1
Adrenergic Receptor Antagonist (Blockers)
α-Blockers
Because α -agonists cause vasoconstriction and raise blood pressure, α -
blockers should be therapeutically used as antihypertensive agents. Unlike
the β-blockers, which bear clear structural similarities to the adrenergic
agonists NE and
E, the α -blockers consist of several compounds of diverse
chemical structure that have little resemblance to the α-agonists.
Nonselective α - Blockers
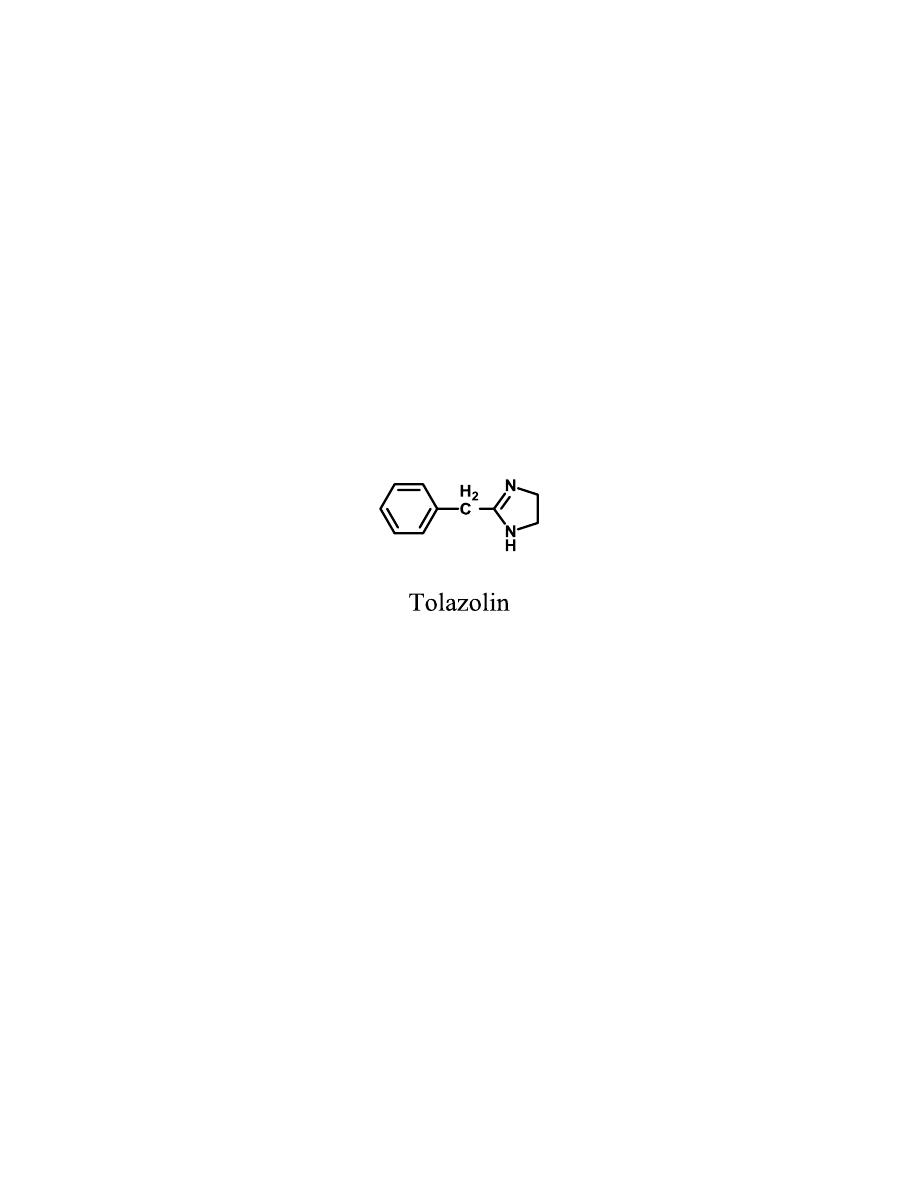
Tolazoline
and phentolamine
They are imidazolines. The structure of tolazoline is similar to the
imidazoline α
1
-agonists, but does not have the lipophilic substituents
required for agonist activity. The type of group attached to the imidazoline
ring thus dictates whether an imidazoline is an agonist or a blocker.
Tolazoline is used in persistent pulmonary hypertension of the newborn
when supportive measures are not successful.
Irreversible α – Blockers
The produce prolonged adrenergic blockade by
long-lasting, irreversible α -
receptor blockade.
The initial step involves the formation of an intermediate aziridinium ion.
The positively charged aziridinium ion electrophile then reacts with a
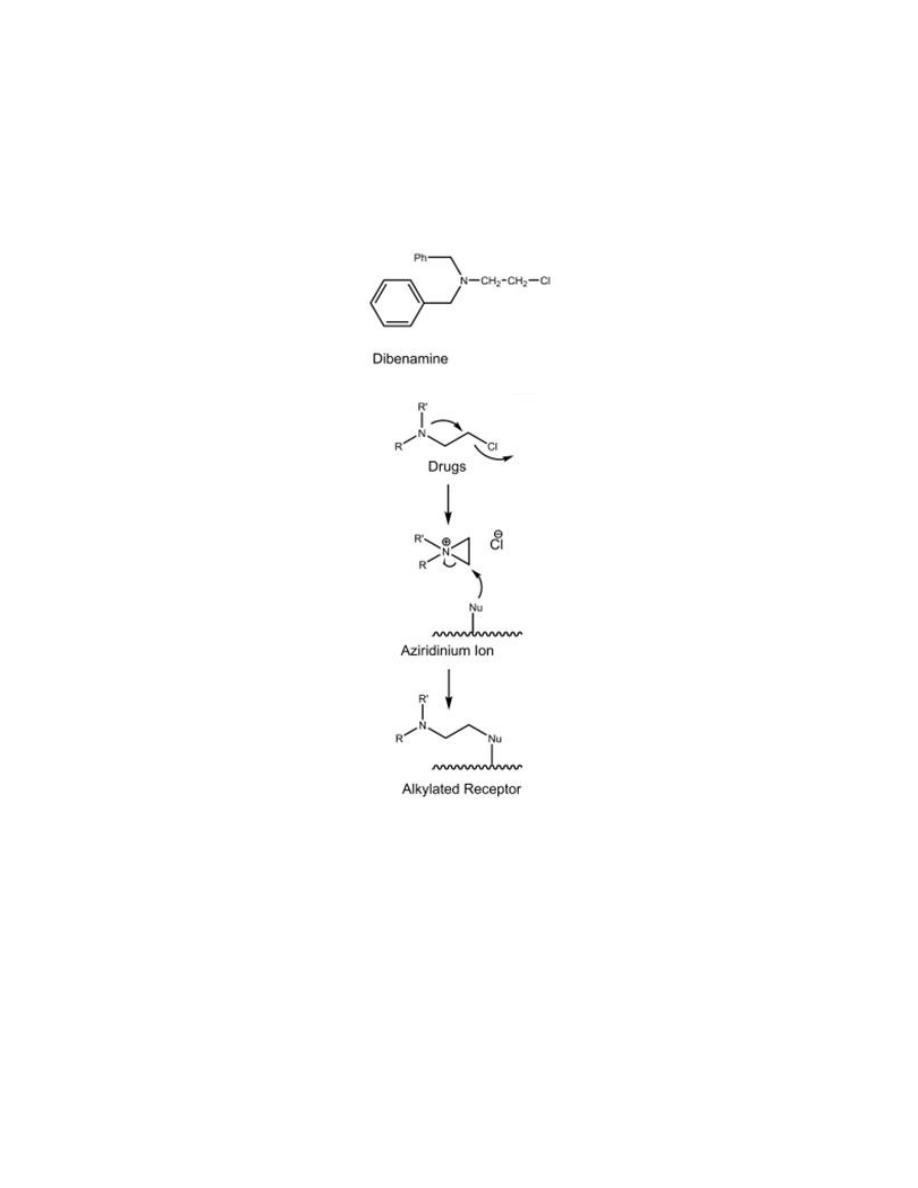
2
nucleophilic group on the α-receptor resulting in the formation of a covalent
bond between the drug and the receptor.
Unfortunately, these nonselective drugs alkylate not only α-receptors but
also other biomolecules, leading to their toxicity.
The onset of action is slow, but the effects of a single dose of drug may last
3 to 4 days, because new receptors must be made to replace those that have
been inhibited irreversibly.
Selective α
1
- Blockers
Prazosin,
Alfuzosin
, terazosin, Tamsulosin and doxazosin
Structurally, these agents consist of three components: the quinazoline ring,
the piperazine ring, and the acyl moiety.
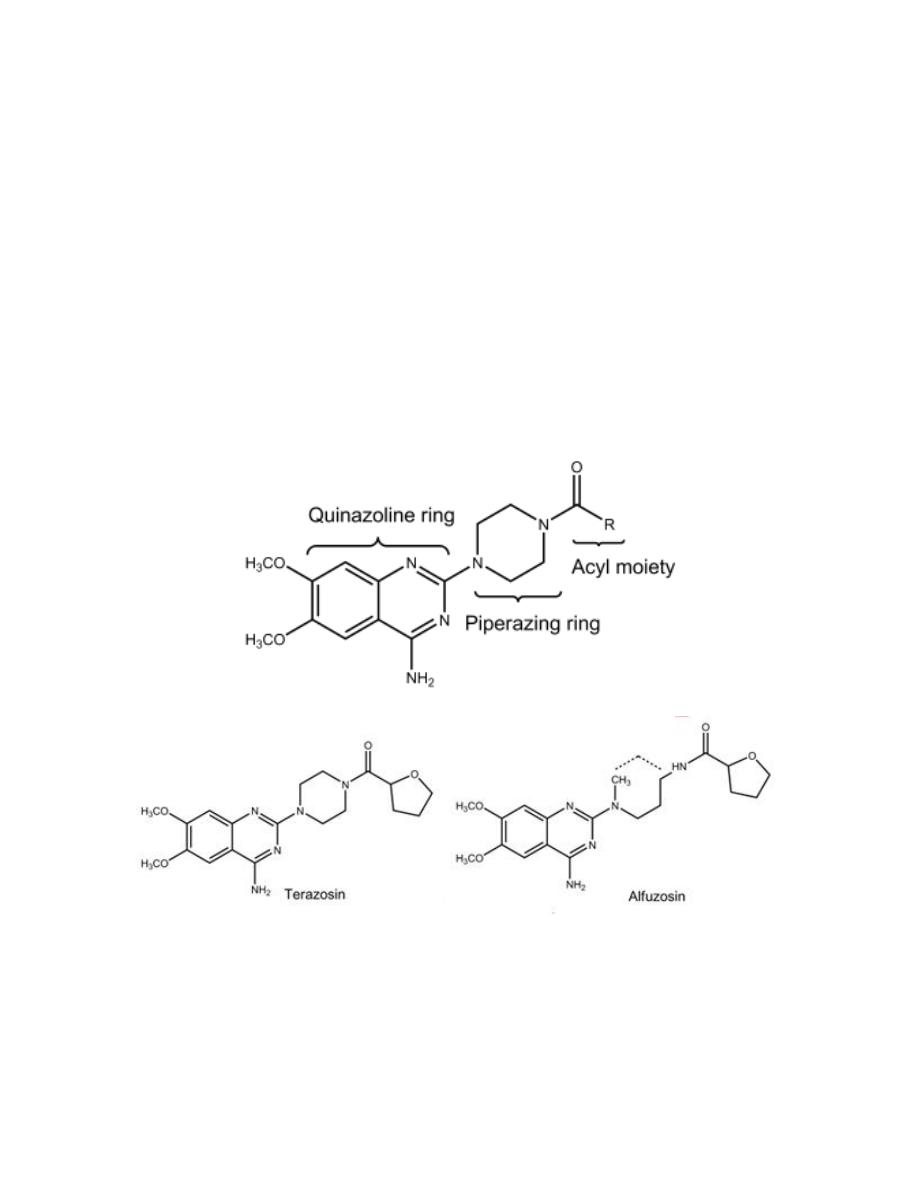
3
•
The 4-amino group on the quinazoline ring is very important for α
1
-
receptor affinity.
•
The piperazine moiety attached to the quinazoline ring can be replaced
with other heterocyclic moieties (e.g., piperidine moiety) without loss of
affinity.
•
The nature of the acyl group has a significant effect on the
pharmacokinetic properties.
Clinically they are used as antihypertensive and for BPH.
Selective α
2
- Blockers
The isomeric alkaloids which are known as the yohimbanes exhibit different
degrees of selectivity toward the α
1
- and α
2
-receptors, depending on their
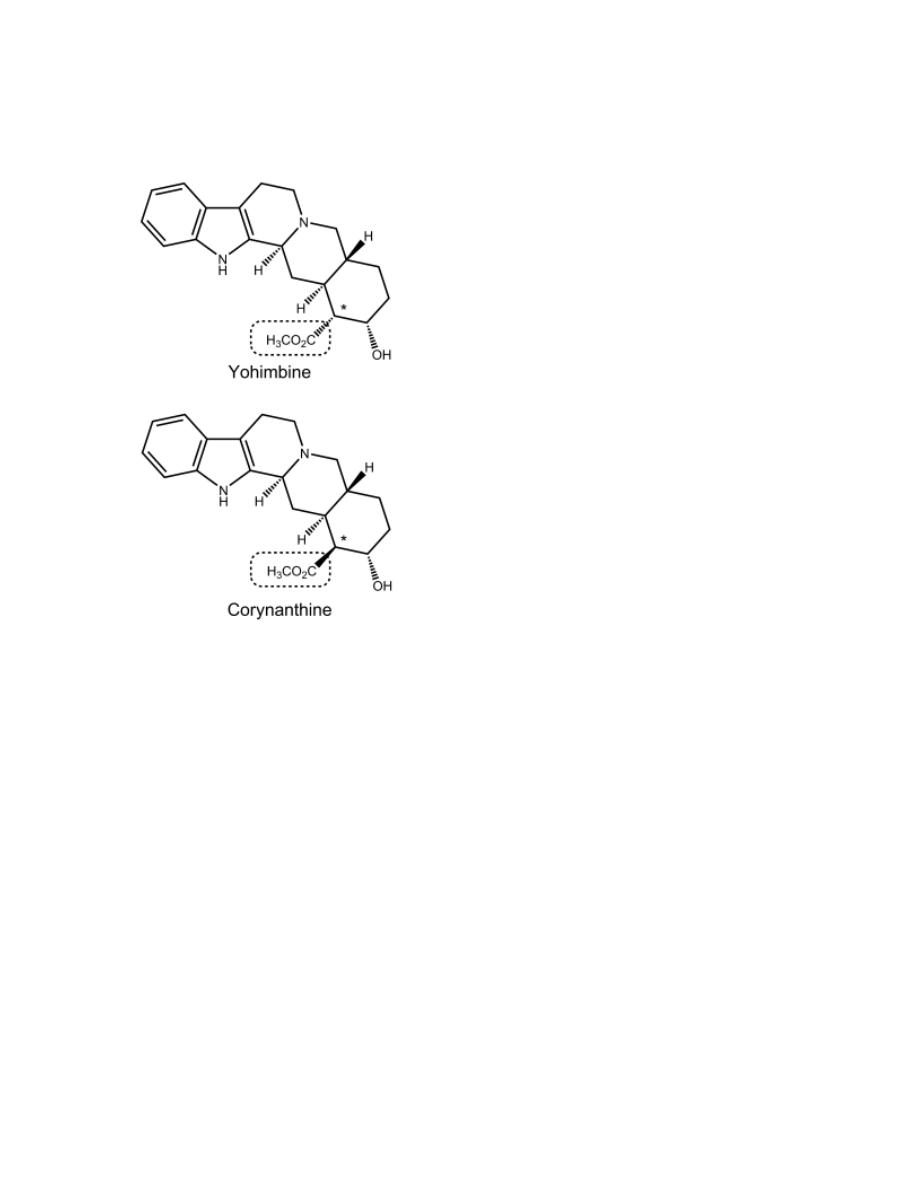
4
stereochemistry. For example, yohimbine is a
selective α
2
-blocker, whereas
corynanthine is a selective α
1
-blocker.
β-Blockers
Structure–Activity Relationships
β-Blockers are among the most widely employed antihypertensives and are
also considered the first-line treatment for glaucoma.
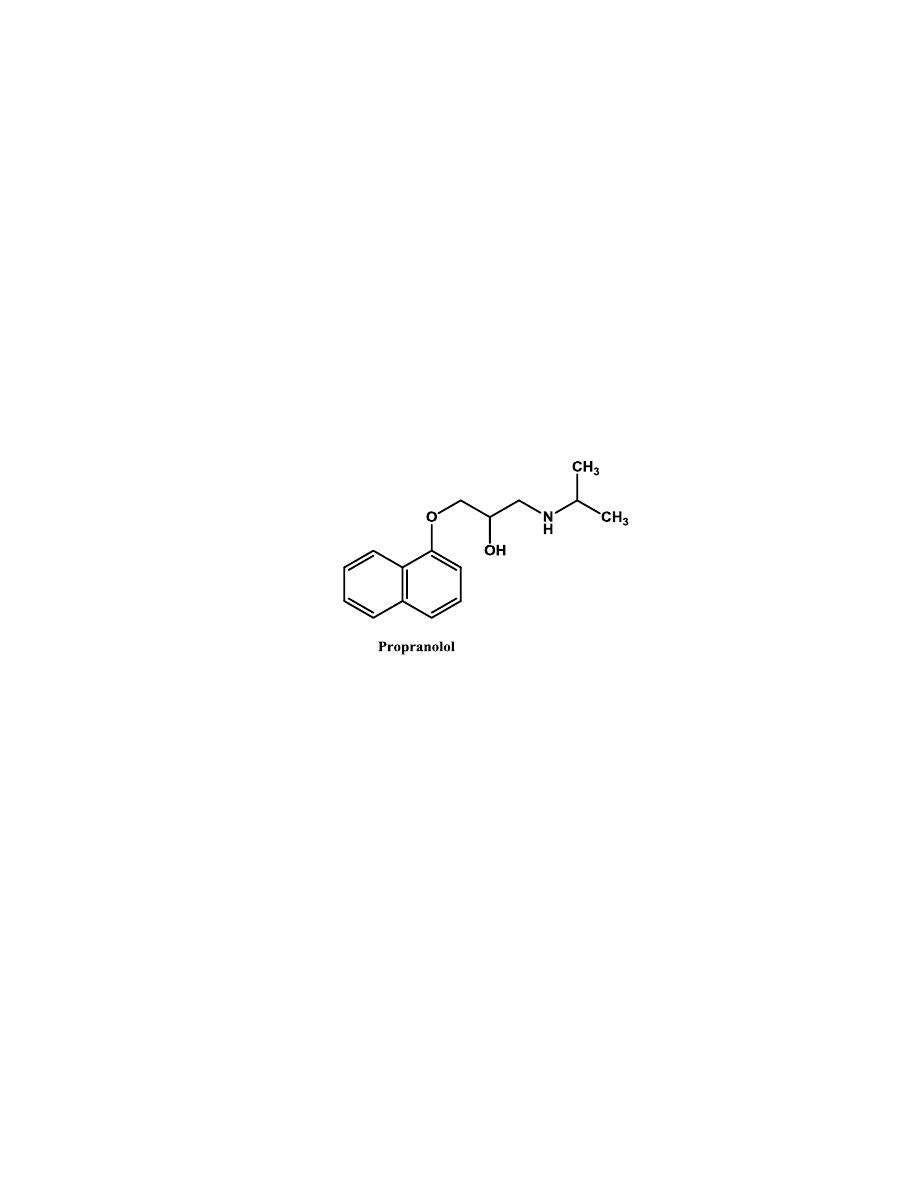
1- Most
of β -blockers are in the chemical class of
aryloxypropanolamines.
2- The aryl group also affects the absorption, excretion, and metabolism
of the β –blockers.
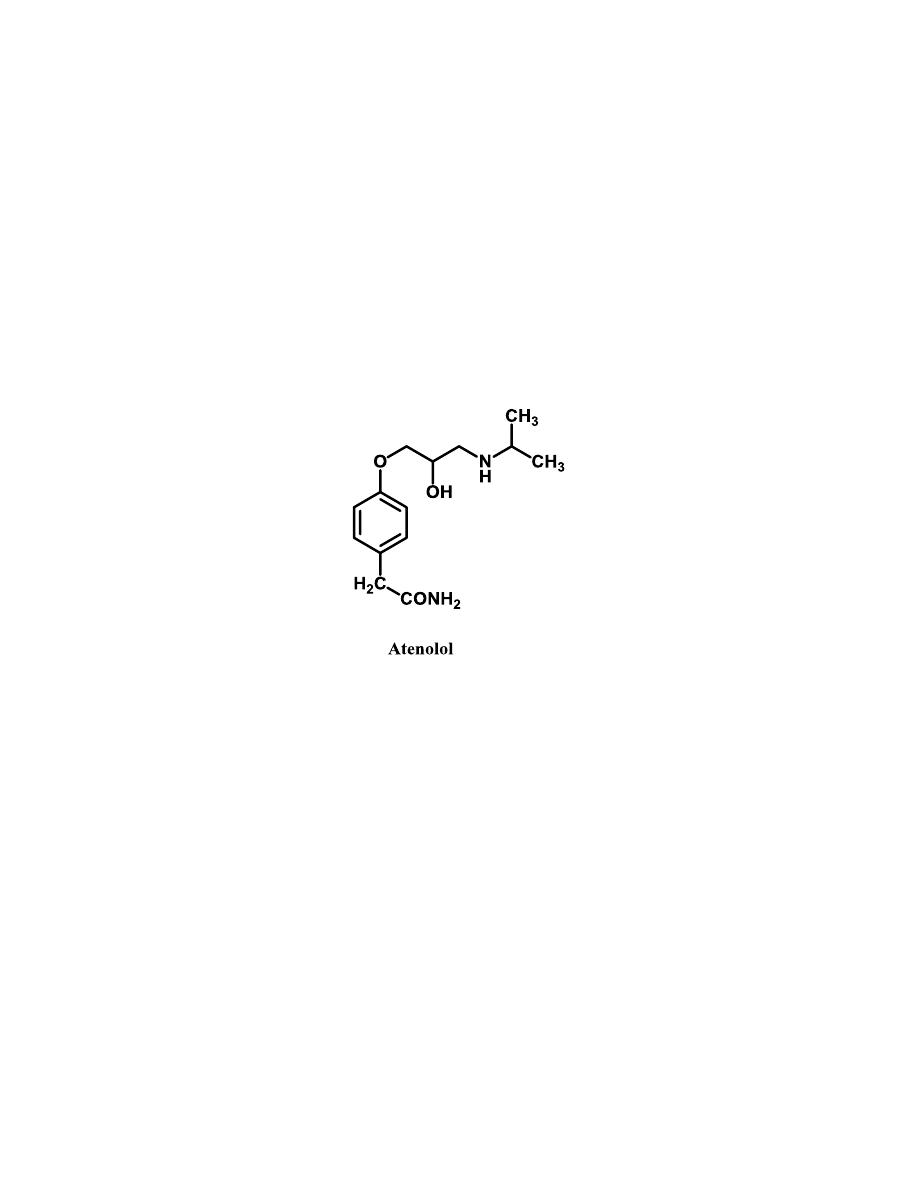
3- One common structural feature of many cardioselective β –blockers
(β
1
–blockers) is the presence of a para-substituent of sufficient size
on the aromatic ring along with the absence of meta-substituents.
5
4- Like β -agonists, β -directing tert-butyl and isopropyl groups, are
normally found on the amino function of the aryloxypropanolamine β-
blockers. It must be a secondary amine for optimal activity.
5- The β -OH-substituted carbon must be in the S absolute configuration
for maximal β-blocking activity.
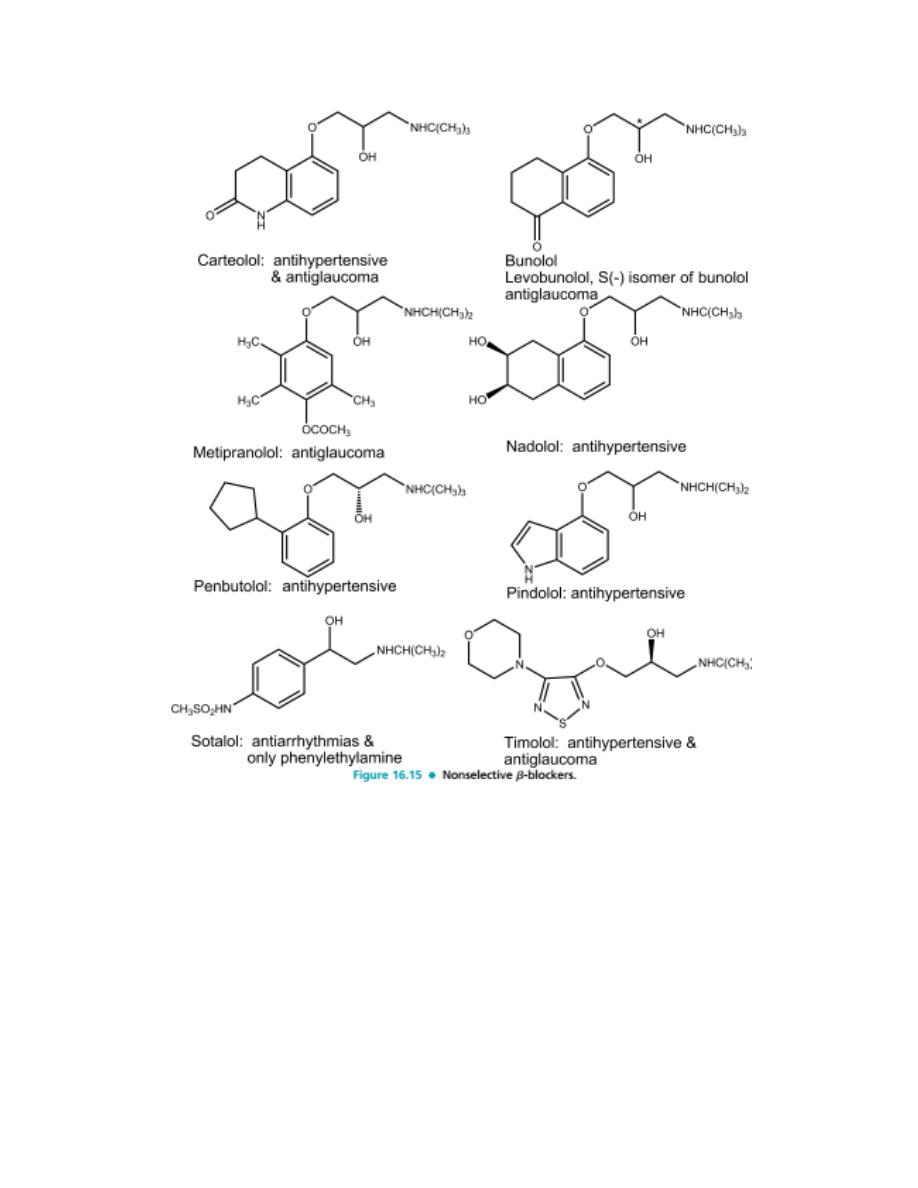
Nonselective β
-
Blockers (First Generation)
Because they exhibit no selectivity for β
1
-receptors, they are
contraindicated in the presence of conditions such as asthma and
bronchitis.
β
1
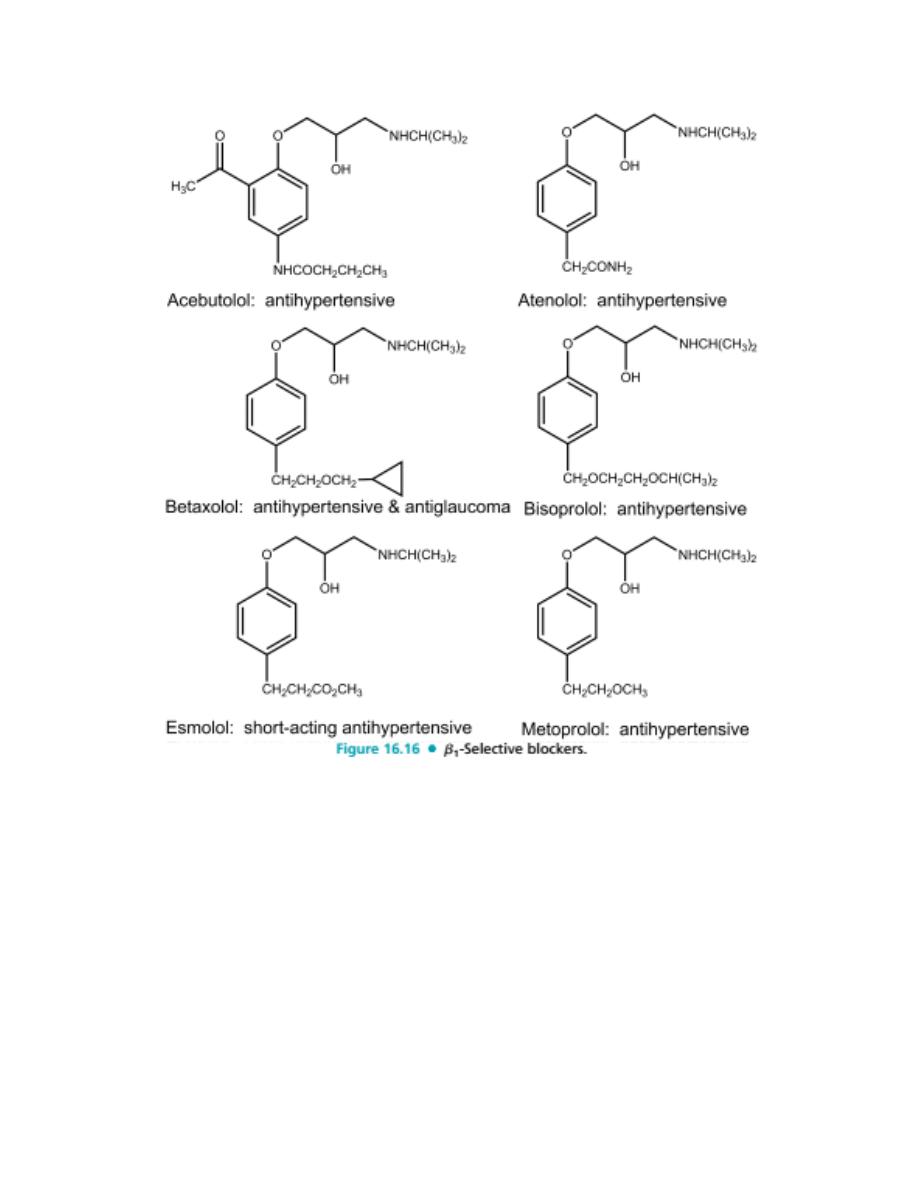
- Selective Blockers (Second Generation)
Cardioselective β
1
-blockers are drugs that have a greater affinity for the β
1
-
receptors of the heart than for β
2
-receptors in other tissues. Such
cardioselective agents should provide two important therapeutic advantages.
The first advantage should be the lack of a blocking effect on the β
2
-
receptors in the bronchi. Theoretically, this would make β
1
-blockers safe for
use in patients who have bronchitis or bronchial asthma.
The second advantage should be the absence of blockade of the vascular β
2
-
receptors. This would be expected to reduce or eliminate the increase in
peripheral resistance that sometimes occurs after the administration of
nonselective β-blockers.
6
Unfortunately, cardioselectivity is usually observed with β
1
-blockers at only
relatively low doses. At normal therapeutic doses, much of the selectivity is
lost.
All of these agents except esmolol are indicated for the treatment of
hypertension.
Atenolol and metoprolol are also approved for use in treating angina pectoris
and in therapy following myocardial infarction. Betaxolol is the only β
1
-
selective blocker indicated for the treatment of glaucoma. Only acebutolol
possesses ISA.
β- Blockers With α
1
-Antagonist Activity (Third Generation)
Labetalol
A phenylethanolamine derivative, is representative of a class of drugs that
act as competitive blockers at α
1
-, β
1
-, and β
2
-receptors. It is a more potent α-
blocker than β-blocker. It is used clinically in treating hypertension.
The rationale for its use in the management of hypertension is that its α-
receptor–blocking effects produce vasodilation and its β-receptor–blocking
effects prevent the reflex tachycardia usually associated with vasodilation.
Carvedilol
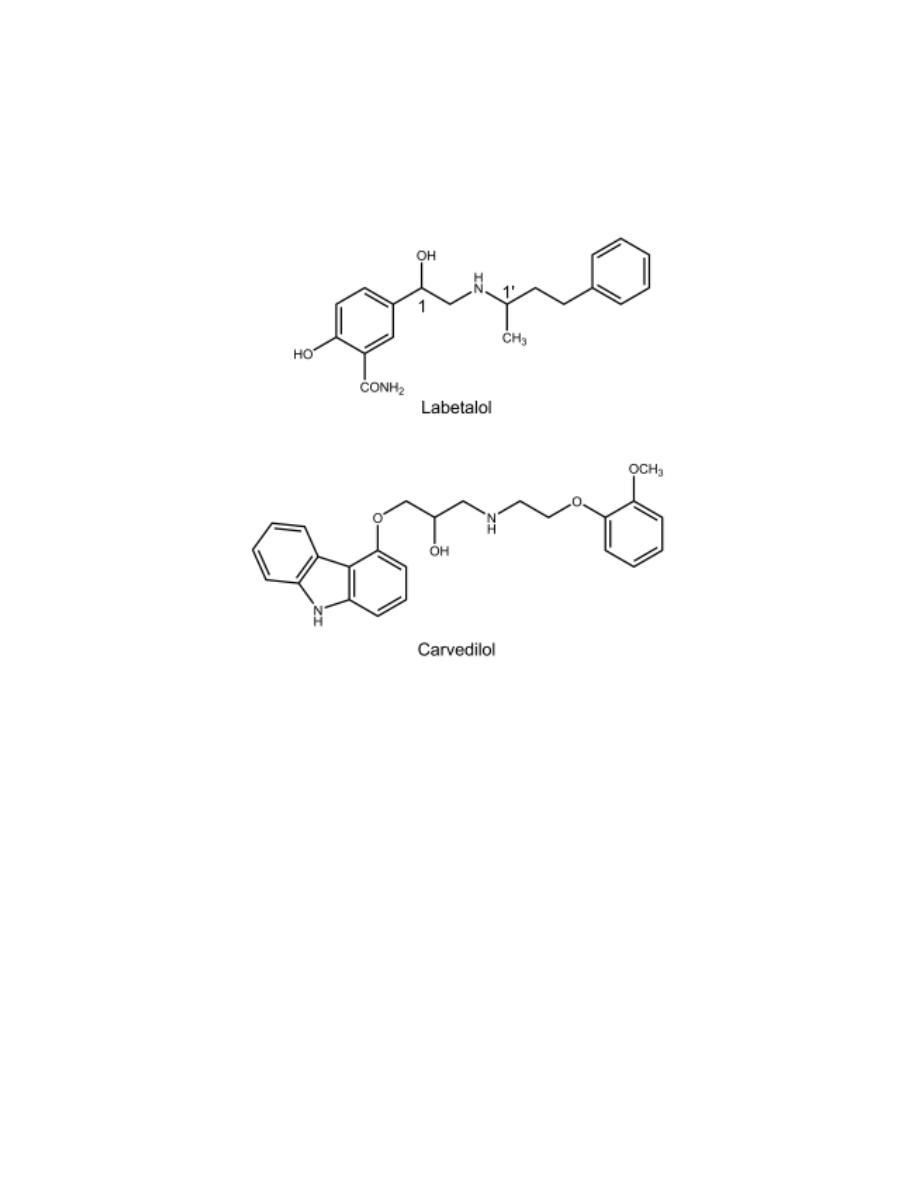
7
It is a β-blocker that possesses α
1
-blocking activity. Only the (S) enantiomer
possesses the β-blocking activity, although both enantiomers are blockers of
the α
1
-receptor. Its β -blocking activity is more than itsα-blocking activity.
It is used in treating hypertension and congestive heart failure.
8
9