Cannabis is the most widely used illicit drug, but use of stimulants (Amphitamines and Captagon) in the South of Iraq is present. This finding is consistent with worldwide data, but in Iraq, this gender difference is either particularly great.
Lifetime rates of licit and illicit drug use were higher among younger participants (18-34 years), those with less education (less than primary school) and those who were not working.
Stimulants
DopaminePsychosis with Cocaine -- bug
Cigarette smoking decreases life expectancy more than the use of any other substance.
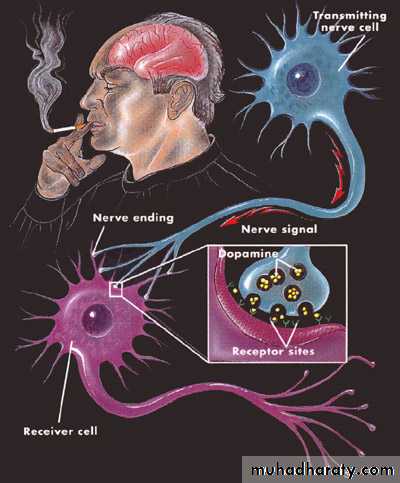

Nicotine
CaffeineAmphetamine
Cocaine
Substances
Effects of Use
Effects of Withdrawal
Psychological
Caffeine & NicotineIncreased alertness and attention span
Mild improvement in mood
Agitation and insomnia
Lethargy
Mild depression of mood
Physical
Decreased appetiteIncreased blood pressure and heart rate (tachycardia)
Increased GIT activity
Increased appetite with slight weight gain
Fatigue
headache
Effects of use
Effects of withdrawal
Amphetamines & Cocaine
Psychological
Significant elevation of mood (lasting only 1 hour with cocaine)
Increased alertness and attention spanAggressiveness, impaired judgment
Psychotic symptoms (e.g., paranoid delusions with amphetamines and formication with cocaine)
Agitation and insomnia
Significant depression of mood
Strong psychological craving (peaking a few days after the last dose)
Irritability
Physical
Loss of appetite and weightPupil dilatation
Increased energy
Tachycardia and other CVS effects which can be life-threatening
Seizures (particularly with cocaine)
Reddening (erythema) of the nose due to "snorting" cocaine
Hypersexuality
Hunger (particularly with amphetamines)
Pupil constriction
Fatigue
SEDATIVES
GABA

أبو الحاجب، أبو الصليب، الدموي
BNZBarbiturates
Alcohol
Substances
Effects of useEffects of withdrawal
Alcohol, Benzodiazepines, & Barbiturates
Psychological
Mild elevation of mood
Decreased anxiety
Somnolence
Behavioral disinhibition
Mild dression of mood
Increased anxiety
Insomnia
Psychotic symptoms (e.g. delusions and formication)
Disorientation
Physical
SedationPoor coordination
Respiratory depression
Tremor
Seizures CVS symptoms, such as tachycardia and hypertension
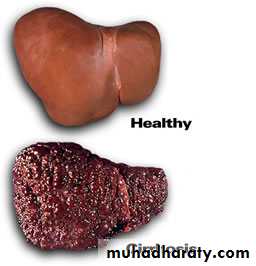
Wernicke and Korsakoff
Delirium TremensOpioids




سيمو، توسيرام
SubstancesEffects of use
Effects of withdrawal
Heroin, Methadone, and Other Opioids
Psychological
Elevation of mood
Relaxation
Somnolence
Depression of mood
Anxiety
Insomnia
Physical
SedationAnalgesia
Respiratory depression (overdose maybe fatal)
Constipation
Pupil constriction (miosis)
Sweating, muscle aches, fever
Rhinorrhea (running nose)
Piloerection (goose bumps)
Yawning
Stomach cramps and diarrhea
Pupil dilatation (mydriasis)
hallucinogens

LSD
Substance
Effects of useEffects of withdrawal
Cannabis, LSD, PCP, Psilocybin, Mescaline
Psychological
Altered perceptual state (auditory and visual hallucinations, alterations of body image, distortions of time and space)
Elevation of mood
Impairment of memory (maybe long-term)
Reduced attention span
"Bad Trips" (panic reactions that may include psychotic symptoms)
"Flashbacks" (a re-experience of the sensations associated with use in the absence of the drug even months after the last dose)
Few if any psychological withdrawal symptoms
Physical
Impairment of complex motor activity
CVS symptomsSweating
Tremor
Nystagmus (PCP)
Few if any physical withdrawal symptoms
أبو الجمجمة، آرتان، باركيزول
CategoryImmediate treatment/detoxification
Extended treatment/maintenance
Caffeine and nicotine
Eliminate or taper from diet
Analgesics to control headache due to withdrawal
Substitute decaffeinated beverage
Nicotine-containing gum, patch or nasal spray
Antidepressants (particularly bupropion)
Support
Hypnosis to prevent smoking
Amphetamines and cocaine
Benzodiazepines to decrease agitation
Antipsychotics to tr. Psychosis
Medical and psychological support
Education for initiation and maintenance of abstinence
Sedative (alcohol, BNZ, Barbiturates)
Hospitalization
Flumazenil to reverse affects of BNZ
Use of long acting BNZ in decreasing doses (detoxification)
Specifically for alcohol: thiamine, restoration of nutritional state.
Education
Specifically for alcohol: disulfiram, naloxone, naltrexone, acamprosate, psychotherapy, and Alcoholic Anonymous AA or other peer support groups
Opioids
Hospitalization and naloxone for overdose
Clonidine to stabilize ANS during withdrawal
Substitution of long-acting opioids (methadone) in decreasing doses to decrease withdrawal symptoms (detoxification)
Methadone, LAAM or buprinorphine maintenance program
Naloxone, naltrexone (or buprenorphine) used prophylactically to block the effects of abused opioids
Narcotic Anonymous or other peer support groups
Hallucinogens
Calming or "talking down" the patient
BNZ to decrease agitation
Antipsychotics to tr psychosis
Education for initiation and maintenance of abstinence
THANK YOU