Diagnosis and treatment planningin Partially Edentulous Arches


Diagnosis : the determination of the nature of a disease
Treatment plan : the sequence of procedures planned for the treatment of a patient after diagnosisThe ultimate treatment is individualized to address disease management and the coordinated restorative and prosthetic needs that are unique to the patient.
understanding the patient’s desires or chief concerns/complaints regarding his or her condition
ascertaining the patient’s dental needs through a clinical examination,
developing a treatment plan that reflects the best management of desires and needExecuting appropriately sequenced treatment with planned follow-up
Clinical examination
The process of clinical examination involves two stages :
Medical examination
Oral examination
A comprehensive medical history includes :
systemic disorders (Chronic degenerative or dysfunctional diseases)
Medication history
Diet
Habits
Systemic disordes include:
HypertensionDiabetes
Pernicious anemia
Vitamin or nutritional deficiencies
Osteoporosis
Chronic pulmonary disease (i.e.,emphysema and chronic bronchitis)
• Climacteric (i.e., menopausal changes)
• Parkinsonism• Salivary gland disorders
• TM disturbances
• Post radiation therapy
• Bell ’ s palsy
• Lichen planus
• Fungal infections
Oral examination
An oral examination should be accomplished in the following sequence :
visual examination,
pain relief and temporary restorations,radiographs,
evaluation of abutment and periodontium,
vitality tests of individual teeth,
determination of the floor of the mouth position,
Oral prophylaxis and impressions of each arch.
Extra oral examination
This includes : extra oral and intra oral examination.TMJ - tenderness, mouth opening deviation & clicking



Intraoral examination
No of teeth present with their clinical evaluationMalposed teeth
Carious teeth
Existing restoration- sensitivity to percussion
Periodontium
Residual ridges
Saliva
Investing structures
Occlusion and occlusal plane
Oral hygiene index
Pain relief and temporary restorations
to determine the need and management of acute needs and whether a prophylaxis is required to conduct a thorough oral examination.to relieve discomfort arising from tooth defects
the extent of caries and arrest further caries activity
Radiographs
areas of infection and other pathologiesthe presence of root fragments, foreign objects, bone spicules and irregular ridge formations
the presence and extent of caries and the relation of carious lesions to the pulp and periodontal attachment
evaluation of existing restorations : evidence of recurrent caries, marginal leakage, and overhanging gingival margins
the presence of root canal fillings
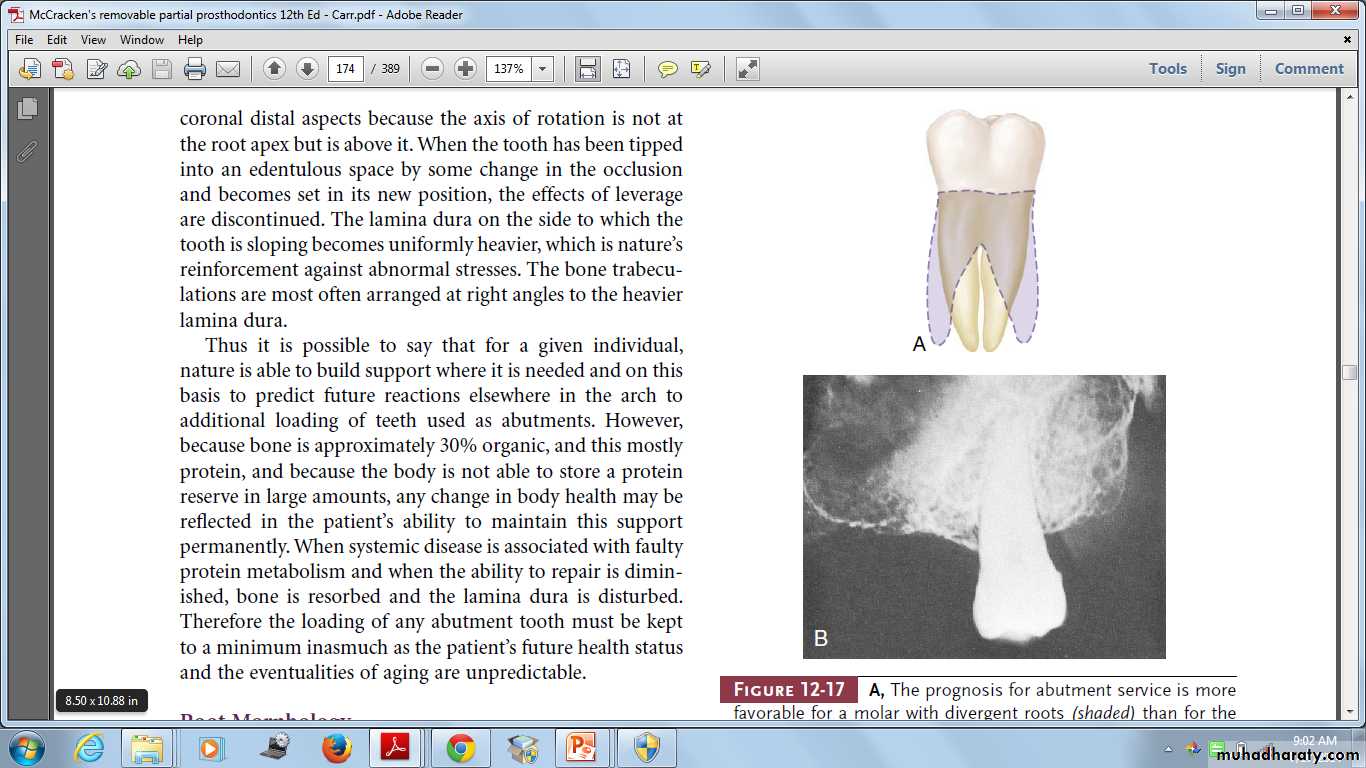
evaluation of periodontal conditions presentto evaluate the alveolar support of abutment teeth, their number, the supporting length and morphology of their roots
the relative amount of alveolar bone loss suffered through pathogenic processes, and the amount of alveolar support remaining
Determination of the floor of the mouth position
To locate inferior borders of lingual mandibular major connectors.Oral prophylaxis & Impression
oral hygiene status before prosthodontic treatment is important.
The impression for the diagnostic cast is usually made with an irreversible hydrocolloid in a stock (perforated or rim lock) impression tray.
Evaluation of abutment
• Anatomic consideration
- Root length, size and form• vitality tests
• caries evaluation
• Periodontal health
• Malpositions
• Analysis of Occlusal Factors
Diagnostic cast
• Supplements oral examination• Permit a topographic survey of the dental arch
• Patient education and motivation
• Custom tray fabrication
• Constant reference
• Patient's record
Surveying of the cast
verification of appropriate mouth modifications for a removable partial denture.
To determine the most desirable path of placement that will eliminate or minimize interference to placement and removal
To locate and measure areas of the teeth that may be used for retention
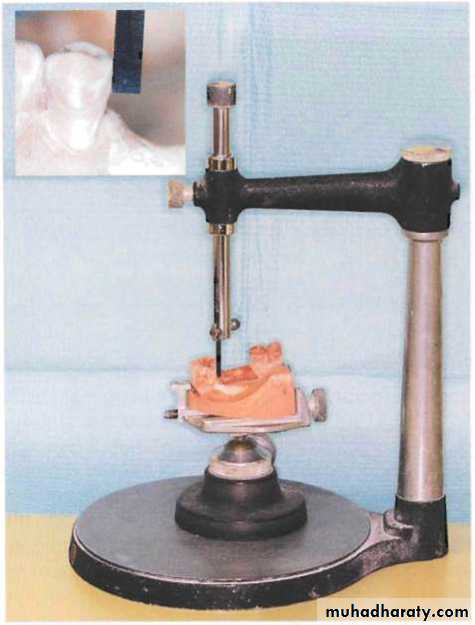
To determine whether tooth and bony areas of interference will need to be eliminated surgically or by selecting a different path of placement
To determine the most suitable path of placement that will permit locating retainers and artificial teeth to the best esthetic advantage.
To permit an accurate charting of the mouth preparation to be made including the preparation of proximal tooth surfaces to provide guiding
Mounting of diagnostic cast
• Occlusal plane & relationships• Abutment tooth contours
• Rest seat areas
• Interarch space
• Residual ridge relation
• Tissue contours
Traumatic Vertical overlap

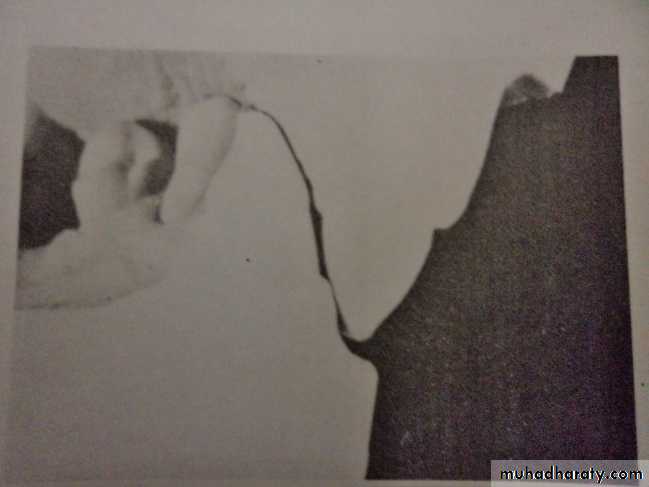
Akerly (1977) has classified traumatic vertical overlap into four basic types:
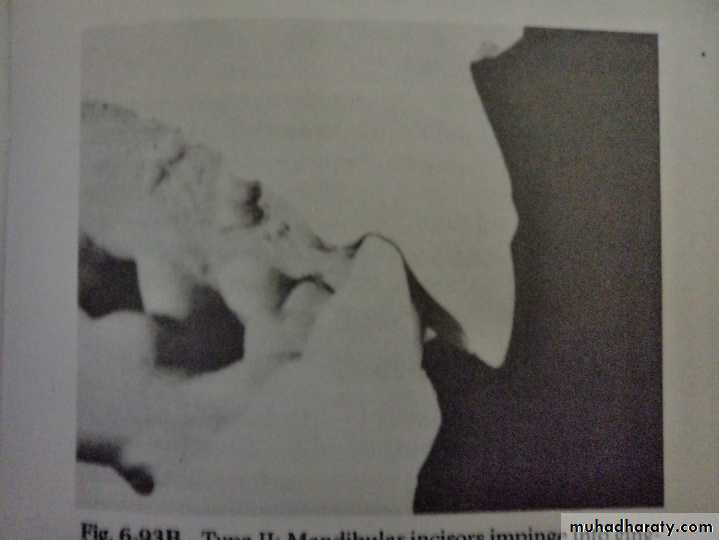
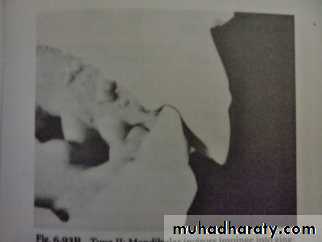
Type 1 – the mandibular incisors extrude and impinge into the palate.Type 2 – the mandibular incisors impinge into the gingival sulci of the maxillary incisors.
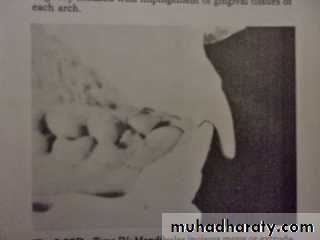
Type 3 – both maxillary and mandibular incisors incline lingually with impingement of the gingival tissues of each arch.
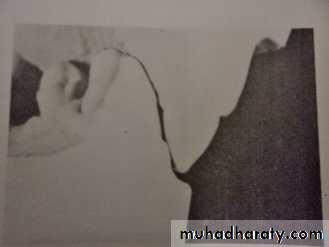
Type 4 - the mandibular incisors move or extrude into the abraded lingual surfaces of the maxillary anterior teeth.

The objectives of any prosthodontic treatment may be stated as follows:
the elimination of diseasethe preservation, restoration, and maintenance of the health of the remaining teeth and oral tissues
the selected replacement of lost teeth; for the purpose of restoration of function
comfort and in esthetically pleasing mannerTreatment planning
Prosthodontic treatment choices
• Implant supported fixed dental prosthesis• Fixed dental prosthesis
• Removable partial denture
• Complete denture
• Combination of the above
• No treatment at all
Indications for removable partial dentures
• Distal extension situations
• After recent extractions
• Long span
• Need for cross-arch stabilization
• Excessive loss of residual bone
• Sound abutment teeth
• Abutment with guarded prognosis
• Economic considerations
1. An RPD can replace lost supporting tissues
in addition to missing teeth. Normalcontour, appearance, and facial support
may be restored with the acrylic resin
denture base material where bone and alveolar
tissue have been lost.
2. An RPD can use soft tissue areas of the
mouth for support in addition to using theteeth, so an RPD may function successfully
when the teeth alone cannot support an
FPD.
3. An RPD may help the patient maintain a
more acceptable level of oral hygiene. Use
of an RPD enables the patient to clean both
the prosthesis and the remaining natural
teeth, since the prosthesis can be removed.
4. An RPD may be designed to splint and stabilize weakened abutment teeth and prevent the loosening, drifting, or extrusion of retained teeth. The cost of cast restorations and the problem of unhygienic soldered splints may sometimes be avoided when an RPD is used.
5. An RPD may be designed to distribute
the forces of mastication on to manysupport areas and to multiple abutment
teeth to prevent overloading only two or
three teeth.
Advantages of an RPD
Shared Decision MakingIt is a communication model
a process where the provider and the patient identify together the best course of care.
it addresses the need to fully inform patients about risks and benefits of care optionsensures that patient values and preferences play a prominent role in the process.
Prosthodontic treatment choices in RPDs
Computer-designed polycarbonate RPD framework.Digital partial design and manufacturing: using 3D printing technology to fabricate RPD frameworks
Valplast RPDs with anterior flexible nylon clasps.
A cast metal framework with metal clasps and flexible nylon polyamide retentive claspsMandibular overlay unilateral distal extension RPD with tooth-colored acrylic resin processed to the metal framework
Mandibular overlay RPD metal framework
Implants and RPDs
Minimize rotation about an axis in a Kennedy Class I or II arch, or any long modification spandirect retainers
restsDevelopment of treatment plan
Phase ICollection and evaluation of data
Pain, infection control
Biopsy
Patient motivation
Phase II
Removal of deep caries
Extirpation of necrotic pulp
Extraction of non-retainable teeth
Periodontal treatment
Interim prosthesis
Occlusal equilibrium
Patient education
Phase III
• Preprosthetic surgical procedures• Definitive endodontic procedures
• Definitive restoration of teeth
• Fixed partial denture construction
• Reinforcement of education and motivation of the patient
• Phase IV
• Construction of removable partial denture• Reinforcement of education and motivation of patient
• Phase V
• Post insertion care• Periodic recall
• Reinforcement of education and motivation of patient.
Importance of a Written Treatment Plan
Plan the amount of time and appointment schedule
Provides information to the patient.
Estimate the professional fees for the treatment.
Coordinate the schedule for dental laboratory procedures
Meet the legal requirements of informed consent
Various Classifications:
Cummer’s system – 1921The Kennedy System – 1923
The Applegate – Kennedy system
Fiset-Applegate-Kennedy classification
Bailyn’s system – 1928
Neurohr’s System – 1939
Mauk’s system – 1941
Godfrey’s system – 1951
Beckett’s system – 1953
Friedman’s system – 1953
Craddock’s system- 1954
Watt’s system - 1958
The Austin Ledge – 1956The Skinner’s system – 1957
Wild’s system
Swenson’s System – 1960
Avant’s System – 1966
Osborne and Lammie’s system
McDermott’s system
American college of prosthodontics system
Costa’s system
Classification for implant dentistry
KENNEDY’S CLASSIFICATION
Proposed by Dr.Edward Kennedy .
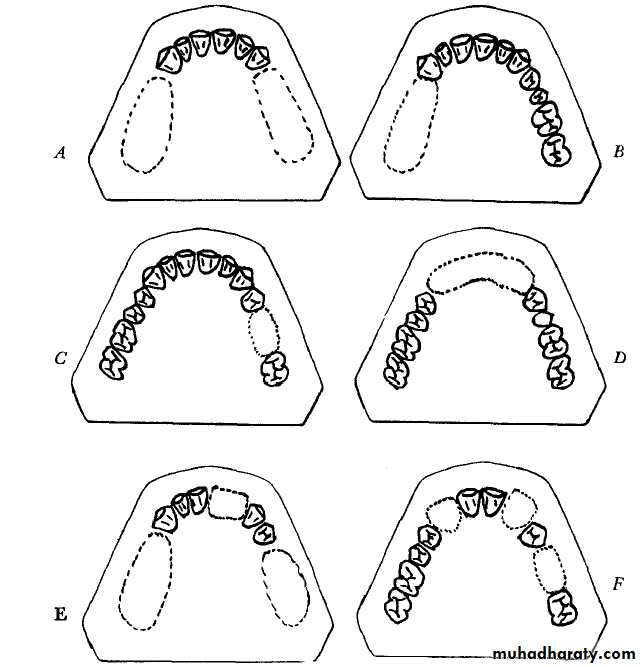
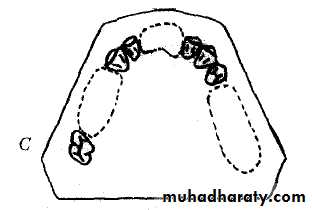
Class-I : Bilateral edentulous area located posterior to the remaining natural teeth.
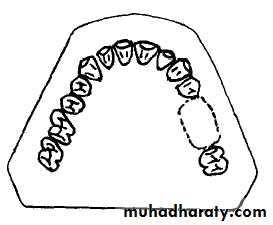
Class II : Unilateral edentulous area located posterior to the remaining natural teeth.
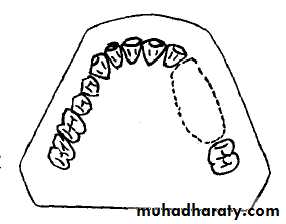
Class III : A unilateral edentulous area with natural teeth both anterior and posterior to it.Class IV : Single but bilateral edentulous area located anterior to the remaining natural teeth.
KENNEDY’S CLASSIFICATION
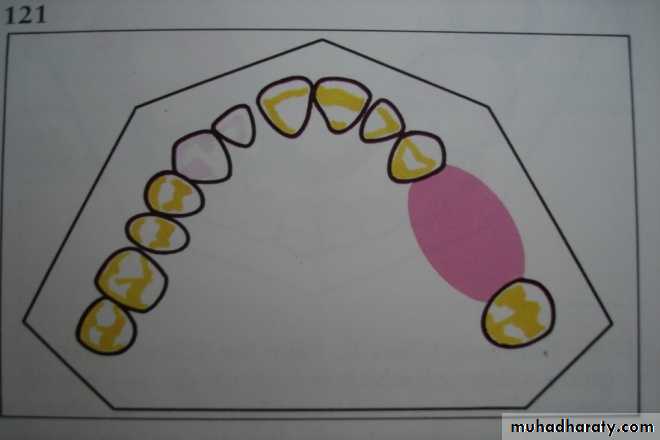
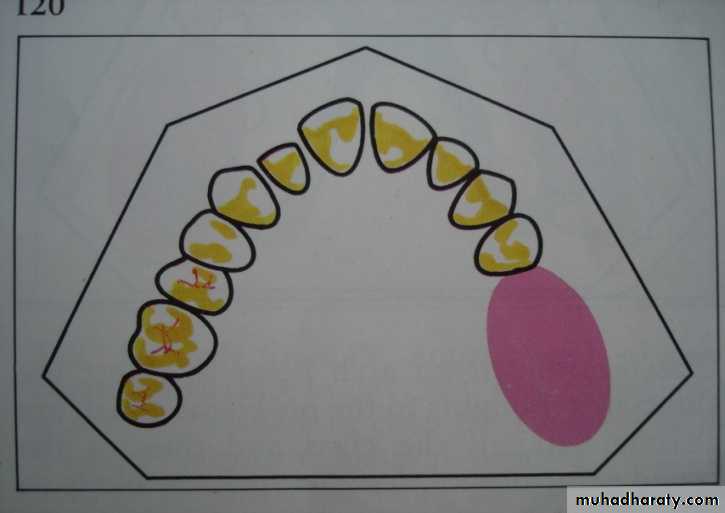
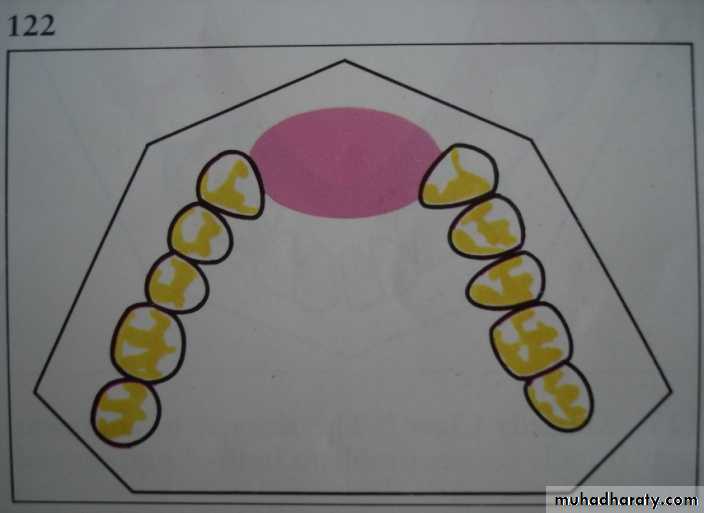
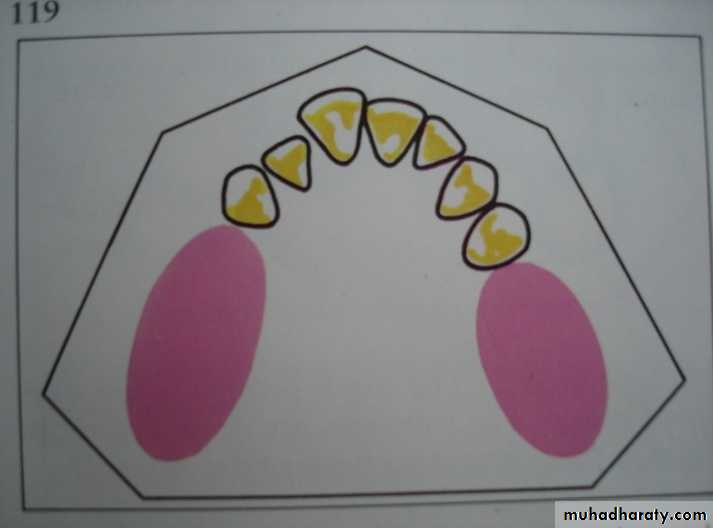
CLASS I
CLASS IICLASS III
CLASS IV
Applegate-Kennedy Classification:
Class V : An edentulous situation in which teeth bound, anterior and posterior but the anterior boundary tooth not suitable for abutment.Class VI: Edentulous situation in which boundary teeth are capable of total support of required prosthesis.
Applegate’s Rules for Applying the Kennedy Classification:
Rule I : Classification should follow rather than precede, any extraction of the teeth that might alter the original classification.Rule II : If 3rd molar is missing, it is not considered in classification.
Rule III : If 3rd molar is present, and is used as abutment, it is considered in classification.Rule IV : If 2nd molar missing, not replaced not considered in classification.
Applegate’s Rules for Applying the Kennedy Classification:
Rule V : The most posterior edentulous area always determine classification.Rule VI : Edentulous area other than those determining the classification are referred to modifications.
Rule VII : Extent of modification is not considered; only the number of additional edentulous areas.
Rule VIII : There is no modification for Class IV.
Thank You