Urea Cycle
• A• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Urea is synthesized in the liver and transported to the kidney for
excretion in urine. Urea cycle is the first metabolic cycle Urea
synthesis is a five steps with five distinct enzymes.
The first two steps are mitochondrial , while the rest are localized
in the cytoplasm.
The urea cycle:
Detoxifies ammonium ion from amino acid degradation.
Converts ammonium ion to urea in the liver.
O
||
H2N—C—NH2 urea
• A
• m• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Provides 25-30 g urea daily for urine formation in the kidneys.
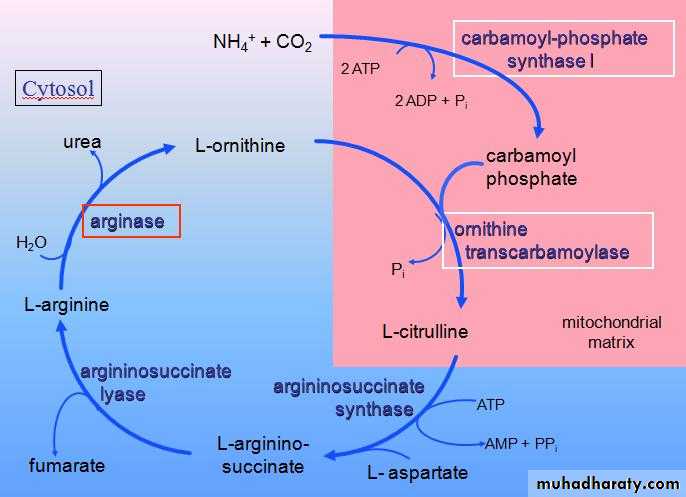
First step
Synthesis of carbamyl phosphate by condensation of NH3 with CO2,consuming ATP,irreversable, catalyzed by carbamyl phosphate synthease
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Second step
Formation of citrulline from CP and ornithine by the enzyme ornithine transcarbamylase . Ornithine and citrulline are basic amino acid.
Ornithine
Citrulline
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Citrulline
Aspartic acid
argininosuccinate
Third step
Synthesis of argininosucinate by condensation of citrulline with aspartic acid
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Argininosuccinate
Fumarate
Ariginine
Fourth step
Cleavage of argininosuccinate by argininosuccinase enzyme into fumarte and arginine. Arginine is the immediate precurrsor for urea .Fumarate provide a connecting link with TCA cycle.
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Cycle can be repeated
Fifth step
Formation of urea . Arginase cleaves arginine to
Orinithine and urea occurs almost exclusively in the liver.
Arginine
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
•
• A
• m• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Urea cycle is linked with TCA cycle in two different ways:
1. The production of fumarate in urea cycle is the most important integrating point with TCA Cycle.
Fumarate H2O malate oxid oxaloacetate which enter TCA cycle.Oxaloacetate undergoes transamination to produce aspartate which enter urea cycle .
2 .TCA cycle is important metabolic pathways for the complete oxidation of various metabolite to CO2+H2O. The CO2 liberated in TCA cycle can be utilized in urea cycle.
Integration between urea cycle and TCA cycle:
• A
• m• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Fate of Urea
Urea diffuse from the liver and transported in the blood to the kidney ,filtered and excreted in the urine in about 25-30 g daily.
A portion of urea diffuse from the kidney to the intestine where it is cleaved to CO2+ NH3 by bacteria Urease enzyme.
This ammonia is partly lost in faeces and the remaining is reabsorbed into the blood..
.
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Fate of Urea
.
In Patient with kidney failure ,blood urea level elevated ,there will be greater shift of urea to the intestine ,due to the action of bacterial urease on this large amount of urea the intestine becomes a important source of ammonia contributing to hyperammonemia seen in these patients (Oral Neomycin)
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Interaction of Urea Cycle and Citric Acid Cycle via Aspartate-Argininosuccinate shunt
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Regulation of the urea cycle
N-Acetylglutamate is an essential activator of carbamyl phospate synthetase- the rate limiting step in urea cycle. N- Acetylglutamate is synthesized from acetyl CoA and glutamate by N-acetylglutamate synthase in a reaction for which arginine is an activator.
.
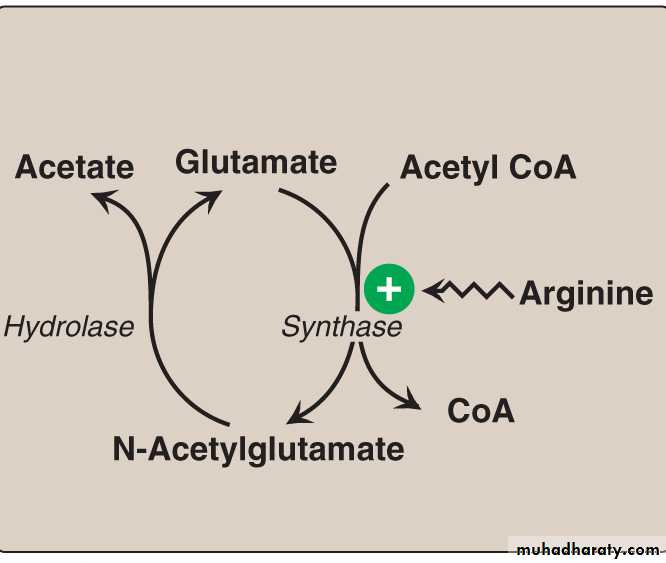
Therefore, the intrahepatic concentration of N-acetylglutamate increases after ingestion of protein rich meal ,which provides both the substrate (glutamate) and the regulator N-acetylglutamate synthesis,this leads to an increase in rate of urea synthesis
• A
• m• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Inborn Error of Metabolism (Inborn Error diseases)
They are genetic disorders in which specific enzymes are affected producing a metabolic block with pathological consequences like convulsion ,loss of appetite ,failure to thrive and vomiting,
S P
S: substrateP: product (NORMAL)
E: Enzyme
• A
• m• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Increase S Decrease P
Block
This block can be responsible for
1 decrease in the product.
2increase or accumulation of substrate S behind the block X or Y.
3increase in the formation of metabolite X,Y
Inborn Error diseases are either
Harmful untreatable (tyrsoinemia)
Harmful treatable (phenylketonuria)
Harmless (alkaptonuria)
E**
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Urea Cycle Disorders
5 enzymatic defects can be expected
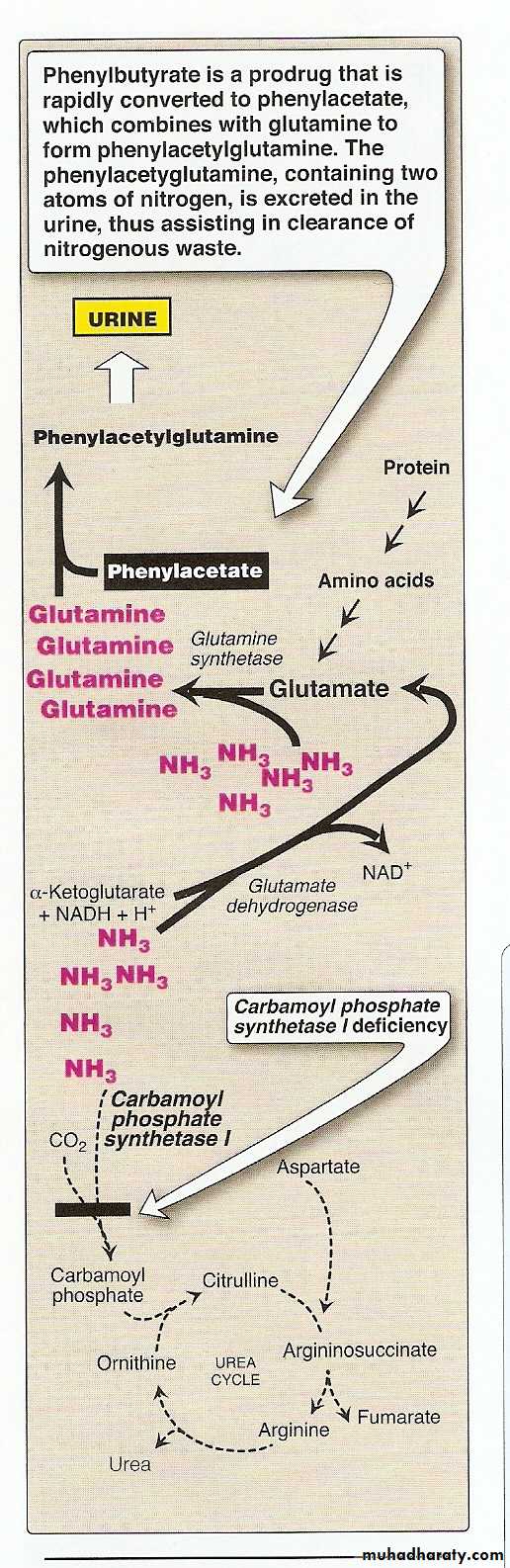
1.Deficiency of carbamyl phosphate synthetase (step 1)
2.Deficiency of ornithine carbamyl transferase(step2)
Both result in ↑in blood ,urinary& hepatic ammonia
( ammonia intoxication)
Symptoms: protein induced vomiting
progressive spasiticity
cerebral atrophy
3. Deficiency of Argininosuccinate synthetase(step 3) Very rare
4.Deficiency in Argininosuccinase enzyme (Step4) ( Most common)
Increase in blood and urinary levels of metabolite immediately preceding the affected step
i.e., ↑ argininosuccinate,citrulline, ornithine
Symptoms: Mental retardation, convulsion.
# Accumulation of argininosuccinic acid in the urine.
#new born baby can not tolerate milk and protein
#Protein loading test is helpful diagnostic test
# Final way of diagnosis is by liver biopsy
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Hyperammonemia
1. Acquired 2. Hereditary
Increase in the level of ammonia in the blood when the ammonia generation exceeds the capacity of urea cycle to convert it to urea.
Normal level of ammonia (5-50)μmol/L, when liver function is impaired level can rise up to( 1000 )μmol/L,consider as medical emergincy due to high toxicity of ammonia specially to the brain.
Ammonia intoxication include tremors,slured speech,vomiting,cerebral odema and blurring of vision.At high concentration can cause coma and death.
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Hyperammonemia
1. Acquired 2. Hereditary
Acquired:
due to acute liver diseases ,viral hepatitis,ischemia,hepatotoxin,cirrhosis of the liver caused by alcoholism.
Biliary obstruction may result in the collateral circulation around the liver, consequently, portal blood is shunted directly into the systemic circulation and dose not have access to the liver,the detoxification of ammonia to urea is impaired or inhibited leading to high level of circulating ammonia in the blood.
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Hyperammonemia
2. Hereditary
Hereditary; Genetic defects of each of five enzymes of the urea cycle can be the cause,ornithine transcarbamoylase deficiency is the most common of these disorders .
Failure to synthesize urea lead to hyper ammonemia during the Ist week following birth.,those who survive end with mental retardation as all other urea cycle disorders.
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Hyperammonemia
2. Hereditary
Treatment includes limiting protein in the diet and administrating compound that bind covalently to amino acid producing nitrogen- containing molecules that are excreted in the urine
Phenylbutyrate given orally converted to phenylacetate.This condenses with glutamine to form phenylacetylglutamine which is excreted in the urine
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
• A
• m• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Clinical importance of Blood urea:
In healthy individual blood urea concentration is 10-40 mg/dl.
High protein intake marginally increase blood urea level however this is well with in normal range .
About 15-30 gram of urea is excreted in urine daily.
Blood urea measurement can be used for the evaluation of renal function.
Elevation of blood urea can be classified into:
1 pre-renal: associated with increase break down of protein observed after major surgery , prolonged fever ,diabetic coma,thyrotoxicosis.
• A
• m
• I
• n
• o
• A
• c
• I
• d
• S
• M
• E
• T
• A
• B
• O
• L
• I
• S
• M
Clinical importance of Blood urea:
2 Renal: in renal disorders acute glomerulonephritis, chronic nephritis, nephrosclerosis polycystic kidney.
3 Post renal: whenever there is an obstruction in the urinary tract , tumor , stones, or prostatic enlargment