


Congenital disorders of the larynx
LaryngomalaciaSubglottic stenosis
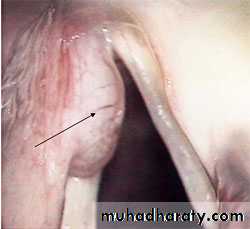
Subglottic hemangioma
Laryngotracheal clefts
Laryngocele
Laryngeal web/ atresia
Vocal cord palsy
Laryngomalacia
The most common typeThe larynx is of an exaggerated infantile type. The epiglottis is long, narrow and folded backwards(omega shaped). The laryngeal inlet is therefore deep and narrow.
Stridor is the main symptom and appears within the first 2 weeks of life, it is intermittent and inspiratory, diminished by rest and sleeping and on lying on prone position, and increase in severity on exertion and crying.
The condition will disappear between the 2nd and 5th years of life. Infrequently it is sever causing feeding difficulties, failure to thrive, apnea and cyanosis.
On examination the laryngeal inlet is deep and narrow and there is collapse of the supraglottic structures on inspiration
Treatment: reassurance is usually all that is necessary. Surgery is rarely needed.
Subglottic stenosis
Defined as a cricoid diameter of less than 3.5 mm in full term infant.
Clinical features: stridor either inspiratory or biphasic which is partially relieved by rest and worsened by exertion but not affected by posture. Feeding difficulty and failure to thrive
Treatment: conservative in mild cases. Tracheostomy in sever cases, growth of the subglottis allow decannulation after some years or laryngotracheal reconstruction to expand the cricoid.
Subglottic hemangioma
Clinically is indistinguishable from subglottic stenosis and the treatment is the same. Laser is particularly effective.Might be associated with external hemangiomas.
Laryngotracheal clefts
Due to incomplete development of the tracheo-esophageal septum.Clinical features: stridor, aspiration and recurrent pneumonia.
Diagnosis: Ba swallow and endoscopic examination
Treatment: clefts at or above the cords treated conservatively. While clefts below the cords cause aspiration and require open surgical repair.
Laryngocele
Originate from the laryngeal ventricleDilated sac filled with air
Either internal or external. Small cyst present as hoarseness or muffled cry. Larger ones cause inspiratory stridor.
Treatment: endoscopy is required to evacuate and uncap the cyst. Treatment may need to be required.
Laryngeal web/atresia
Web formed due to arrest in development or failure of recanalization of the larynx and consists of a fibrous stroma covered by epithelium. The most sever form of laryngeal web is total atresia which is incompatible with life.Clinical features: hoarseness and inspiratory stridor.
Treatment: mild cases treated conservatively while sever cases require tracheostomy and surgical excision.
Vocal cord palsy
Due to birth trauma or idiopathicUnilateral or bilateral.
Clinical features: inspiratory stridor and hoarseness.
Treatment:
Mild cases treated conservatively
Sever cases require tracheostomy and surgical intervention.
Stridor and Stertor
Auditory manifestations of disordered respiratory functionStertor:
Low pitched snoring or snuffly sound caused by obstruction of the airway above the larynx; in the nose, nasopharynx and oropharynx.
Stridor:
Noisy breathing due to obstruction at the level of the larynx, trachea or bronchi.
Both due to turbulence of airflow within a partially obstructed respiratory tract.
While stertor is always inspiratory, stridor could be inspiratory, expiratory or both(biphasic)
Causes of stertor
1- congenital
2- traumatic
3- inflammatory
4- neoplastic
5- allergic rhinitis and nasal polyp
6- hypertrophied tonsils and adenoid
Causes of stridor:
1- congenital2- traumatic
3- foreing body
4- inflammatory
5- neoplastic
6- allergy
7- pressure on the larynx, trachea or bronchi from without.
Management of stertor and stridor
1- Historya- age of onset
b- character
c- onset
d- associated features
e- review of other systems
f- smoking and alcohol dinking
g- pastmedical and surgical history
2- Examination
a- general exam.
b- vital signs
c- nasal exam.
d- exam. Of the oral cavity and oropharynx
e- exam. Of the larynx
f-exam. Of related systems : lungs,heart and CNS.
3- Investigations:
a. Pulmonary functon test and arterial blood gasesb. Laboratory
c. Radiological:
1- plain x-ray
2- CTS and MRI
3- Ba swallow, angiography and thyroid scan
d- endoscopy : panendoscopy
4- Treatment:
a- hospital admissionb- careful follow up
c- conservative measures
d- tracheostomy or endotracheal intubation in sever cases
e- traetment of underlying cause