BEGNIN DISEASE OF THE CERVIX & UTERUS
A- absence1- complete
2- in complete
Complete absence of the uterus result when the Mullerian duct fail to develop, usually associated with sex chromosomes' abnormalities .i.e. no tube and no uterus and no upper vagina
Incomplete , part of Mullerian duct present .e.g. just the tube and fimbriated end called Plica transversals.
B- hypoplasia
Error in antenatal or postnatal developmenta- either as nodules or the uterus as asmall hallow organ .
b- or it is essentially normal in shape but it is small in dimensions i.e. infantile proportion between the uterus and the cervix .i.e. longer cervix so either hypo plastic uteri ,rudimentary or infantile
Causes:
1- chromosomal error , her the uterus incompletely formed or incapable to respond postnataly to the stimulation of estrogen2- Failure of adrenal plus ovaries to supply estrogen to stimulate the uterus
3- Or inhibition of estrogen effects on Mullerian duct
Clinical features:
1- Primary amenorrhea
2- hypoplasia
3- late menarche
4- abortion
5- 2nd amenorrhea which is usually due to uterine atrophy not due to hypertrophy
6- infertility
Diagnosis depend on :
subnormal menstrual cycle , small uterine cavity , thin endometriumtreatment : By estrogen (ethinyl estradiol) 0.05 × 3 for 3 weeks then one week free for 3- 6 months (if amenorrheaic)
If she is menstruating : give estrogen in the follicular phase of the cycle only and one 1/3 of the above dose , If NO RESPONSE mean TARGET ORGAN DEFECT
If there is response and regress after stop estrogen ,mean it is due to deficiency of estrogen
SO ESTEROGEN IS USUFULE FOR DIAGNOSTIC AND THREPUTIC PROCEDURE
C – Cochleat uterus: ( ante flection of uterus),or
( Retroflection) the uterus C shapedD– Displacement of the of the uterus
Upwards displacement of the uterus . Lateral. Forwards displacement / by adjacent
Structure
E– Retroversion : Frequency 15%
Causes
1- developmental (not congenital),usually shallow anterior vaginal fornix, the anterior vaginal wall and cervix appear to be almost continuous2- Acquired:
traumatic : sudden physical movement
prolapse: change of the axis of uterus in the direction of the vagina
tumor and adhesion: tumor in front of the uterus ͢ pushing
or adhesion ͢ pulling like endometriosis
3- Puerperal : axial in 3– 6 weeks then become anteverted
Symptoms of retroversion
1- The mobile one is symptomless2- +ve symptoms , if is fixed ,due to the disease that cause fixation and displacement
3- spasmodic dysmenorrhea
4- low backache
5- Rectal symptoms
6- dyspareunia
7- infertility
8- incarceration
Physical signs
Cx pointed for wards
the body can be felt in the pouch /Tr :tr the cause
Treatment also
By peccaryby surgery / Baldy Webster, Ventro suspension
F – Inversion of the uterus :
turn inside out through the cervix it varies between DIMPLING of the fundus to the involvement of the whole uterus and cervix
1- Acute inversion
2- chronic inversion
a- puerperal
b- senile inversion
c- due pedunculated fibroid ( sub mucosal fibroid )
The CERVIX
Differentiation of the cervix from the body of the uterus is recognizable by the tenth week of gestation and clearly separated from the vagina by 20 weeks of gestationDevelopmental malformation
A – Incomplete canalization usually of Mullerian ducts
1- congenital atresia :it is rare but if it is present usually associated with absence of the lower vagina
2- Conical cervix and pinhole os
occasionally it is so conical ,or the external os appear so small ie pinhole os and the cervix tends to be long and narrow
3- congenital hypertrophy of the cervix
actually it is developmental rather than congenital , it affect the vaginal portion rather than the supravaginal portion the diagnosis made only in nulliparaous women , it may cause subfertility , discomfort during straining and during coitus
4 -- Cervical incompetence
a- congenitalb- acquired
c- functional
Diagnosis before pregnancy ,after pregnancy
timing of cereclage
Types of cereclage
Indication of removal :…………….
5– Laceration of the cervix:
a – obstetrical injuries
1- usual laceration during labor
2- pathological tearing
Forceps, ventose, breech extractions before the Cx is fully dilated, instrumental dilatation of the Cx ,precipitated labor,
Unilateral, Bilateral , multiple tear ,stellate
6- DETACHMENT OF PART OF THE CERVIX
that the anterior lip become imprisoned /. / the presenting part and symphysis pubis, annular detachment in case Cx dystocia5- cervico vaginal fistula
7- surgical injuries , D&C , Cone biopsy, Amputation of the Cx
INFECTION
CervicitisA- acute
Gonococcal, puerperal in origin ,chlamydial, trichmonal
The infection may spread to the base of broad ligament
Macroscopically :
1- red Cx
2- congested
3- swollen
4- Profuse purulent exudate some time white &sometimes yellowish
Microscopically :
1- there is intense polymorph nuclear infiltration of the mucosa & the under lying tissue
2- Hyperemia or less edema
3- the gland Lumina maybe distended with exudate consisting of a large number of dead leukocytes and desquamated cells and mucus .
Clinical symptoms:
1- leucorrhea, purulent in acute stage in gonorrheal type2- in acute stage there is urethritis and vaginal irritability
3- The Cx tender on touch or movement
4- there may be a slight elevation if body tempture with a sensation of congestion in the vaginal region ,combined with urinary irritability and burning if there is urethritis
Diagnosis:
A– Inspection by mean of speculum1- Cx , red irritated , friable
2- the Os' may be surrounded by reddish, granular halo
3- the epithelium of the Paris vanginals may present tiny abrasions like area due to macerating effect of the discharge
B- Gram stained smears of cervical discharge
1- For intracellular gram negative diplococci
2- Direct examination for TV
3- Culture and sensitivity
Treatment : according to the cause and C&S
B- Chronic cervicitis:
Etiology :*It present in 35- 85% of women
*It caused by vaginal organism becoming pathogenic
Puerperal cervicitis which often associated with laceration of the cervix ͢ chronic cellulitis
Gonococcal
Chlamydia
Chronic &repeated injury
The cervix looks red, congested ,swollen +profuse purulent exudate , varies from white to yellow
Clinically :
+ve leucorrhea , that become purulent if it is due to gonococcal infection
Cervical tenderness on touch ,on movement ,vaginal congestion ,urinary irritability ,congestive dysmenorrhea ,backache, deep seated dyspareunia, post coital bleeding,
Infertility due to change in the physical character of the cervical plug and from decrease in PH of vaginal
D . D :
CA cervix , so cytological assessment by Pap, colposcopy, examination,Treatment:
Antibiotic specially for gonococcal infection
Thermal, cryosurgery
Viral cervicitis:
1- herpes
consist of oedema, vesicles, ulcer, in extremely cases a granulomatous lesion
It self limited and end within 2-3 weeks
The diagnosis based on the history , cultures, the gross appearance of the lesion , cytology
2- Condylomata accuminata
rarely seen grossly on the cervix ,appear as a pale white , raised irregular plaque on the cervix , it is the cause of cervical dysplasia
can be treated by 20% podophllin or by fulguration or excision
3- HPVThey are flatter and moister than the typical genital warts (condylomata acuminata) seen on the vulva and perianal skin. In fact, they often are invisible to the naked eye, becoming visible only after application of a dilute solution of acetic acid (acetowhite epithelium) or by colposcopic examination (white epithelium, mosaicism, and coarse punctation). More than 65 types of HPV have been identified. Benign lesions of the cervix are associated with types 6, 11, 42, 43, 44, 53, 54, and 55, whereas types 16, 18, 31, 33, 35, 39, 45, and 56 are more often found in association with cervical intraepithelial neoplasia and invasive cancers.Approximately one-third of women with HPV infection have coexistent cervicitis caused by other organisms. The presence of cervicitis does not significantly affect the clinical course of HPV lesions.
Mycoplasmal, chlamydia, associated with infertility mainly due to salpengitis
T. B. :
IT is rare lesion usually secondary to T.B. In the tube and uterus
it maybe hyperplastic or ulcerative lesion , presented as mucoperulent discharge
SHOULD BE DIFFERENCIATED FROM CA CERVIX
Cervical stenosis
Causedatrophy
Scaring
T.B
MALIGNANCY
Conization, cauterization ,cryo therapy ,radiation
IT may lead to :
dysmenorrhea , hematometra , pyometra, ASYMTOMATIC IN CASE OF ATROPHY
Cervical ectropian
Bilateral cervical laceration or one side which may be small or large , it may extend to the vaginal fornixThe laceration cause disruption of circular fibro muscular fibers and leaving the longitudinal fibers of external cervical muscle free to act unopposed leading to curl the lips of the cervix upward and outwards lead to ectropian
Clinical features:
1- red –looking endocervix , due to columnar epithelium
2- associated with excessive mucus secretion
3- post coital bleeding
Management:
1- pap smear
2- stop contraceptive
3- thermal therapy , using a metal thermal probe , that heats the tissue to around 100 C, that destroying the epithelium to a depth of
3—4 mm.

Cervical ulcers
1- bacterial:a- T.B
B- SYPLITIC
2- Traumatic
3- malignant:
Diagnosis by swabs+ biopsy
Nabothian follicle:
squamous cells metaplasia of transformational zone cause roofing of glands within columnar epithelium leading to formation of small cysts fill with mucus and becomes visible on ectocervix ,IT IS OF NO PATHOLOGICAL SIGNIFICANCE
Cervical polyp
Usually mucosal polypIt may be a distension cyst of cervical ,they are multiple , small, cherry red, usually arise from the cervical canal ,contained a fibrous core and covered by columnar epithelium ,causing excessive vaginal discharge, mucoid , post coital bleeding, infection
Treated by excision + D&C and send for histopathology
BENGNIN DISORDERS OF T HE UTERUS
Absence :
A- Complete : when the Mullerian ducts fails to develop usually associated with sex chromosomes abnormalities i.e. no tube no uterus no upper vagina
B– incomplete : that part of Mullarian duct present ,e.g. just the tube &fimbriated end called Plica transversalis
Hypoplasia:
Error in antenatal or postnatal development1- either as nodule or the uterus as small hollow organ
2- or it is in infantile proportion /./ the uterus and cervix
CAUSES:
chromosomal error ͢ the uterus incompletely formed or incapable to respond postnatally to estrogen
2- failure of the adrenal and the ovaries to supply estrogen to stimulate the uterus at the time of ovulation like in case of hypo gonadotrophic hypogonadism
3- receptor defect
Presentation:
1- primary amenorrhea
2- hypo menorrhea
3- late menarche
4- abortion
5- secondary amenorrhea duo to uterine atrophy not to hypoplasia
6-infertility
DIAGNOSIS:
ULTRA SOUND ,MRI , and on menstrual history
Treatment: depend on presentation
Ante flexion
The cervix is more conical ,narrower than normal , the cervix directed up wards or directed to the left or to the right ,it is regarded as mal development rather than under development , it cause spasmodic dysmenorrheaDysparuinea
Subfertility
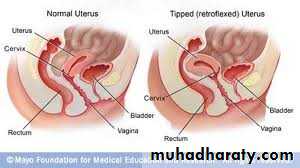
RETROVERSION
Either maldevelopment or pathological that cause fixed retroversion or mobile typeSacculation of uterus this is occur in gravid uterus
Inversion of the uterus
Acute
Chronic :
puerperal: incomplete inversion that is overlooked in the 3rd stage ,cause vaginal discharge low backache ,chronic pelvic pain
senile especially if the cervix has previously been amputated at high level that lead to cervical a tony
due to pedunculated tumor
Endometritis
A- acute/ apart from infections at operations and by instrumentation it is eitherpuerperal
gonococcal
The regrowth of new surface endometrium during each cycle prevents the persistence of any infection which not deep seated can be treated accordingly
B- chronic :
T.B
Senile
other causes
It is a rare disease between the menarche and menopause because of regrowth of endometrium
It is caused when the uterus is permanently injured or when there is a chance for its continuously infected like :
foreign body
Malignant disease of the uterus
Infected polyp
Retained gestational products
Chronic salpingio-oopheritis
Pelvic cellulitis from radiation
Endometrial burn due to radiation
Microscopically there is large collection of plasma cells and f
Clinical features :
1- purulent discharge from the uterus
2- menorrhagia
IN ANY SIGNS OF INFCETION ---- SEND FOR CULTURE TO EXCLUD T.B
Treatment :
find the cause and treat accordingly
If there is wide spread infection then treat by hysterectomy
Senile endometritis :
The endometrium lose its resistance ,and not shed repeatedly
It may be associated with senile vaginitis
The endometrium infiltrated by macrophages known as foam cells the epithelium become destroyed lead to granulation tissue that lead to pus exudation if is collect in the cavity lead to pyomertra , because the cervix is narrow due to senility atrophied myometrium
The uterus enlarge and become thin , pyrometera may cause squamous metaplasia or rarely ruptured spontaneously :
Clinical features:
1- purulent very offensive post menopausal discharge , some times bloody stained
2- Sometime intermittent discharge
3- uterus is enlarge
D.D:
1- Ca of the uterus
2- if there is pyometra then DO dilatation of the cervix that lead to drainage of pus+ antibiotics for 1-2 weeks and then do curettage for DD
Treatment : if the patient fit for surgery then hysterectomy after exclusion of Ca
UTERINE POLYPS
1- endometrial polyps
usually multiple , and may be apart of hyperplastic endometrium, at menopause are single or few in number ,
Pathology :
small, pink ,pale projecting from the endometrium ,some time has long stalk that make it projecting through the cervix or the vulva , atypical cellular changes or squamous metaplasia can occur ,adenocarcinoma can occur also
2- fibroid polyp :
sub mucosal fibroids can protrude in to the cavity or pass through the cervix into the vagina, its surface covered by endometrium ,it cause spasmodic dysmenorrhea ,menorrhagia ,
3- Adenomayomatous polyp
Contain smooth muscle + endometrial elements
Usually coexist with adenomyosis ,causing heavy menses but regular, cramping , some time causing intermenstrual spotting ,malignant changes can occur with it
Placental polyp:
It is rare ,due to organization of small retained pieces of placental tissue, it cause intermenstrual bleeding ,it may cause sever hemorrhage on removal , treated by excision , send for biopsy

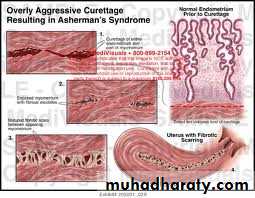
Asherman ΄s syndrome
When there is endometrial damage to endometrium ,the whole thickness , i.e. beyond the basal layer ,caused by :1- excessive curettage for retained products , after miscarriage , for 2ndry PPH
2- T.B ,schistosomasis
3- ENDOMETRIAL RESCTION( ABLATION)
It cause : it cause fibrosis and adhesion
Hypo menorrhea, amenorrhea, infertility
Treatment by :
Resection by hysteroscopy + inert IUCD+ HRT