
17/06/2013
1
Medicament used in the treatment
of periodontal disease
Dental plaque
Accumulation of dental plaque induce inflammatory
response in Gingiva that may spread to connective
tissue & bone
So
Plaque control measures include mechanical &
chemical means
plaque control measures aim inhibition of plaque
formation or reducing at regular intervals amount
of plaque to a level at & below which no
inflammatory disease develops
17/06/2013
2
In certain types of diseases like ;
advanced chronic periodontitis,
refractory periodontitis ,
aggressive periodontitis &
periodontitis as manifestation of systemic
diseases
ADJUNCTIVE
chemotherapeutic agents are
necessary
Large no.of microorganism responsible for
initiation & progression of periodontal disease
according to non-specific plaque theory
So
mechanical & chemical plaque controls aim
elimination of entire plaque mass
17/06/2013
3
Non-specific plaque theory
Periodontal disease results from elaboration of noxious
products by entire
plaque
flora
So
when few
plaque
are present, noxious products
neutralized by host defense.
Similarly, large amount of
plaque
produce more noxious
products that overcome host defense
• Support this theory
• control of plaque accumulation
• by mechanical debridment
• & Oral hygiene measures
• induce control of disease in spite of
• the direction toward specific plaque theory
Specific plaque theory
Only certain plaque is pathogenic & its pathogenicity
depends on presence or increase in specific microorganism
So if plaque contains pathogenic
microorganism the periodontal disease will
result & if not no periodontal disease occur
That is why certain patients with plaque &
gingivitis not develop to periodontitis
(contained Gingivitis)
17/06/2013
4
Specific plaque theory
Also patients with periodontitis show
site specificity in pattern of disease as some
sites were disease free while others show
advanced disease in the presence of uniform
host response
Because of increase ability to isolate periodontal
microorganism
(improved sampling of subgingival plaque &
culturing media)
Specific plaque theory
More acceptance of such hypothesis especially
after recognition of A.a. as pathogen in
aggressive periodontitis
Also they have detected
One or few bacteria within plaque mass
constitute the etiological factors
So
antimicrobial drugs should have a potential to
eliminate pathogenic bacteria only
17/06/2013
5
Specific plaque theory
Unfortunately
only few bacteria have been identified as pathogen & satisfy
kochs postulate
among more than 600 species of normal inhabitants of oral
cavity
Good response of some disease
to unique spectrum antimicrobial agent
support such theory
Kochs postulate
Classic criteria by which microorganism can be
judged to be a causative agent in human
infections
Causative agent must ;
1- Be routinely isolated
2- Be grown in pure culture
3- produce similar disease when inoculated into
susceptible laboratory animals
4- Be recovered from lesions in a diseased
animal
Ex; S.mutans in dental caries

17/06/2013
6
In periodontal disease the problems
are ;
1-inability to culture all organisms associated
with disease (as many oral spirochetes)
2-defficulty inherent in defining & culturing sites
of active disease
3-lack of good animal model system for studying
periodontitis
So SIGMUND
criteria;
• Periodontal microorganism must;
1- be associated with disease, increase in no.at disease site
2- be eliminated or decrease in sites with disease
resolution with treatment
3- demonstrate a host response (cellular & humoral)
4- capable of causing disease in experimental animal
models
5- demonstrate virulence factors responsible for enabling
microorganism to
invade, evade & destruct
For instance:
A.a.& porphyromonas gingivalis
17/06/2013
7
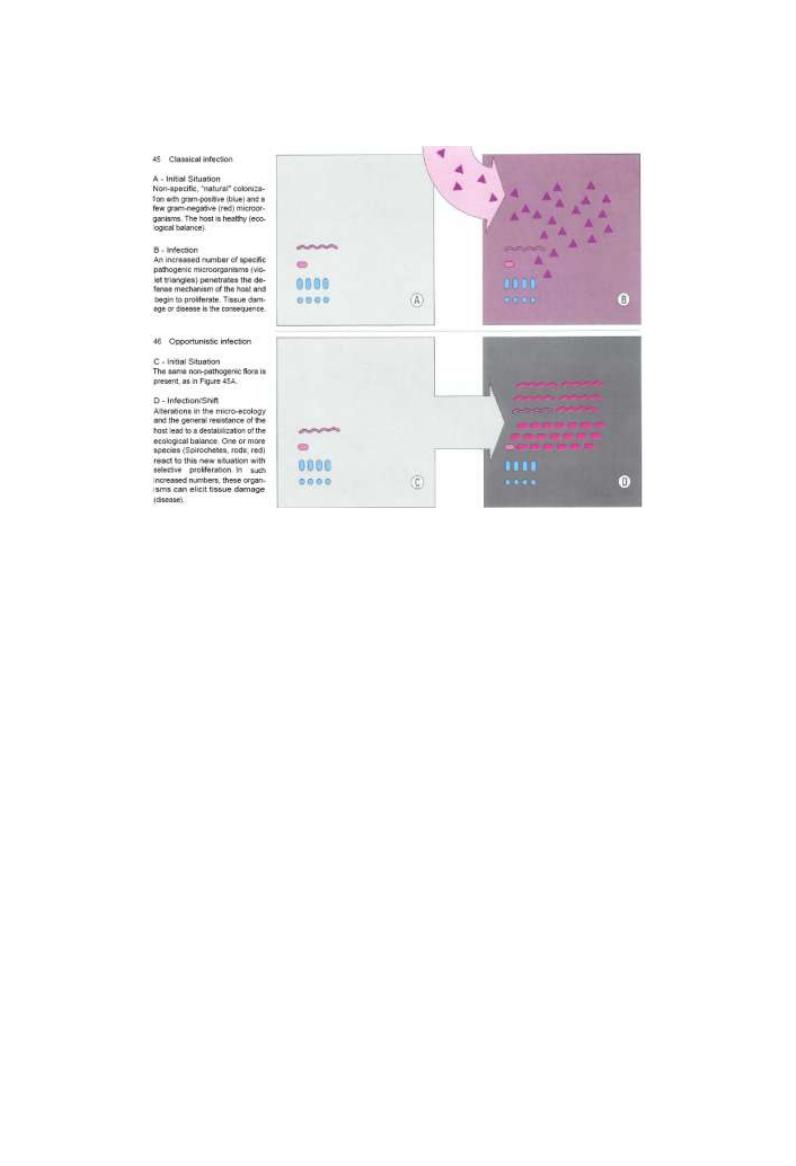
Antibacterial agent not used routinely for
treatment of periodontal diseases ?
Because periodontal disease considers as
an opportunistic infection not classic
infection
Opportunistic infection
develops usually when organism that already
present in the body allow to multiply & proliferate
when alteration in host resistance happen or
presence of favorable environment as;
favorable environment
1-
Q.& Q. alteration of supragingival plaque
2- calcification
3- faulty dentistry
4- hormonal changes with resultant
gingival enlargement
So Antibacterial agents induce limited & transient
suppression of organisms , regrowth of residual
organisms in unchanged environment will occur
So the treatment directs to changing the
environment rather than giving antibiotic
17/06/2013
8
•
Complete elimination by chemical &
mechanical means
or
•
Reduction below certain threshold levels at
which health is maintained
Roll of plaque control measures in prevention of gingivitis & its
conversion to periodontitis
17/06/2013
9
or
• Alteration of microbial composition by introduction of
non-virulent antagonist to subgingival pathogen thereby
replace virulent strain
or
• Prevent adhesion of bacteria to tooth surface through a
change in its chemistry ( interference with pellicle
formation & initial adherence to tooth surface)
Roll of plaque control measures in prevention of gingivitis &
its conversion to periodontitis
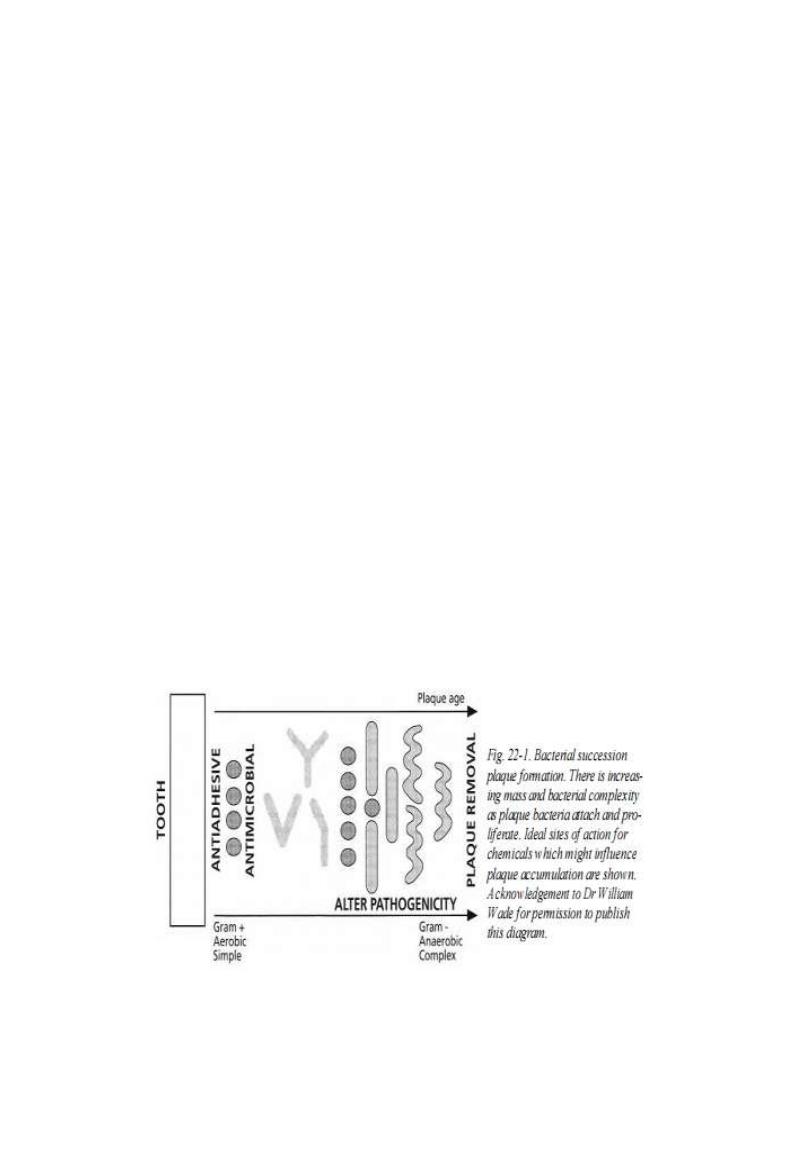
. The action of the chemicals could
fit into four categories:
Antimicrobial
Antiadhesive Antipathogenic.
Plaque removal

17/06/2013
10
At present most antiplaque agents are antimicrobial &
prevent the bacterial proliferation phase of plaque
development
plaque formation could be controlled by antiadhesive or
plaque removal agents but these are not as yet available or
safe for oral use
alteration of bacterial plaque pathogenecity through
chemical agents or bacterial modification would require a
greater understanding of the bacterial etiology of gingivitis
Antibacterial agents
they are grouped according to
substantivity
(contact time that connect a substance & a substrate in a given
medium)
Weak substantivity (1
st
generation ) like ;
certain AB, phenolic compound, oxidizing agent ,fluoride,
plant alkaloids
High substantivity (2
nd
generation ) like chx
17/06/2013
11
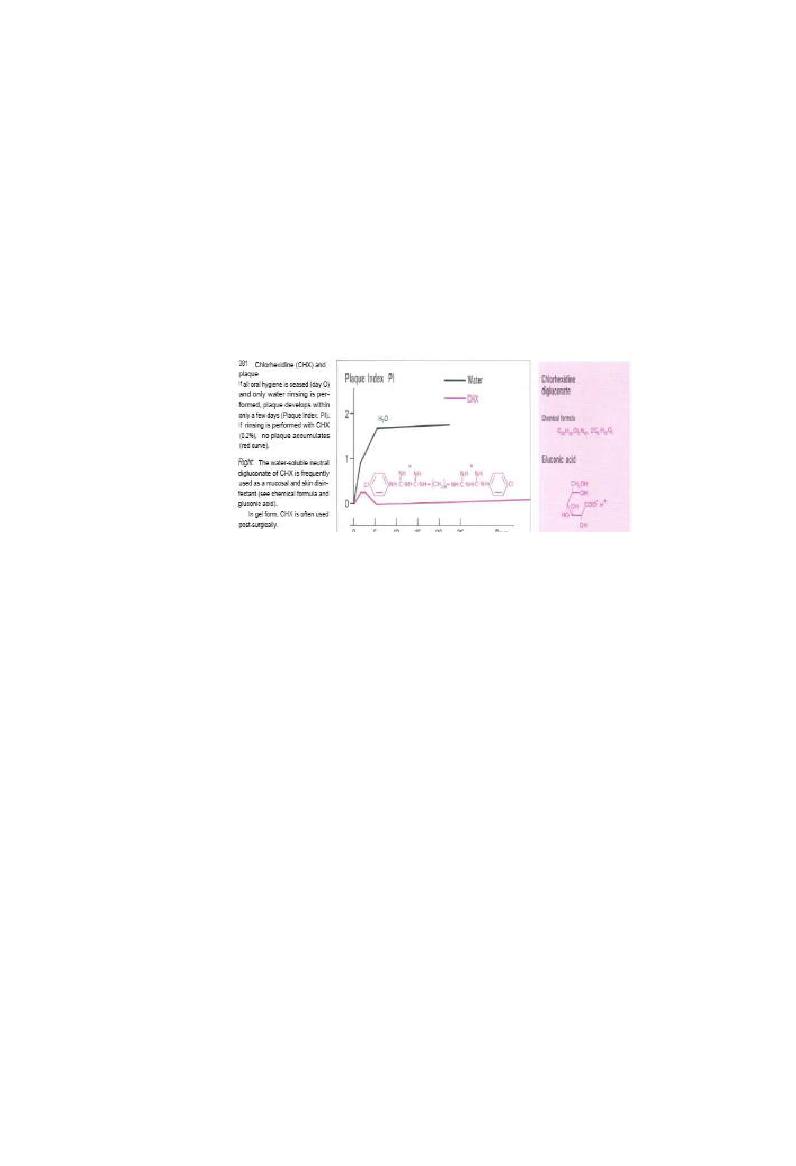
Chlorhexidine digluconate (chx)
Mouthrinsing
with 10ml of 0.2% or 0.12% solution of
chx twice daily produce a plaque reduction of 45-
61% & can safely be used for extended period of
time with no reduction of bacteria sensitivity to chx
Substantivity & mechanism of action
Chx adsorbs to surface of oral tissue including teeth & slowly
released in active form ,about 30% of 10ml will bind &
70% will be spat
Cationic chx molecule bind to anionic component like free
sulfates, carboxyl & phosphate groups of pellicle, thereby
reducing adsorption of protein to tooth required for
formation of plaque
Coating salivary bacteria with chx
molecules also alter mechanism of
adsorption to tooth

17/06/2013
12
Chx molecules bound to salivary
proteins will be released in active
form in 8-12h with low conc.of chx
can still be recovered after 24h
Chx can eliminate already present
plaque
after 6day of its use by
degradation of glycoprotein
Chx has high affinity to cell wall of bacteria
that lead to its death by;
Attack cell wall & change surface structure
that lead to loss of osmotic equilibrium
later on the cytoplasmic membrane is
extruded with vesicle formation &
Cytoplasmic precipitate that
Inhibit repair of cell wall
17/06/2013
13
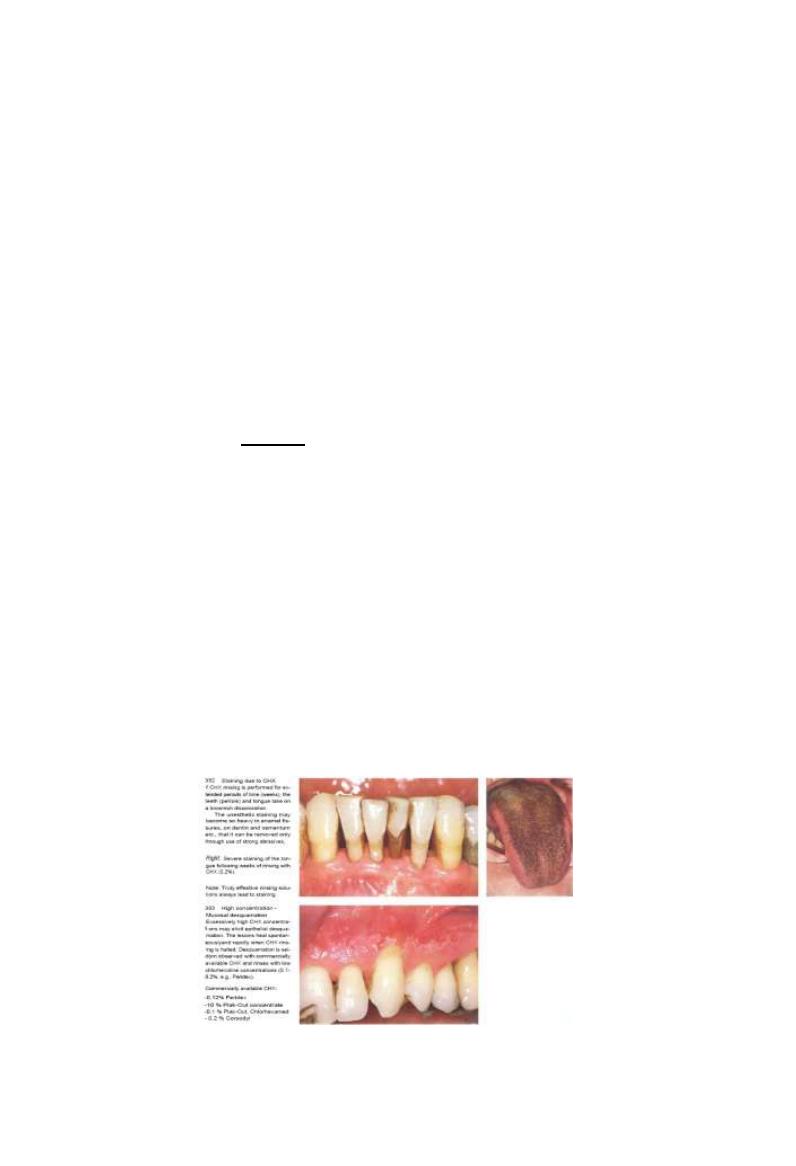
Side effects
1- formation of extrinsic yellow-brown stain (vary from
individual to other & depend on conc.)
2- desquamation & painful mucosal lesions (associated
with high conc.chx)
3- impairment of salty taste perception (transient)
4- ascending parotitis (rare)
5- disturbance of wound healing (associated with high
conc.chx)
6- Enhanced supragingival calculus formation
This effect may be due to the precipitation of salivary
proteins on to the tooth surface , thereby increasing pellicle
thickness and/or precipitation of inorganic salts on to the
pellicle layer
.
Certainly pellicle forming under the influence
of chlorhexidine shows an early and highly
calcified structure

17/06/2013
14
Metabolism & toxicology
Primary route of excresion is through
feaces
Low toxicity as its poorly absorb from GIT
Has not been associated with terratogenic
alteration
{Safe in pregnancy}

17/06/2013
15
Clinical applications
Mouth rinses;
2 daily rinses for 30-45 S. with 10ml of 0.2% chx
& advise subject
no water rinsing, eating or drinking for 1/2h
following rinsing
rinsing should be done 1/2h after brushing ?
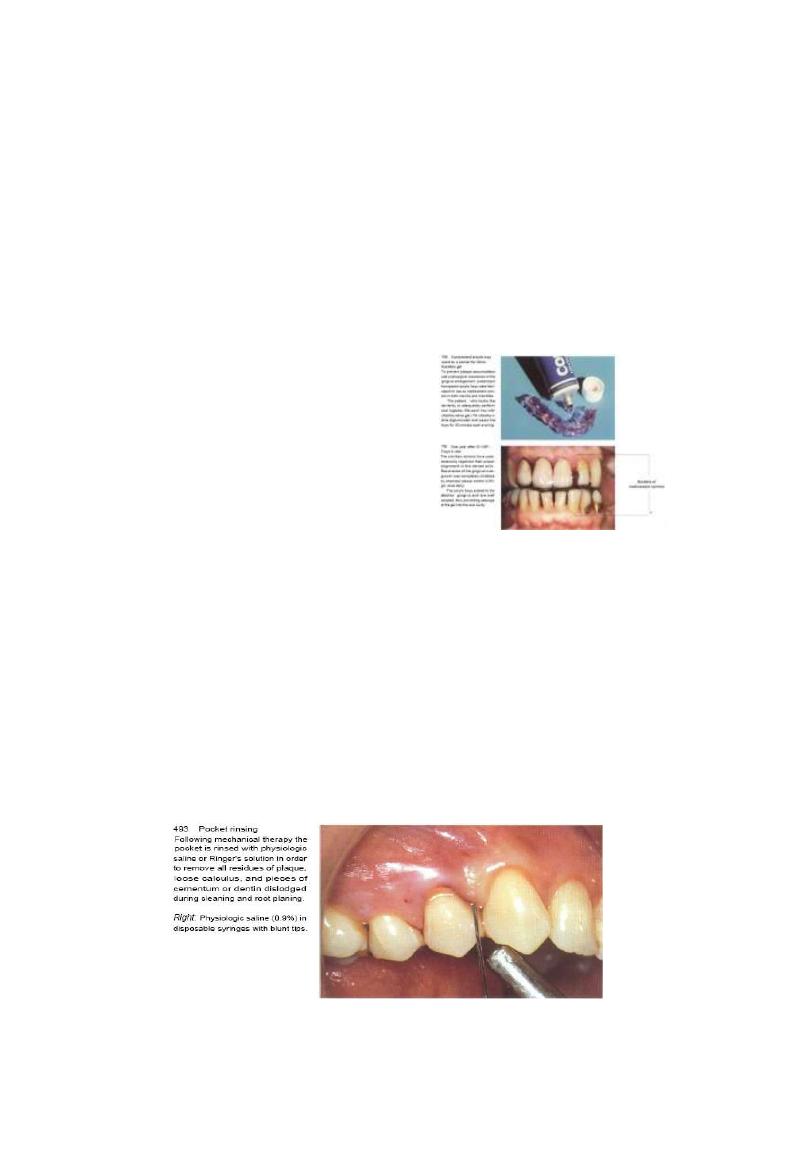
Irrigators
400ml of 0.02% once daily as adjunctive to
mechanical plaque control
17/06/2013
16
Gels 1%
apply for 5min once or twice daily on tray or stint
effective in denture stomatitis & oral candidiasis &
for handicapped
Also once daily for 30min to prevent recurrence of
disease following periodontal treatment in patients
lack dexterity
3 daily application of 1% gel
for several weeks reduce severity
& duration of aphthus ulceration
Professional irrigation
by using syringe with blunt needle to enhance
result obtained with S & RP each recall visit
Its effect is controversy
17/06/2013
17
Chlorhexidine is more effective as a
preventive
rather than a therapeutic agent and
therefore must
be of questionable value as a subgingival
adjunct in
the treatment of periodontitis
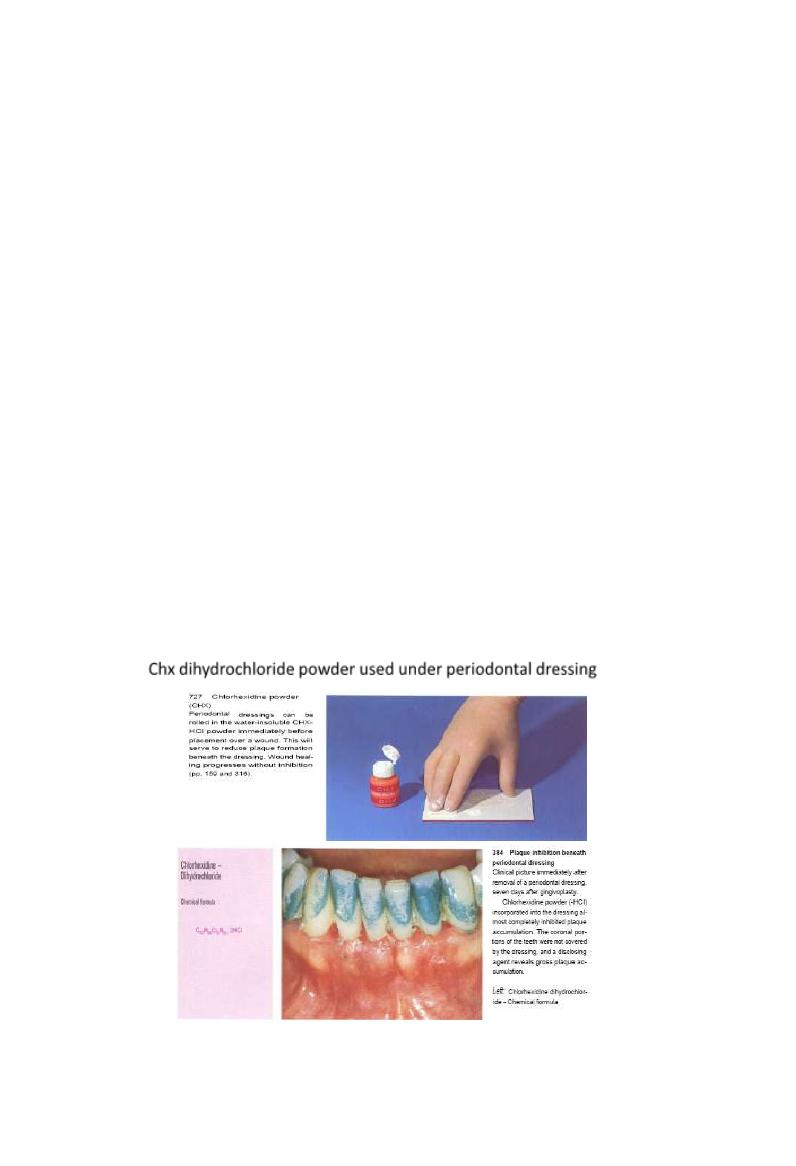
Chx dihydrochloride powder used under periodontal dressing
17/06/2013
18
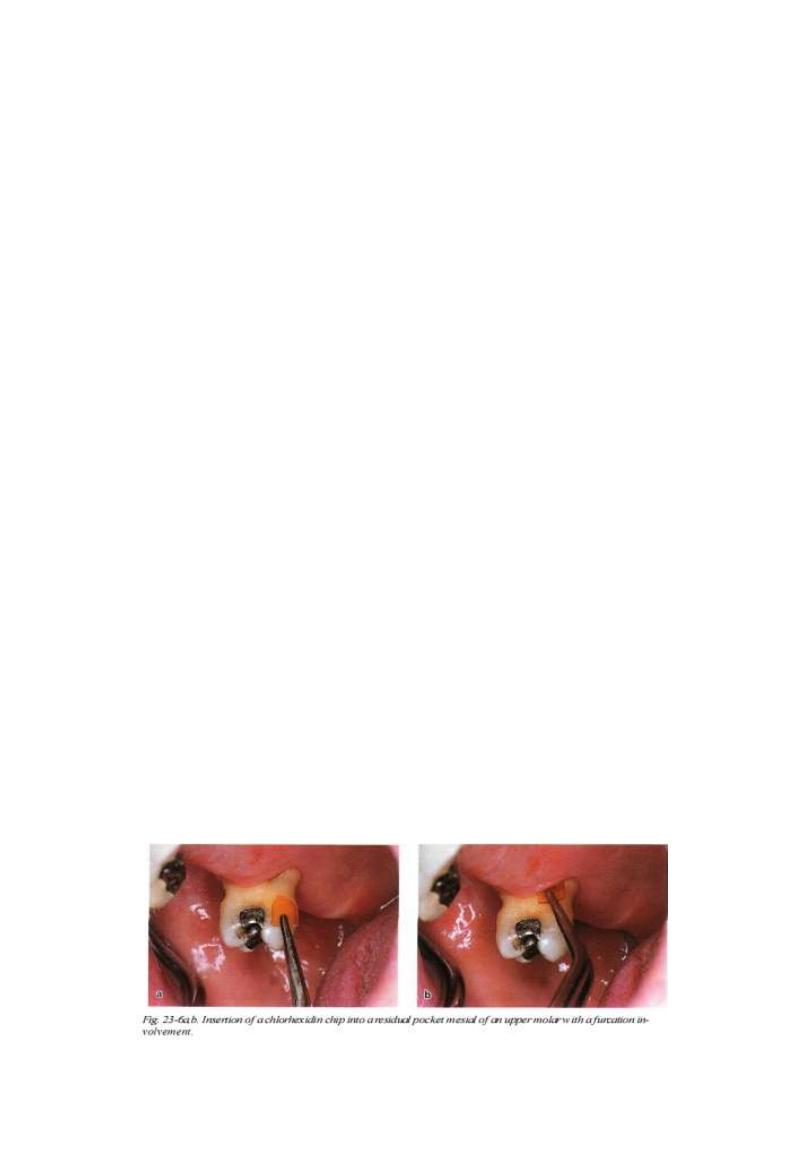
Chlorhexidine gluconate in a gelatin chip
Several attempts have been made to develop local
delivery devices for
the subgingival application of
antiseptic, rather than antibiotic agents.
Acrylic strips and ethyl-cellulose compounds
have been tested for this purpose
PerioChip
a degradable gelatin chip containing 2.5 mg chlorhexidine,
isthe most extensively tested delivery device of this category
Conc.in Gingival fluid greater than 100ng /ml for at least 7d.
Because the chip biodegrades in 7-10 d.,a 2
nd
appointment
for removal is not needed
17/06/2013
19
Other vehicle for delivery include;
1. Toothpaste
2. Spray
3. Chewing gum
4. varnish
Indications
1- jaw #
2- orthodontic therapy
3- handicapped pt.
4- elderly pt.
5- leukemic pt.to Mucositis following
chemotherapy
6- adjunctive treatment following periodontal
surgery (1-4w)
7- to augment plaque control during phase 1 therapy
8- pt.with recurrent problems
9- Mucositis following irradiation
17/06/2013
20
H2P2
Oxidizing agent induce 28% reduction as it consider O2
liberating agent that affect growth of anaerobic bacteria
3-10% solution for topical application used to clean wound &
as a rinsing solution for
Periodontal pocket & initial therapy for NUG
Side effect;
Tissue damage with long term use emphysema if applied
under pressure
hairy tongue
Enzymes
Mucinase
incorporated to dentifrice to inhibit calculus
formation
Urea
induce 30% calculus inhibition
They act to delay plaque mineralization ,keeping
deposits in an amorphous non-hardened state to
aid their removal with tooth brushing & flossing
Fluoride
Low conc.have antimicrobial activity mainly stannous
fluoride than sodium fluoride( bactericidal effect)
17/06/2013
21
Essential oil mouthrinse & phenolic
compound)
Include broad class of chemicals that used as
antiseptic & disinfectants
Thymol is principle antibacterial component of
commercial preparation
Eucalyptol,
menthol,
methyl salicylate,
Triclosan
Essential oil mouthrinse & phenolic
compound)
Listerine retard accumulation of plaque &
severity of gingivitis
Twice daily rinse for 2w induce plaque reduction
range from
19.5-51%
Side effect ; Initial burning sensation & bitter
taste but acclimatization occurs in few days
17/06/2013
22
Quaternary ammonium compounds
Benzylconium chloride and, more particularly
cetylpyridinium chloride are the most studied of this
family of antiseptics. Cetylpyridinium chloride is used
in a wide variety of antiseptic mouthrinse products
usually at a concentration of 0.05%.induce 28%
plaque reduction
Side effect; tooth staining
Herbal extract
Sanguinarine
inhibit bacterial adherance & induce 38% reduction in plaque
formation
Twice daily rinse with 0.03% conc.
Recently its increase the likelihood of oral precancerous
lesions almost ten fold even after cessation of mouthwash
use
Myrtus communis (
(
اس
extract from its leaves has antibacterial activity
due to presence of polyphenol
Qureucus infectori
(
عفص
)
antiplaque activity due to presence of tannic acid

17/06/2013
23
Other antiseptics
A number of antiseptics/antimicrobial agents have been
studied for plaque inhibition. Most have been found to have
little or no effect in vivo; a few have been formulated in
mouthrinse products including
povidone iodine and
hexetidine
Povidone iodine 1%
has a substantivity of only 60 minute lacks appreciable
plaque inhibitory activity or action in acute infections such
as acute ulcerative gingivitis , for which it is recommended.
Povidone iodine is largely without side effects
but as a rinse has potential to affect thyroid function
adversely
Hexetidine 0.1%
saturated pyrimidine, was shown to have limited
plaque inhibitory action and no evidence for anti-
plaque activity when used as an adjunct for oral
hygiene The action of hexetidine against plaque
appears enhanced by zinc salts
side tooth staining and mucosal erosion, although
effects for hexetidine uncommon
Nevertheless, mucosal erosion is markedly
increased in incidence if the concentration is raised
to 0.14%
A mouthrinse product containing 0.1% hexetidine
is available in some European countries