Pediatrics cardiology
SADIQ M. AL-HAMASHProfessor
M.B.Ch.B.; F.I.C.M.C.S. (Pediatrics); F.I.C.M.S. (Cardiology)
College of medicine
AL-mustansiriyah University12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH1
2015
Contents:
Main MenuClick on the purpil circle opposite each item for selective tour.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
2
CONGENITAL HEART DISEASES (cont.) .. definition
• Congenital heart disease, in a definition “a gross structural abnormality of the heart or intrathoracic great vessels that is actually or potentially of functional significance.”12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
3
Overview (Incidence):
1 percent of babies are born with a CHD (risk increase to 4% for 2nd pregnancy following the birth of a child with CHD & 20% to siblings having CHD).Nine out of every 1,000 babies born in the US are born with a congenital heart abnormality.
One third of these babies require intervention to prevent death in the first year of life.
85 to 90 percent of CHDs have no known causes.
5 to 6 percent are related to chromosome abnormality.
3 to 5 percent are related to single gene defects.
2 percent are related to environmental factors.
Approximately 1.3 million people living in the US today were born with a congenital heart defect, and at least half of these individuals are under age 25.
12/31/2015

Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
4
Etiology:
• Mostly unknown, but appears to result from interaction among many factors, genetic, environmental and maternal diseases, so it is a multifactorial etiology.12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
5
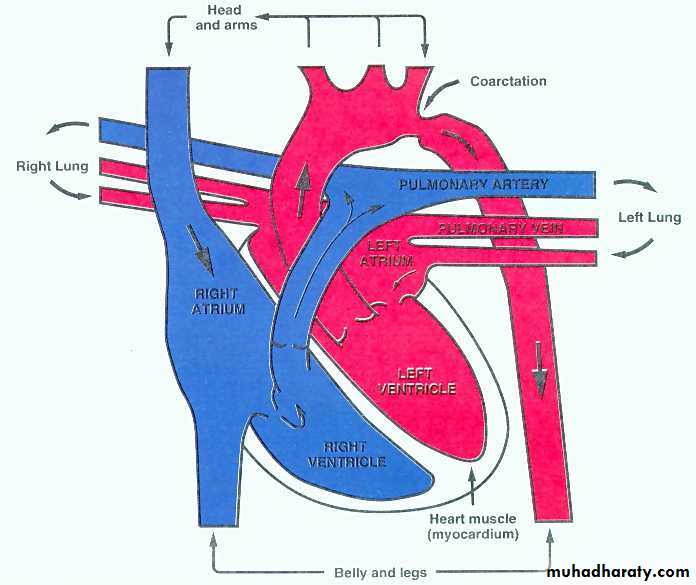
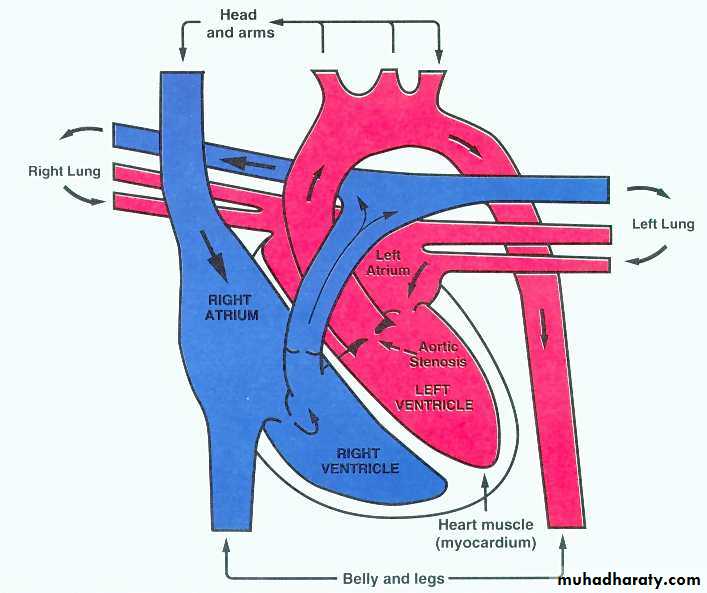
Normal Cardiac Blood Flow
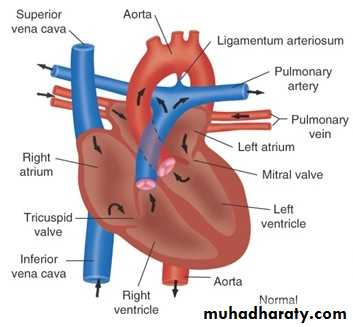
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH6
Classification:
Main Menu12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH7
Classification of congenital heart disease:
• Conditions with ↑ PBF: ( intar- or extracardiac Lt → Rt shunt “without” RV outflow obstruction): best examples VSD, PDA.
• Conditions with ↓ PBF: (shunt “with” RV outflow obstruction): eg. TOF
• Conditions with normal PBF: eg. Coarctation of aorta, Pulmonary stenosis (PS), Aortic stenosis (AS).
PBF: Pulmonary Blood Flow; PDA: patent ductus arteriosus; RV: Right Ventricle; TOF: Tetralogy of Fallot; VSD: Ventricular Septal Defect
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
8
1. Conditions with ↑ PBF:
• Examples:Ventricular septal defect (VSD); Atrial septal defect (ASD); Patent ductus arteriosus (PDA); Total anomolus pulmonary venous drainage (TAPVD); Transposition of great arteries (TGA); Tricuspid atresia without pulmonary stenosis (PS); Single ventricle without PS.
Clinical Features:
• Signs& symptoms of heart failure
• Recurrent chest infections;
• Failure to thrive
Complications:
Pulmonary hypertentin +/- Eisenmenger’s syndrome
Chest X-rays:
• Cardiomegaly
• Plethoric lungs.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
9
1. Conditions with ↑ PBF (cont.):
• Echocardiography :Defining the defect with “no PS”.
• Medical Treatment:
• Antifailure medications.
• Nutritional support
• Treatment of infections
• SBE prophylaxis
• Surgical Treatment:
• Palliative: Pulmonary artery (PA) banding
• Definitive: closure of the defect
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
10
Conditions with ↓ pbf:
EXAMPLES:• Tetralogy of Fallot (TOF)
• Double outlet right ventricle (DORV) with PS
• Single ventricle with PS.
CLINICAL FEATURES:
• Cyanosis
• Hypercyanotic spells (cyanotic spells; Fallot spells; “tet” spells).
Complications:
• Polycythemia
• Cerebrovascular accident (CVA)
• Brain abssess
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
11
Conditions with ↓ pbf (cont.):
• Chest X-rays:• “Small” heart
• Oligemic lung
• Echocardiography :
Different cardiac anomalis “with PS”.
• Medical Treatment:
• Beta-Blockers
• Treatment of complication (eg. Hypercyanotic spells- see later)
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH12
Conditions with ↓ pbf (cont.):
• Surgical Treatment:• Palliative: shunt operation (eg. BT shunt(1), Glenn operation(2))
• Definitive: according to the lesion.
“Modified” Blalock-Taussig (BT) shunt: using prosthetic matrial e.g., Gore-Tex tube between the subclavian artery and the ipsilateral pulmonary artery. The “classic” one connects the subclavian a. directly to the ipsilateral pulmonary artery.
Glenn operation: anastomosis between SVC and distal RPA in end-to-end fashion.
Fontan operaion: complete seperation of of the pulmonary and systemic circuits. The SVC blood is directed to the RPA (Glenn shunt) and right atrial appendage is anastomed to the LPA which direct all IVC blood to LPA. Nowadays various forms of Fontan modifications
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH13
• Conditions with ↓ PBF
• Conditions with ↑ PBF• TOF
• DORV with PS
• Single ventricle with PS
• VSD; ASD;PDA; TAPVD; TGA; Tricuspid atresia without (PS); Single ventricle without PS.
• Examples
• Cyanosis
• Hypercyanotic spells (cyanotic spells Fallot spells; “tet” spells).
• Signs& symptoms of heart failure
• Recurrent chest infections
• Failure to thrive
• Clinical Features
• Polycythemia
• Cerebrovascular accident (CVA)
• Brain abssess
• Pulmonary hypertentin +/- Eisenmenger’s syndrome
• Complications
• “Small” heart
• Oligemic lung
• Cardiomegaly
• Plethoric lungs
• Chest X-rays
• Different cardiac anomalis “with PS”
• Defining the defect with “no PS”
• Echocardiography
• Beta-Blockers
• Treatment of complication (eg. Hypercyanotic spells- see later)
• Antifailure medications
• Nutritional support
• Treatment of infections
• SBE prophylaxis
• Medical Treatment:
• Palliative: shunt operation (eg. BT shunt, Glenn operation)
• Definitive: according to the lesion.
• Palliative: Pulmonary artery (PA) banding
• Definitive: closure of the defect
• Surgical Treatment
IN SUMMARY:
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
14
Few important notes:
“Shunt size”: The extent of extra flow is assessed as the ratio of measured pulmonary blood flow (Qp) to systemic blood flow (Qs).
In the normal case, where no connection exists, the ratio Qp:Qs is 1:1.
Left-to-right shunting results in a Qp:Qs >1, while right-to-left shunting results in a Qp:Qs <1.
For example, a Qp:Qs of 2:1 indicates that the pulmonary blood flow is twice that of systemic blood flow.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
15Pulmonary Hypertension (PH) is defined as an elevation of pulmonary artery pressure (PAP) due to any cause.
• Mean PAP ≥ 25 mm Hg.
• Normal mPAP= 6-10mmHg
12/31/2015
Pediatric Cardiology...Assist. Prof. SADIQ M. AL- HAMASH
16
Pulmonary Hypertension ..definition ..2013
Pulmonary arterial hypertension (PAH) is defined as a specific type of PH caused by pulmonary vascular disease of the precapillary arterioles in the absence of other causes.A revision of the World Health orgnization (WHO) classification, including most of the of PH encountered in children, was proposed at the IO Dana Point meeting in 2008 (Table 67.1)
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH17
Definition of PAH by WHO
2008 Dana Point/ACC Consensus• Required:
• PCWP ≤ 15 mm Hg
• PVR ≥ 3 Wood Units (240 dynes.sec.cm-5)
• PASP > 35 mmHg, PADP > 15 mmHg
• PASP ….pulmonary artery systolic pressure
• PADP……pulmonary artery dystolic pressure• PCWP…. Pulmonary capillary wedge pressure
PVR…….. Pulmonary vascular resistance
Main Menu
SADIQ M. AL-HAMASHProfessor
M.B.Ch.B.; F.I.C.M.C.S. (Pediatrics); F.I.C.M.S. (Cardiology)
VENTRICULAR SEPTAL DEFECT
(VSD)
12/31/2015
Pediatric Cardiology...Assist. Prof. SADIQ M. AL- HAMASH19
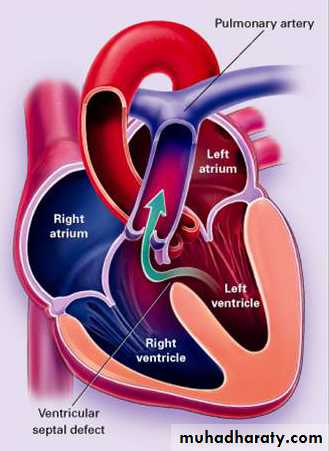
Ventricular Septal Defect
DefinitionIs a congenital opening ( hole or multiple holes) in the interventricular septum which connect both ventricle of the heart.
A VSD may be part of another major cardiovascular
anomaly and may be acquired, and primary VSD may
have minor coexisting morphologic abnormalities
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH20
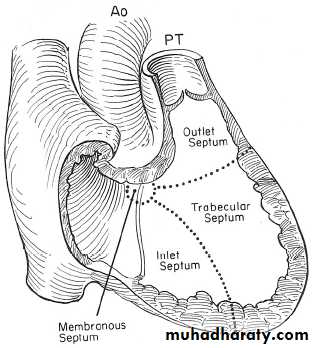
VENTRICULAR SEPTAL DEFECT (cont.)
• The most common CHD• Anatomically: classified into:
• Perimembranous VSD 80%
• Muscular VSD 10%
• Inlet VSD 5%
• Outlet VSD 5%.
• Hemodynamically (functionally)
• classified into:
• Small VSD (small Lt.-Rt. Shunt)
• Moderate VSD
• Large VSD
•
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH21
• Pathophysiologiy:
• The magnitude of the L-R shunt depends on: size of VSD & degree of pulmonary vascular resistance.• In large VSD, there is no resistance to the flow large shunt progressive increase in right ventricular (RV) & pulmonary artery pressure pulmonary vascular resistance which causes Rt.-Lt. (Eisenmenger syndrome) which is irreversible.
• In small VSD, there is high resistance to the flow through the VSD small Lt.-Rt. Shunt pressure is normal in RV and pulmonary artery (PA).
VENTRICULAR SEPTAL DEFECT (cont.)
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
22
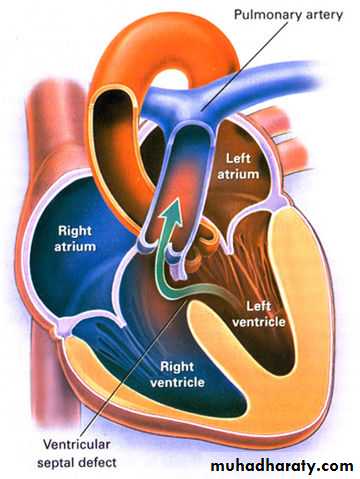
Hemodynamics of VSD
VSD shuntPulmonary plethora
PA congestive
RV
RA
SVC, IVC
Increased volume of blood in pulmonay circulation
LA enlargement
LV enlargement
Aorta ejects less blood
Systemic circulation insufficiency
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH23
VENTRICULAR SEPTAL DEFECT (cont.)
• Clinical features:
• Small VSD: asymptomatic.
• O/E: loud harsh, grade 4-6 pansystolic murmur at the lower left sternal border.
• Large VSD: heart failure (between the age of 2-8 weeks); the patient will show tachypnoea, dyspnoea, recurrent pulmonary infections, feeding difficulty, poor growth and excessive sweating.
• O/E: the murmur is soft with loud P2.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
24
VENTRICULAR SEPTAL DEFECT (cont.)
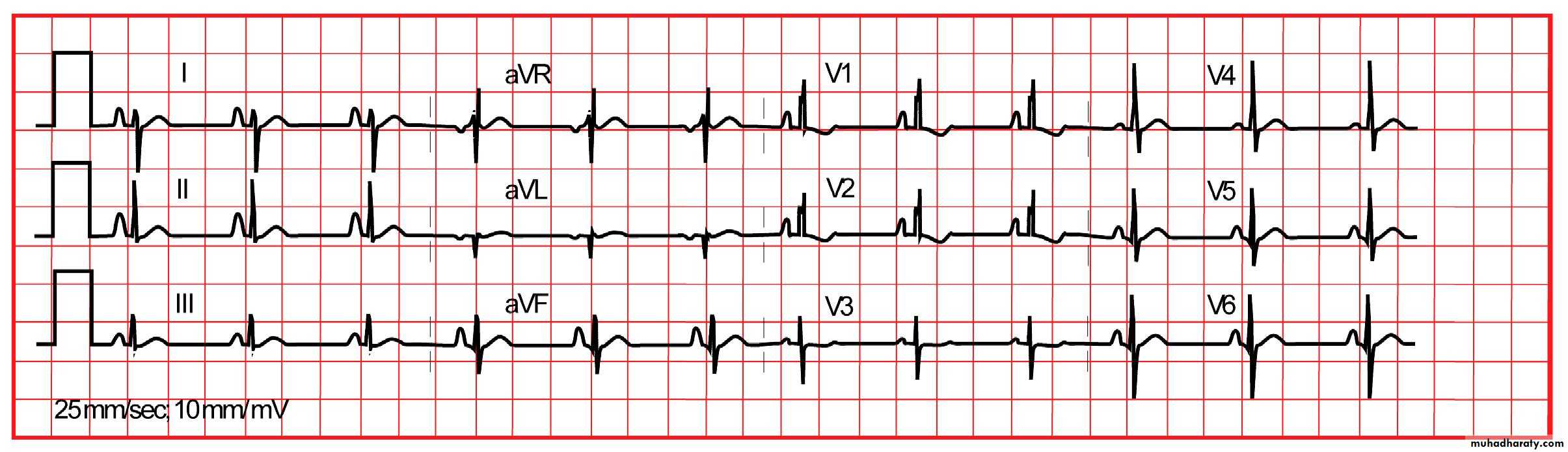
• Diagnosis:• ECG:
• small VSD normal ECG
• large VSD biventricular hypertrophy
•
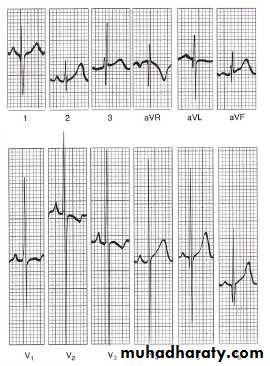
ECG with biventricular hypertrophy in large VSD.
12/31/2015Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
25
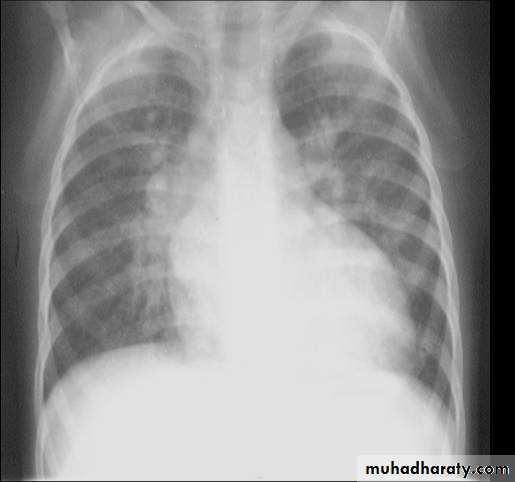
VENTRICULAR SEPTAL DEFECT (cont.)
• X-ray findings• small VSD normal
• large VSD cardiomegaly, dilated pulmonary vessels (plethoric lung)
1. LV and RV enlargement with Left ventricular type
2. Pulmonary vasculature is increased.
3. Prominent PA segment
4. Normal or smaller aorta
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH26
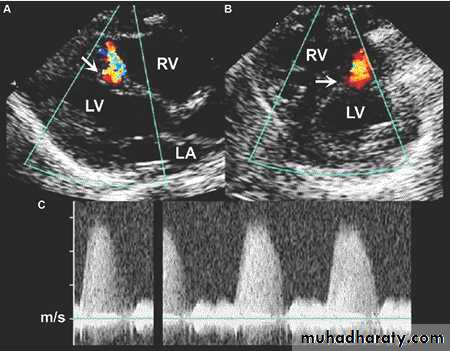
VENTRICULAR SEPTAL DEFECT (cont.)
• Echo:• two-dimensional & Doppler echo must be done in all patients to determine the following:
Size
Anatomical location
Size & direction of intercardiac shunt
The degree of pulmonary hypertension
Presence e of associated lesion (as TOF)
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
27
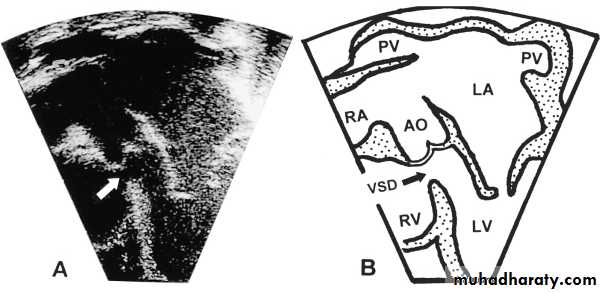
PLAX & PSAX views of echo showing muscular VSD
A5C view echo showing membranous VSDVENTRICULAR SEPTAL DEFECT (cont.)
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
28
VSD …Echo
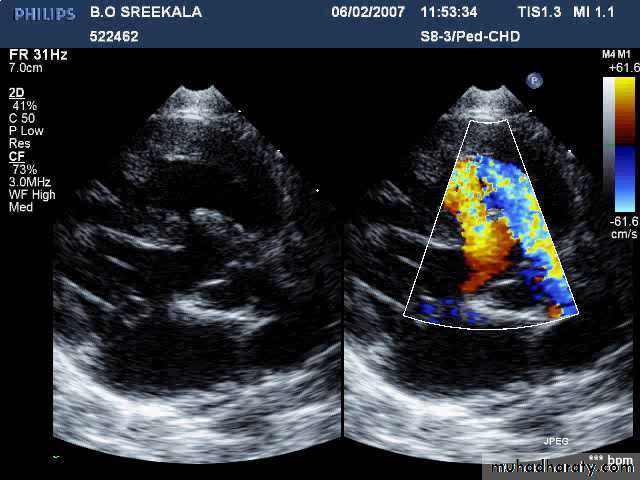
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH29
VENTRICULAR SEPTAL DEFECT (cont.)
• Catheterization & angiography:• A small number of patients with VSD requires cath.
• Benefits:
• Clear anatomical picture of the location and no. of VSD in patients when surgery is required.
• Estimation of magnitude of the shunt & pulmonary vascular resistance.
• Closing some muscular VSDs.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
30
VENTRICULAR SEPTAL DEFECT (cont.)
• Natural history:
• Small VSD: 50% close spontaneously (the majority during the 1st 2 years of life); the other will remain asymptomatic.
• Large VSD: Without surgical repair, most patients will develop pulmonary hypertension and some reach to Eisenmenger syndrome (10%). And some patients develop Bacterial endocarditis .
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH31
VENTRICULAR SEPTAL DEFECT (cont.)
• Management:• Small VSD: The patient needs no treatment apart from follow-up & SBE prophylaxis.
• Large VSD: we have medical, surgical and catheterization options.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
32
• Medical:
• Treatment of heart failure.
• Treatment of infection, especially respiratory.
• SBE prophylaxis.
• Nutritional support.
VENTRICULAR SEPTAL DEFECT (cont.)
12/31/2015Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
33
• Surgical:
• Either pulmonary artery banding or total surgical repair.• Indications:
• Failure of medical treatment of heart failure.
• Repeated pulmonary infections.
• Failure to thrive and growth failure.
• Any degree of pulmonary hypertension (after 2 years of age).
• “Catheterization based treatment:”
• Most muscular VSD and some membranous VSD can be closed by devices placed during cardiac catheterization.
VENTRICULAR SEPTAL DEFECT (cont.)
12/31/2015

Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
34Interventional Options
Percutaneous Device ClosureMuscular VSDs can typically be closed percutaneously
Class IIb recommendation in Guidelines (i.e. surgery still preferred)
No FDA approved devices for perimembranous VSDs, although there are specific devices for this purpose
Concern re proximity of defect to AV node and high risk of complete AV block requiring pacemaker

12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH35
Main Menu
SADIQ M. AL-HAMASH
ProfessorM.B.Ch.B.; F.I.C.M.C.S. (Pediatrics); F.I.C.M.S. (Cardiology)
ATRIAL SEPTAL DEFECT (ASD)
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH36
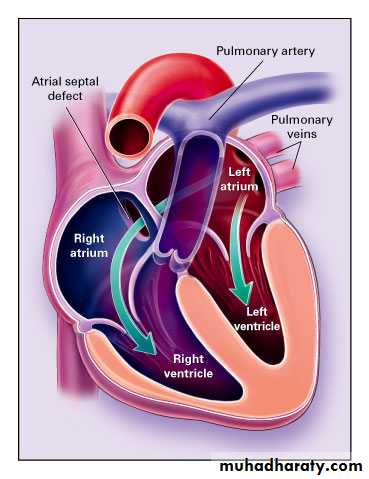
ATRIAL SEPTAL DEFECT (CONT.):
•
• An opening in the inter-atrial septum other than patent foramen ovale;
• Account for 10% of all congenital anomalies• Most common congenital defect to present in adulthood
• more common in females; F:M ratio is 3:1.
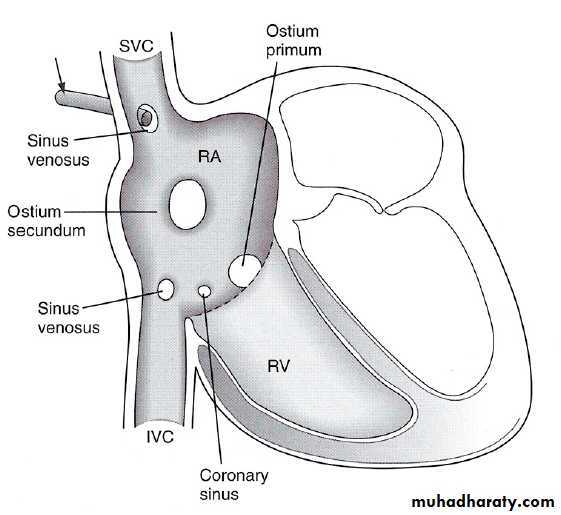
• It has 3 types:
• Secondum ASD (in the middle) 80%
• Primum ASD (in lower part) 10%
• Sinus venosus (in the upper part) 10%.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
37ATRIAL SEPTAL DEFECT (CONT.):
• Hemodynamic effect:• There will be chronic Lt. Rt. Shunt which causes volume overload on the Rt. sided cardiac structures & result in their dilatation & increase of pulmonary blood flow.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
38
ATRIAL SEPTAL DEFECT (CONT.):
• C/F (mostly secondum type):• Most of them are asymptomatic.
• Normal growth
• Dx
• accidentally: fixed splitting of 2nd heart sound, soft ejection systolic murmur at the 2nd left intercostal space, no thrill & parasternal heave.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
39
ATRIAL SEPTAL DEFECT (CONT.):
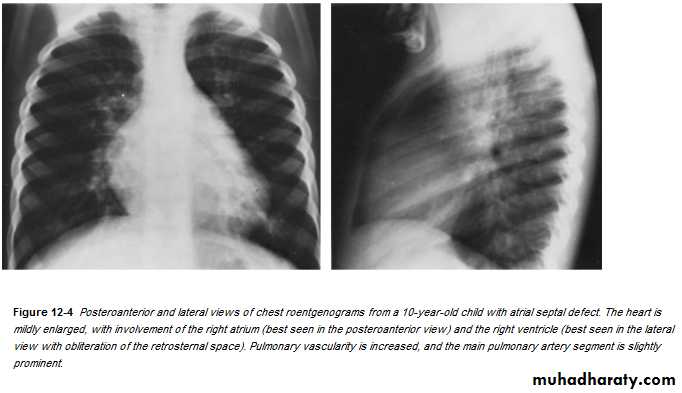
• Dx:• CXR:
• 1. Cardiomegaly of RV configuration. 2. Round apex peak.
• 3. Increase pulmonary marking
•
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH40
Associated findings:
ECG abnormalities:Peaked P-wave (RA enlargement)
Prolonged PR interval
Right axis deviation RAD (+100°)
Incomplete RBBB
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH41
ATRIAL SEPTAL DEFECT (CONT.):
• Echo:• Trans-thoracic & trans-esophageal echocardiography is essential for Dx.
12/31/2015
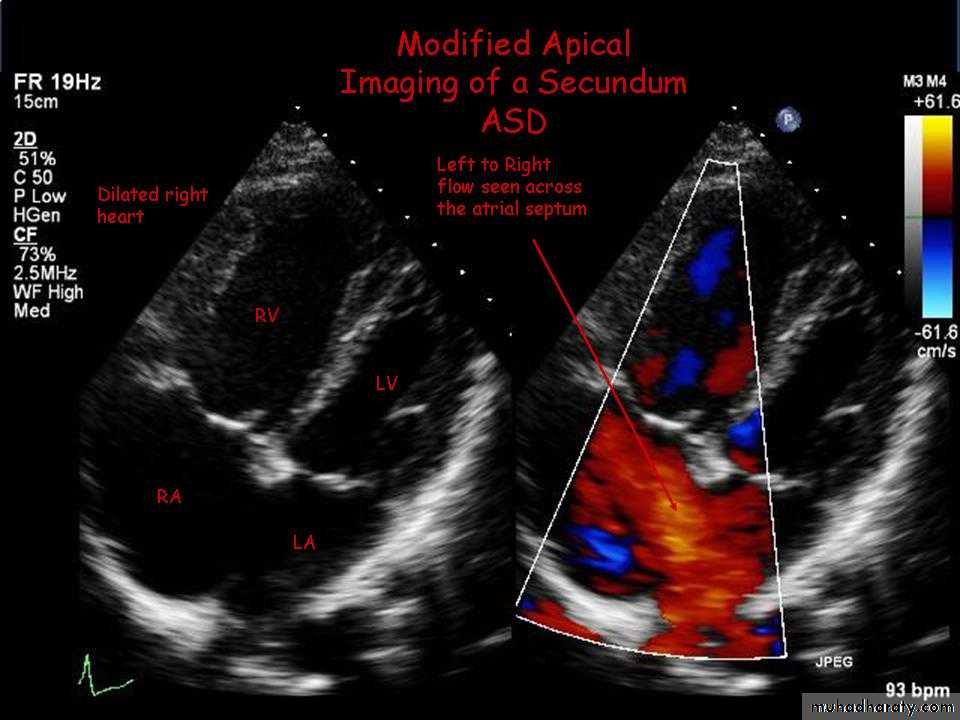
Large Secundum ASD
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH42
ATRIAL SEPTAL DEFECT (CONT.):
• Cardiac Catheterization:• Not essential for Dx, indicated in:
• Therapeutic aim.
• Exclude associated cardiac anomaly as patent anomalies.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
43
ATRIAL SEPTAL DEFECT (CONT.):
• Natural history:
• ASD is a benign lesion.
• Rarely causes heart failure or pulmonary hypertension in the 1st decade of life.
• Rarely complicated by infective endocarditis.
• Rarely closed spontaneously after infancy.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
44
ATRIAL SEPTAL DEFECT (CONT.):
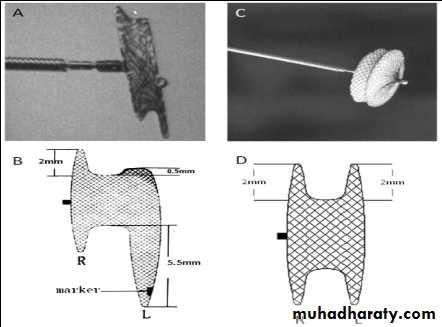
• Treatment:• Closure of ASD in asymptomatic patients is done at 4-5 years, either by occluder, which if failed by surgical repair.
•
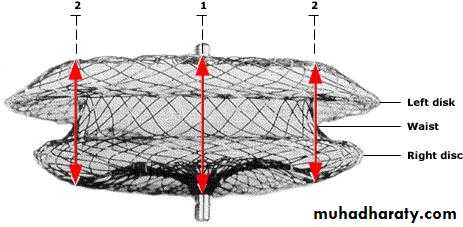
In the lateral view the Amplatzer septal occluder has
a waist between the left and right atrial discs;the left atrial disc is slightly larger than the right one.
Broken lines and red arrows indicate measurement sites.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
45
ATRIOVANTRICULAR SEPTAL DEFECT
It is a group of anomalies sharing a defect at the site of atrioventricular septum and abnormality in the atrioventricular valve.
Common in Down's syndrome, so all patients with Down's syndrome (children) should have cardiac evaluation if symptomatic or before 6 months of age.
Equal no. of males and females are affected.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
46
ATRIOVANTRICULAR SEPTAL DEFECT (cont.):
Classification:12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
47
ATRIOVANTRICULAR SEPTAL DEFECT (cont.):
• Clinical features:• Partial: either asymptomatic (mainly) or mild symptoms.
• O/E: ASD & murmur of mitral regurgitation.
• Complete: as the above with heart failure and/or pulmonary vascular disease.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
48
ATRIOVANTRICULAR SEPTAL DEFECT (cont.):
• CXR:
• Cardiomegaly is always present and involves all four cardiac chambers. Pulmonary vascular markings are increased, and the main PA segment is prominent.
• ECG:
• “Superior” QRS axis with the QRS axis between -40 and -150 degrees is characteristic of the defect.
• Most of the patients have a prolonged PR interval (first-degree AV block).
• RVH or RBBB is present in all cases, and many patients have LVH, too.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
49
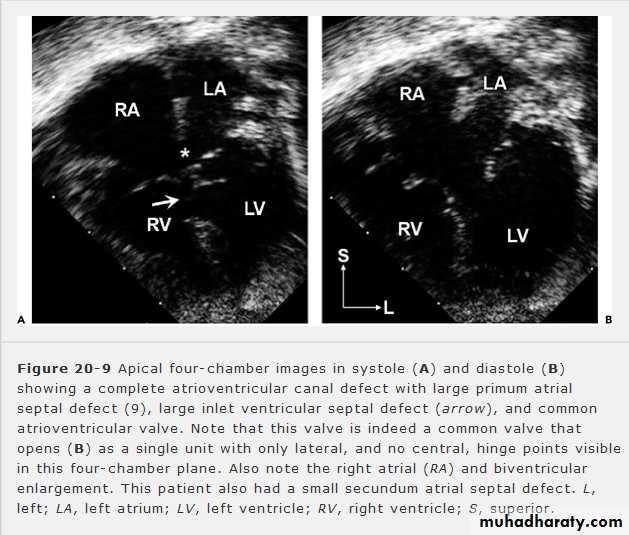
ATRIOVANTRICULAR SEPTAL DEFECT (cont.):
• Echo: is diagnostic.A4C view in systole(A) & diastole (B) showing complete AV septal defect.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
50
ATRIOVANTRICULAR SEPTAL DEFECT (cont.):
• Natural history:
It depends on the size of various atrial and ventricular defects and the amount of mitral regurgitation.
The ostium primum ASD with no mitral regurgitation has the same benign natural history of simple secondum ASD, but with complete AV-canal defect, heart failure and/or pulmonary vascular disease may occur.
• Rx:
• Repair the septal effect (patching), it will cause complete repair.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
51Main Menu
SADIQ M. AL-HAMASHProfessor
M.B.Ch.B.; F.I.C.M.C.S. (Pediatrics); F.I.C.M.S. (Cardiology)
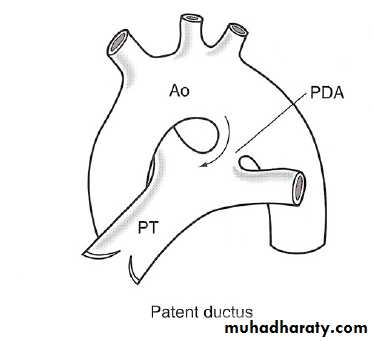
PATENT DUCTUS ARTERIOSUS
(PDA)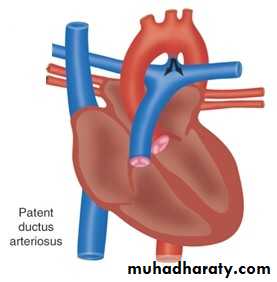
12/31/2015
Pediatric Cardiology...Assist. Prof. SADIQ M. AL- HAMASH52
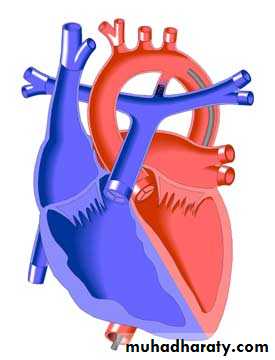
PATENT DUCTUS AaRTERIOSUS (cont.)
It represent persistent patency of the vessel that normally connect the pulmonary artery and the aorta in fetus.It is the most common lesion in infant of mothers with congenital rubella,
PDA more common in females.
•
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
53PATENT DUCTUS ARTERIOSUS (cont.)
• Clinical features:• Patients with small PDA usually are “asymptomatic” but large PDA will result in heart failure & pulmonary hypertension along with growth failure.
• O/E:
• Collapsing pulse with side pulse pressure; on auscultation classical continuous machinery murmur (systolic & diastolic) at the pulmonary area with a thrill when there is severe pulmonary hypertension, only systolic murmur can be heard with loud S2.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
54
PATENT DUCTUS ARTERIOSUS (cont.)
• ECG:
• In small PDA, it is normal, but large PDA, there is normal axis deviation, left ventricular hypertrophy (LVH) or biventricular hypertrophy.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
55
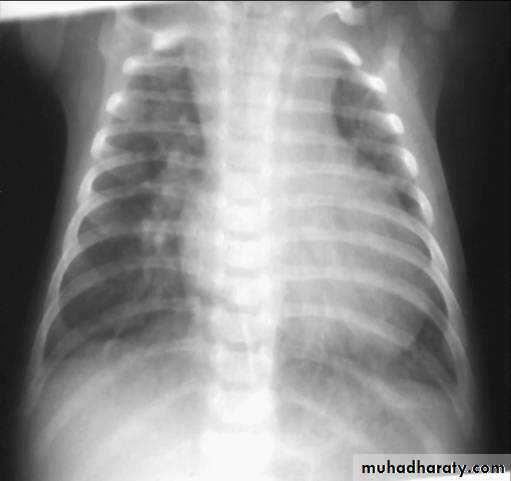
X-ray finding in PDA
Cardiac enlargement with a LV silhouetteMay be LA enlargement
Porminent ascending aorta and aorta knuckle
Plethoric lung field
Prominent PA segment

12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH56
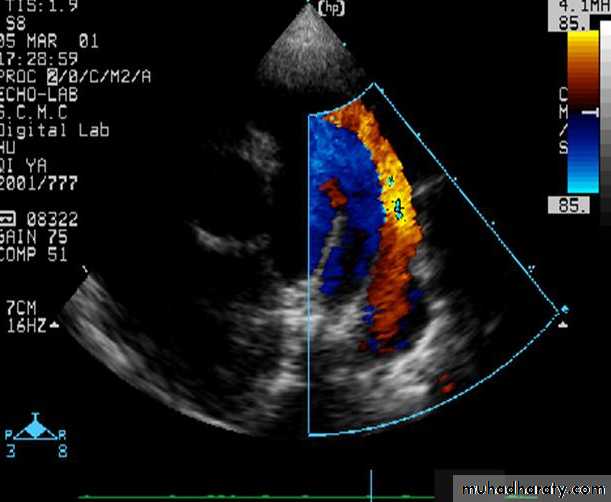
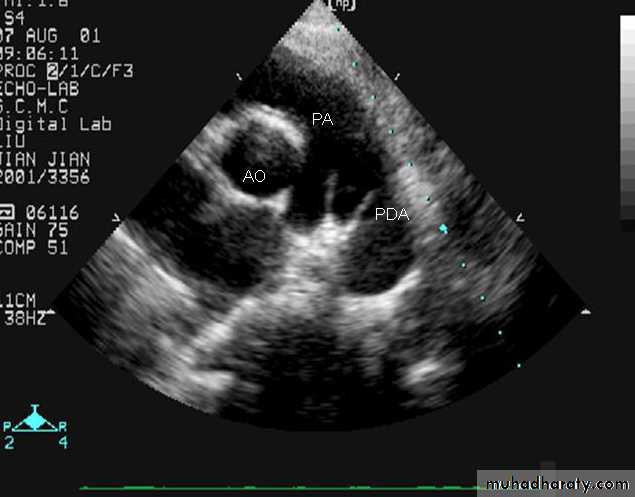
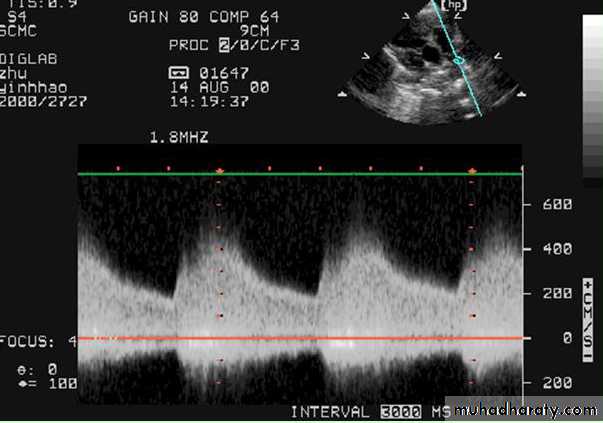
PATENT DUCTUS ARTERIOSUS (cont.)
Echo: is diagnostic2D echocardiogram can idendtify the PDA which can be confirmed by Doppler.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
57
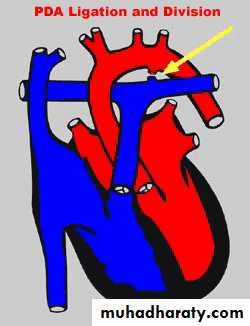
Treatment of PDA…
Medical interventionIn first two weeks, Indomethacin, a prostaglandin synthetase inhibitor, can be given orally to close the ductus. It is effective for 90% preterm PDA cases.
Surgical intervention
Patients can be sent up for operation when there is surgical indications.
Cardiac catheterization
Most PDA closures can be done by transcatheter device usually done by occluder (safe and effective) and some need transthoracic surgery, .
12/31/2015
5812/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
59
Main Menu
SADIQ M. AL-HAMASHProfessor
M.B.Ch.B.; F.I.C.M.C.S. (Pediatrics); F.I.C.M.S. (Cardiology)
COARCTATION OF THE AORTA
12/31/2015
Pediatric Cardiology...Assist. Prof. SADIQ M. AL- HAMASH60
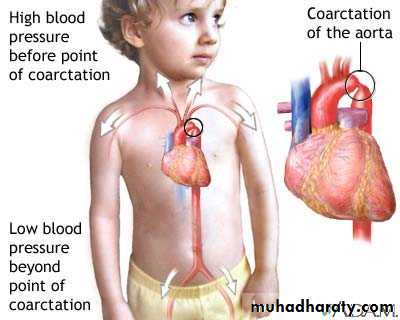
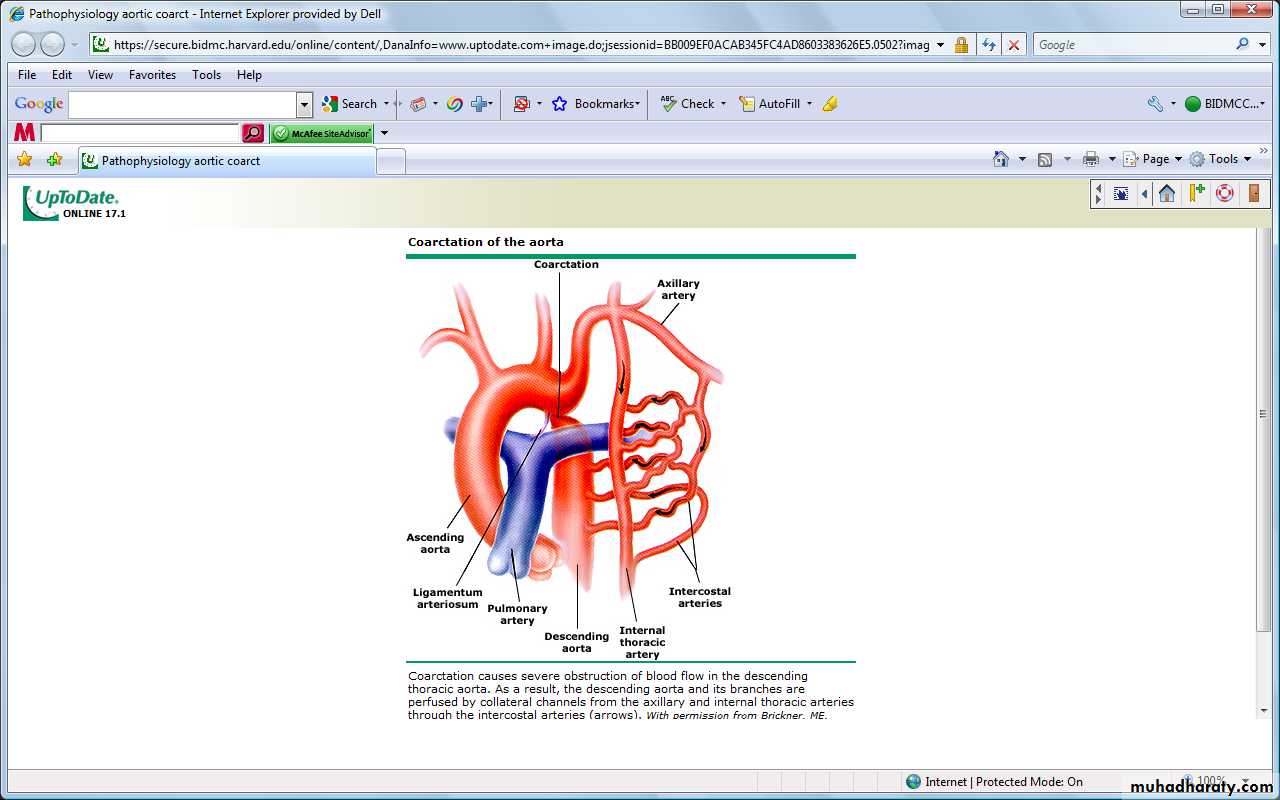
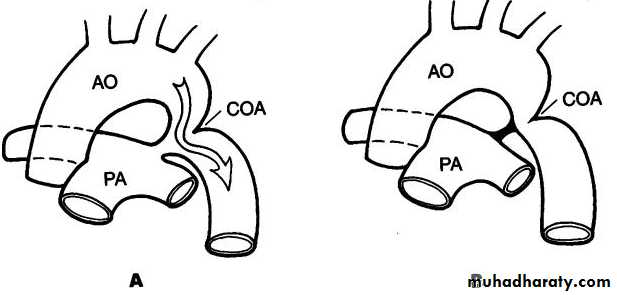
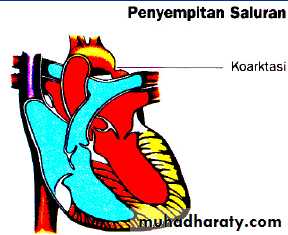
Definition
Is an obstruction in the descending aorta located typically near the aortic attachment of the ductus arteriosis or ligamentum arteriosum.
Distal to left subclavian artery
Rarely long segment or tubular hypoplasia occur
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH61
COARCTATION OF THE AORTA (cont.):
• occurs in 6-8% of congenital heart disease.• More common in males with M:F = 2:1.
• Could be associated with others sydromes or CHD
• More common cardiac lesion in Turner syndrome.
• Mostly sporadic but could be familial
•
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
62
Coarctation of Aorta
Clinical features & diagnosis1. Infancy
In infants, usually presented with congestive heart failure, dyspnoea, poor feeding.
2. Childhood
* Asymptomatic without significant associated lesion
* Hypertension (90%) * Cardiomegaly (33%)
* Rib notching (15%)
3. Adolescence and adult
* Hypertension ; very common * Valvar heart disease
* Heart failure at 30 years of age
4. Associated syndrome
* Turner syndrome (XO) : 2% * Von Recklinghausen’s D
* Noonan’s syndrome or congenital rubella
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
63
Diagnostic Approach
• History and examination• Diagnostic tests
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH64
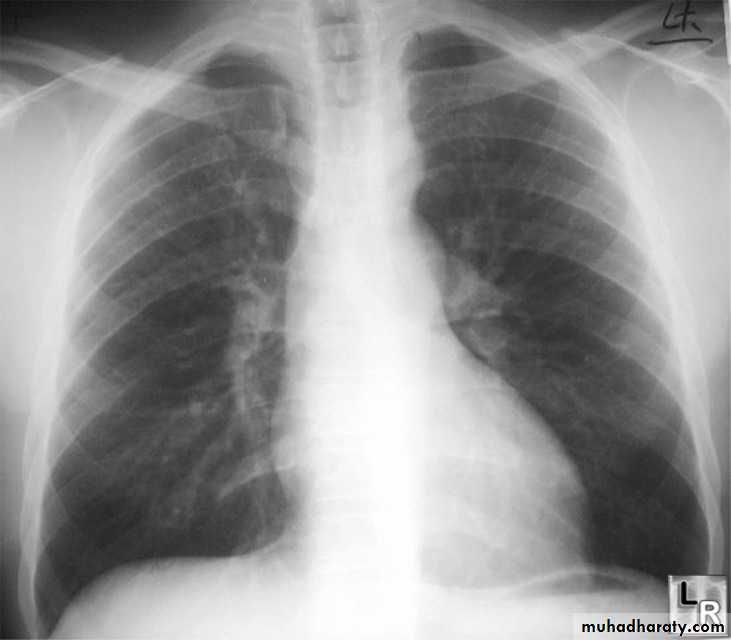
CXR
Infants with severe disease: cardiomegaly, heart failure
Notching posterior ribs: erosion by collaterals
“3” Sign: Indentation of aortic wall with pre and poststenotic dilatation
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH65
COARCTATION OF THE AORTA (cont.):
Rx:
• Balloon coarctation angioplasty native or recurrent (previously).
• Surgery by end to end anastomosis.
Prognosis:
The mean age for untreated coarctation is about 34 years and the most common cause of death are: heart failure, aortic rupture, infective endocarditis, intracranial hemorrhage (due to B.P. or aneurysm).
12/31/2015

Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
66Main Menu
SADIQ M. AL-HAMASHProfessor
M.B.Ch.B.; F.I.C.M.C.S. (Pediatrics); F.I.C.M.S. (Cardiology)
PULMONARY STENOSIS
12/31/2015
Pediatric Cardiology...Assist. Prof. SADIQ M. AL- HAMASH67
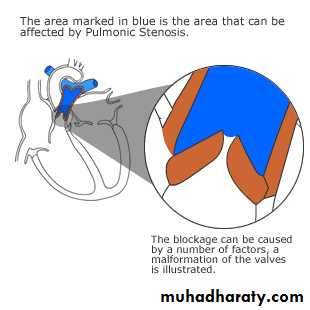
Definition…. Pulmonary stenosis
Congenital obstruction to right ventricle outflow can originate in the pulmonary valve (most common ) or can reside below or above the pulmonary valve.12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
68
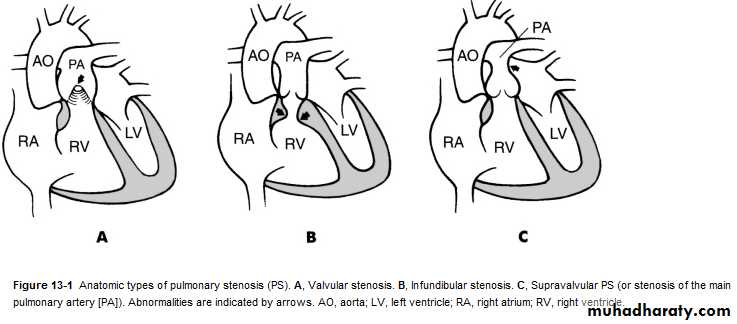
PULMONARY STENOSIS (cont.):
• Anatomical classification:• Valvular 90%
• Subvalvular
• supravalvular
Valvular stenosis
supravalvular stenosis
subvalvular stenosis
10%
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
69PULMONARY STENOSIS (cont.):
Classification according to severity:12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
70
PULMONARY STENOSIS (cont.):
• C/F:• Most patients are asymptomatic and discovered accidentally.
• Symptoms: exertional dypnoea and sometime chest pain.
• O/E:
• The asymptomatic patient has normal growth unless it is a severe case.
• In symptomatic patients:
• S1 is normal.
• Non-fixing splitting S2.
• Multiple systolic ejection click at pulmonary areas.
• Ejection systolic murmur with thrill (i.e. > grade 4), maximally at pulmonary area.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
71
PULMONARY STENOSIS (cont.):
• ECG: Rt. Axis deviation & peaked P-wave.
• Echo:
• For Dx
• Severity determination
• Level of stenosis (supra, valvular or sub).
• Catheterization:
• Diagnostic and therapeutic.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
72
PULMONARY STENOSIS (cont.):
• Rx:• Mild: just reassurance.
• Moderate to severe: balloon valvuloplasty;
• if failed surgical valvotomy.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
73
BPV
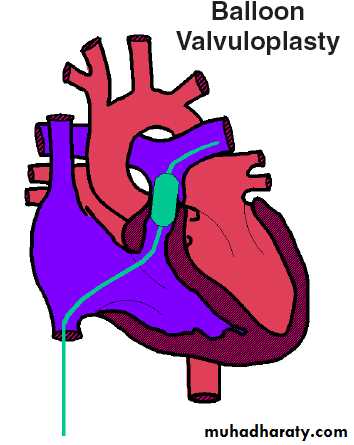
Balloon Dilatation of Pulmonic Valve
12/31/2015Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
74
AORTIC STENOSIS
SADIQ M. AL-HAMASH
ProfessorM.B.Ch.B.; F.I.C.M.C.S. (Pediatrics); F.I.C.M.S. (Cardiology)
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
75
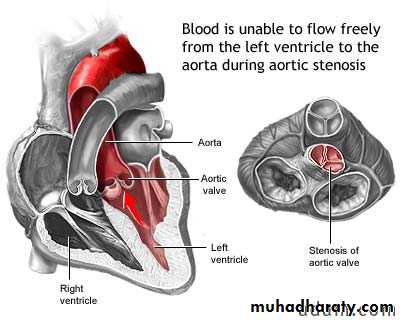
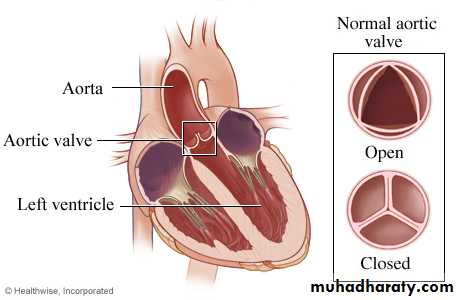
Definition
Congenital obstruction to blood flow from left ventricular outflow tract to Aortarepresents up to 10% of all CHDs.
Aortic valve stenosis occurs more often in males (male/female ratio of 4:1).
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH76
Clinical Manifestations
Children with mild to moderate AS are usually asymptomatic.In severe cases-chest pain or dyspnea, easy fatigability and syncope may occur in infants with critical stenosis of aortic valve.
They may also develop CCF in the first few months of life.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
77
On examination
acyanotic with normal growth and development.In severe aortic stenosis-‘
• anacrotic' pulse with narrow pulse pressure,
• systolic thrill over the upper right sternal border radiating to the carotid arteries.
• Pre-systolic tap indicates forceful atrial contraction over precordium.
• On auscultation-in severe AS-an ejection click with paradoxical splitting of S2.
• A harsh ejection systolic murmur heard over 2-3rd left intercostal space radiating to the neck.
In presence of aortic regurgitation, a decrescendo diastolic murmur may be present
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
78
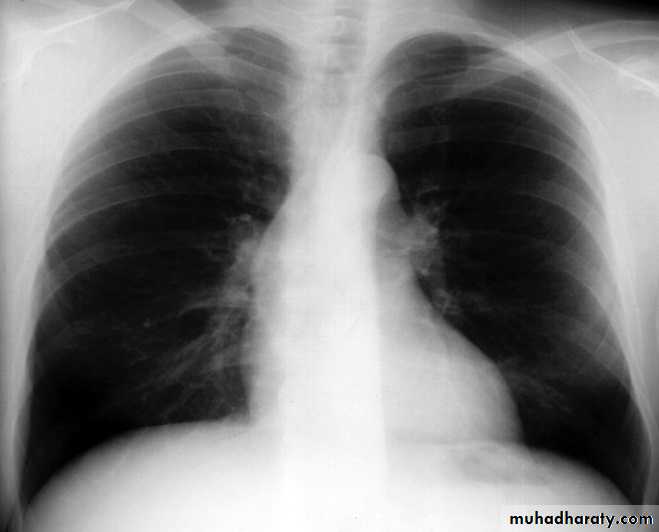
Investigation
1. Electrocardiography1. Left ventricular hypertrophy (LVH) with strain in severe aortic stenosis .
2. Exercise induced ischemic ST changes likely to reflect subendocardial ischemia owing to an imbalance in oxygen balance.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH79
AS ..cont.
2. X-ray Studies1. Cardiac size is usually normal.
2. If AR is also associated then cardiomegaly may develop.
3. Left atrial enlargement suggests severe aortic stenosis.
4. Critical AS in newborns-generalized cardiomegaly with pulmonary venous congestion.
5. Ascending aortic enlargement common finding in older children.
3. Echocardiography with doppler
4. cardiac catheterization
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
80
Management
Medical1. Management of good oral and dental hygiene and antibiotic prophylaxis against bacterial endocarditis is mandatory.
2. Children with moderate to severe AS should not perform sustained strenuous activities.
3. Percutaneous balloon valvuloplasty may be tried to relieve the stenosis, though the results are not good as those for PS and subsequent progression of stenosis or regurgitation is expected.
Surgical
1. Closed aortic valvotomy-
2. Aortic valve replacement-
3. In some centers, Ross procedure is the preferred option particularly in small children. In this procedure the child's pulmonary valve is translocated to the aortic position and a pulmonary homograft implanted.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
81
Cyanotic Heart Lesions
12/31/2015
Pediatric Cardiology...Assist. Prof. SADIQ M. AL- HAMASH
82
SADIQ M. AL-HAMASH
Professor
M.B.Ch.B.; F.I.C.M.C.S. (Pediatrics); F.I.C.M.S. (Cardiology)
CYANOSIS IN CHILDREN
Central cyanosis:Cyanosis of the tongue,mucous membranes and peripheral skin, it is necessary to have >5g/dl of reduced Hb to have it.
Peripheral cyanosis:
It is visible only in the skin of the extremities with normal arterial saturation due to vasomotor instability,ex. cold environment.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
83
CAUSES OF CENTRAL CYANOSIS
• Congenital Heart Disease•
• 1) Cyanosis with PBF 2) Cyanosis with PBF
•
• a) TOF a) D-TGA
•
• 12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
84
Main Menu
SADIQ M. AL-HAMASH
ProfessorM.B.Ch.B.; F.I.C.M.C.S. (Pediatrics); F.I.C.M.S. (Cardiology)
TETRALOGY OF FALLOT (TOF)
12/31/2015
Pediatric Cardiology...Assist. Prof. SADIQ M. AL- HAMASH85
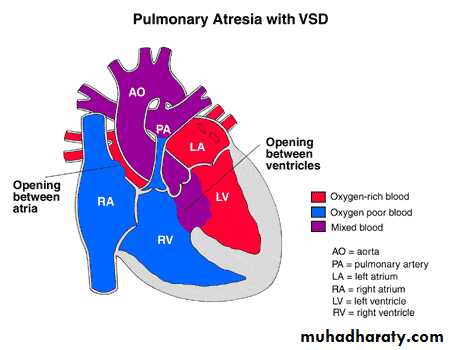
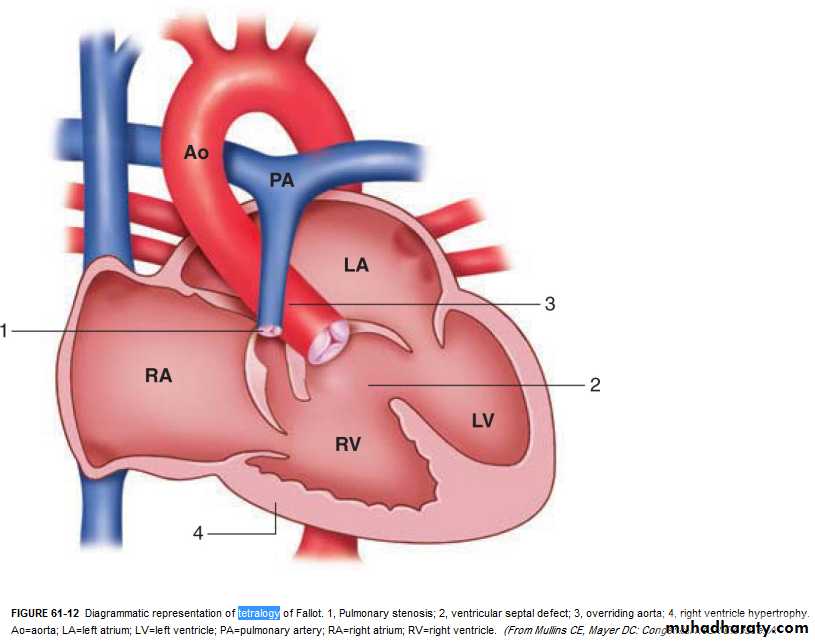
TETRALOGY OF FALLOT (cont.):
• It is the “commonest” cyanotic congenital heart disease in children and adults. It is a combination of:• VSD
• Pulmonary stenosis (PS).
• Overriding of aorta.
• Right ventricular hypertrophy (RVH).
•
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH86
TETRALOGY OF FALLOT (cont.):
• Hemodynamics:• The degree of right ventricular outflow obstruction (i.e. P.S.) determines the degree of pulmonary blood flow and the severity of cyanosis.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
87
TETRALOGY OF FALLOT (cont.):
C/F:1、Cyanosis:central,worsen when exercise or fast breathing.
most patients develop cyanosis in the first 6 month – 1 year of life.
2、Squatting:seen older children
it is the characteristic posture of children with TOF after any
physical effort
3、Clubbing fingers(toes)
4、Anoxic spell
5、Delayed growing( Failure to thrive)
6、Dyspnea

12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH88
TETRALOGY OF FALLOT (cont.):
• O/E:Cyanosis (central and peripheral).
Clubbing (usually after 3 months of age).
Single S2 & ejection systolic murmur at the left sternal border.
Normal pulse & quiet precardium.
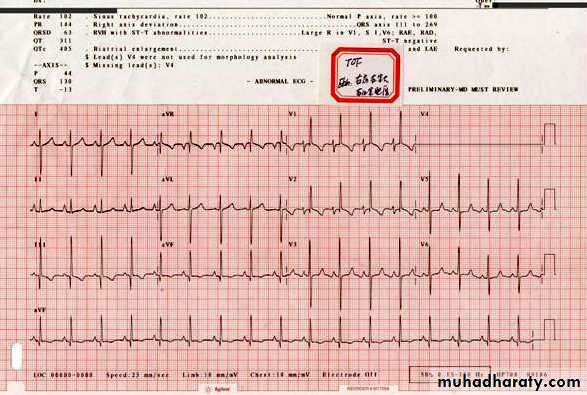
• ECG: Right axis deviation (RAD) & right ventricular hypertrophy (RVH).
12/31/2015

Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
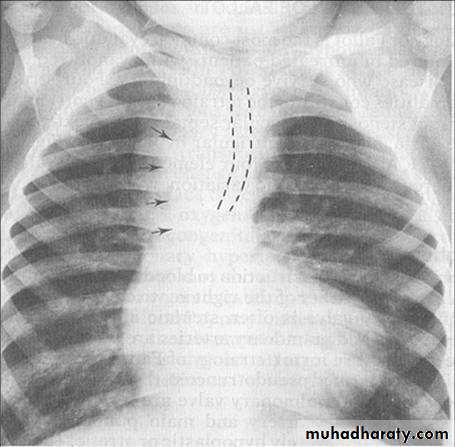
89TOF x-ray findings
Normal heart size.
1、Upturned apex
( RV hypertrophy)
2、The absence of main PA segment gives it the shape described as boot shape .
3、Pul. Fields are oligemic.
(decrease pulmonary vasculature, clear lung fields)
12/31/2015
90ECG
Right axis deviation
RV hypertrophy
RA hypertrophy
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
91
TETRALOGY OF FALLOT (cont.):
• Echo: It is essential for Dx.• Catheterization: Gives the definitive Dx and as a preoperative step.
•
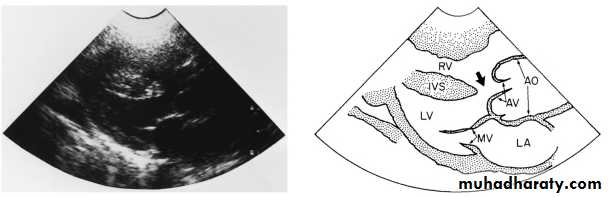
Echo: PLAX view showing TOF.
12/31/2015Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
92
TETRALOGY OF FALLOT (cont.):
• Complications:• Hypercyanotic spells.
• Cerebrovascular accidents (CVA).
• Cerebral abscess.
• Infective endocarditis.
• Hematological complications include bleeding and thrombosis.
• All complications are essentially due to cyanosis & polycythemia.
• Polycythemia is due to hypoxia which results from right to left shunt (as the right pressure grows higher than the left one).
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
93
TETRALOGY OF FALLOT (cont.):
• Rx:
• Medical:
• Rx of anemia by iron, sometimes considered as relative anemia if we find normal Hb level; also nutritional support.
• Phlebotomy: in symptomatic patients with hematocrit more than 65% (as there is a risk for CVA).
• B-Blocker
• Surgical:
• Palliative to pulmonary blood flow e.g.: Blalock-Taussig shunt (BT shunt).
• Total surgical repair.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
94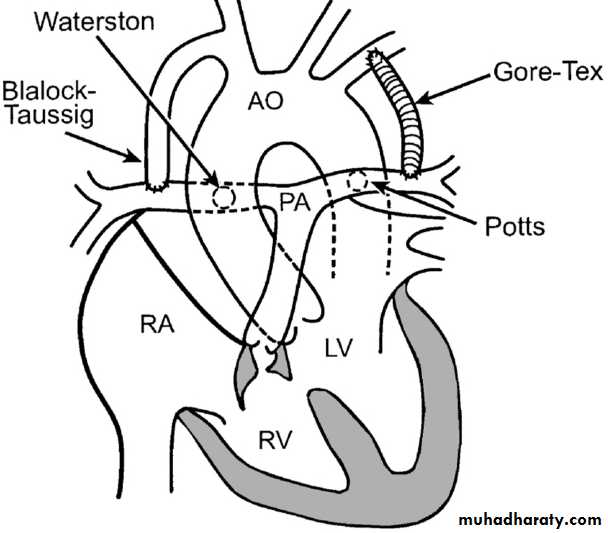
TETRALOGY OF FALLOT (cont.):
• Indications for surgery:• Cyanosis
• Hypercyanotic spells
• Polycythemia
• exercise tolerance
• Appropriate age and weight (usually between 2-3 years, if there is cyanosis).
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
95
TETRALOGY OF FALLOT (cont.):
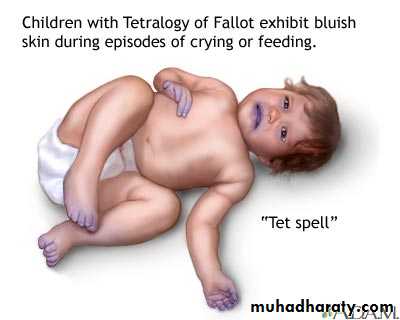
• Hypercyanotic spells:
• Attacks of increasing cyanosis associated with abnormal respiration and altered level of consciousness and it is an important cause of death in TOF patients (especially in mild cyanosis).
• Spells are particular problems during the 1st 2 years of life and is more common in the morning and can be precipitated by any activity. Most spells are self-limited, but should be considered as an indication for surgery.
• The cause is infundibular spasm.
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH
96TETRALOGY OF FALLOT (cont.):
• Rx:• Knee-chest position.
• O2.
• Sodium bicarbonate to correct metabolic acidosis.
• Morphine: 0.2 mg/Kg subcutaneously (s.c.) or i.v. can be repeated 4 hourly.
• B-blocker: propranolol (inderal) given 0.1-0.2 mg i.v. and can be given orally (1-2 mg/Kg/day) as a prophylaxis against the spells (given in 2 divided doses to patients not indicated for surgery).
• Surgery: emergency surgical intervention may be necessary in severe spells resistant to medical Rx.
12/31/2015
Pediatric Cardiology...Assist. Prof. SADIQ M. AL- HAMASH
97
Main Menu
SADIQ M. AL-HAMASHProfessor
M.B.Ch.B.; F.I.C.M.C.S. (Pediatrics); F.I.C.M.S. (Cardiology)
TRANSPOSITION OF GREAT ARTERIES (TGA)
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH98
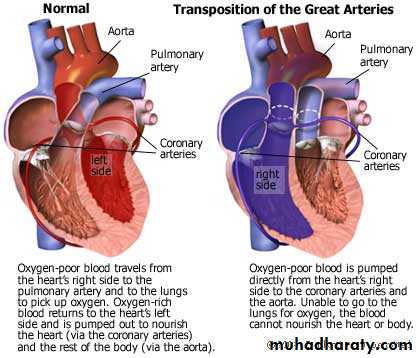
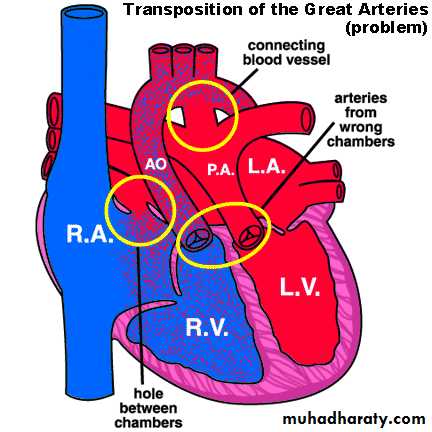
Complete Transposition of the Great Arteries
Systemic and pulmonary circulation run in parallel need for a communication between the two – circulatiom via ASD, VSD (most common), or PDA to support lifeIf circulatory mixing via PDA, its physiological closure abrupt cyanosis and deterioration need for Rashkind atrial balloon septostomy until definite surgery
RA -> RV -> Ao
ASD PDA
LA -> LV -> PA
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH99
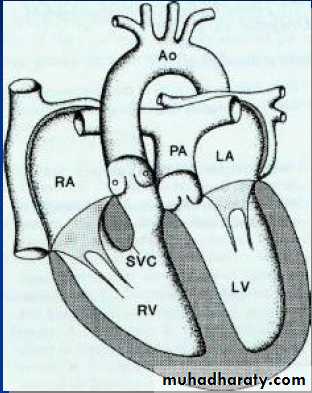
TRANSPOSITION OF GREAT ARTERIES (cont.):
One of the most common cyanoticdefects in the newborns
• 6% of CHD.
• M:F is 2:1
• More common in infants with DM mothers.
• In TGA, there is Ventriculoarterial discordance.. aorta & RV, pulmonary artery and LV.
• Aorta on the right and anterior
12/31/2015
Pediatric Cardiology... Prof. SADIQ M. AL- HAMASH
100
TRANSPOSITION OF GREAT ARTERIES (cont.):
• Clinical features:• Cyanosis and tachypnoea in the first hours or days of life.
• Prognosis:
• Without surgery, 90% will die within the first year of life.
• If corrected by Rashkind septostomy, 90% will survive.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
101
TRANSPOSITION OF GREAT ARTERIES (cont.):
• CXR:• Mild cardiomegaly with “egg-shaped side” of heart with a narrow base and increase in pulmonary vascularity.
•

12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
102
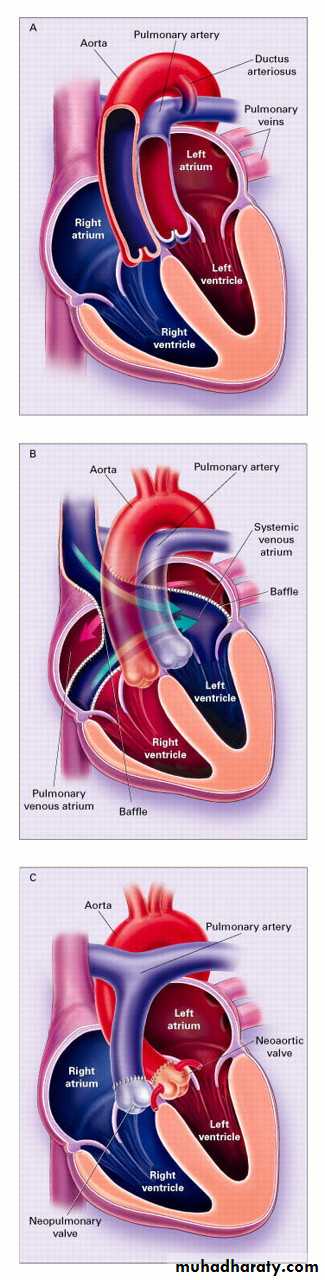
Transposition – Diagnosis and Treatment
TreatmentBalloon septostomy during cardiac cath.
Rashkind’s Procedure
Reestablish Foramen Ovale
Prostaglandin E1 to keep PDA open.
Surgical Correction
Jantene Operation
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
103
TRANSPOSITION OF GREAT ARTERIES (cont.):
• Correction:• Corrective anatomical surgery ( arterial switch )if it is to be done in the first month of life; if not, then only physiological correction i.e. switch the systemic venous return to the LV and the pulmonary venous return to the RV so the RV will pump blood to the body.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
104
Complete transposition (D-TGA) Atrial switch (Mustard/Senning)
Developed in the 1950sBaffle directs venous return to contralateral ventricle
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH105
Main Menu
HEART FAILURE (HF)SADIQ M. AL-HAMASH
Professor
M.B.Ch.B.; F.I.C.M.C.S. (Pediatrics); F.I.C.M.S. (Cardiology)
12/31/2015
Pediatric Cardiology…. Prof. SADIQ M. AL- HAMASH106
HEART FAILURE (cont.):
• Heart failure:(failure to work or Pumping Blood)
• Heart failure (HF) is inability of myocardium to produce cardiac output to sustain metabolic body need.
• i.e. the cardiac output which is heart rate times the stroke volume is not enough to supply O2 & nutrients and other cellular essential building units, also it is not enough to remove the waste products generated by the cells. So heart failure will sequentially lead to tissue failure (ischemia) and those to be 1st affected are of the highest BMR heart, brain, and kidneys.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
107
HEART FAILURE (cont.):
Causes of HF according to age:12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
108
HEART FAILURE (cont.):
Causes of HF according to age (cont.):12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
109
HEART FAILURE (cont.):
• Pathophysiology:• There are several types of pathophysiologic alteration that if become sufficiently severe will compromise the COP; these pathophysiologic alterations include:
• preload or volume overload as in: Lt. Rt. Shunt, valvular insufficiency, severe anemia.
• after load or pressure overload as in: aortic stenosis, aortic coarctation, acute HPT.
• Myocardial abnormalities: this impair its contractility as in myocarditis, dilated cardiomyopathy.
• Diastolic dysfunction i.e. Impaired ventricular filling so this reduce stroke volume as in: hypertrophic cardiomyopathy, tachy-dysrrhythmias.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
110
HEART FAILURE (cont.):
• C/F:• Hx is important in both Dx and evaluation of HF, and knowing the cause of HF.
• In infants:
• Feeding difficulties (less volume per feeding).
• Dyspnoea (crying, milk or formula sucking).
• Profuse sweating, irritability.
• Poor weight gain.
• Weak cry and noisy labored respiration.
• In children (as in adult C/F):
• Fatigue, effort intolerance, anorexia, cough, dyspnoea, abdominal pain which is due to (hepatic capsule stretching or intestinal vascular congestion).
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
111
HEART FAILURE (cont.):
• O/E:• Infant with HF:
• Weak peripheral pulse, narrowed pulse pressure (pulse pressure = systolic – diastolic B.P.)
• Tachycardia, Gallop rhythm i.e. S1,2,3, + S4, murmur of the cause.
• Rhonchi due to compressed airway by congested pulmonary vessel.
• Basal crepitations which may be due to respiratory infection.
• Peripheral edema is rare in infant.
• In children facial edema, and edema of dependant body part is more common than peripheral edema.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
112
HEART FAILURE (cont.):
• Compensatory mechanism against HF:
• Enlarged myocardial contractility with increased filling volume. This is “frank-starling law”.
• Hypertrophy of myocardium.
• Activation of rennin-angiotensin system.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
113
HEART FAILURE (cont.):
• Dx:• CXR: the most important to look for is heart size, pulmonary vascular shadow this is usually elevated, frank pulmonary edema is rare in children.
• ECG: non specific but it is helpful in assessing the cause but it does not confirm the Dx. So, ECG is best to evaluate rhythm disorder as a cause of heart failure.
• Echo: to diagnose structural defect, assess myocardial function by determining stroke vol., end-systolic vol., End-diastolic vol.
• Blood gases & pH: to assess severity of HF& to follow up the patients.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
114
HEART FAILURE (cont.):
• Rx of HF: Aims are:• Improve myocardial performance by digoxin (digitalis).
• Relief of pulmonary and systemic venous congestion by diuretic and vasodilator.
• Rx of underlying cause.
General Rx measures:
Bed rest.
Semi-up right position.
Diet.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
115
HEART FAILURE (cont.):
• Medical Rx:• 1. Digoxin: it remains the most widely used pharmacologic agent in Rx of HF in infant and children, it is +ve inotropic agent i.e. increases myocardial contractility.
• Mechanism of action: Inhibit Na+-K+ pump so intracellular Na+ and indirectly Ca+2 this Ca+2 increase the myocardial contractility.
• Slowing heart rate by direct effect on AV-node and by vagus N. stimulation and by anti-adrenergic effect.
• Metabolism:
• t1/2 = 36 hr., eliminated by kidney.
• Cross placenta so it can be used for fetus also.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
116
HEART FAILURE (cont.):
• Dose:• There is individual variation in response to drug.
• Infants tolerate larger doses than adults.
• Don't exceed the adult dose 1-1.5 mg
• Digitalization dose is 0.04-0.06 mg/Kg/day, we give 1/2 dose immediately and succeeding 2 doses 8-16 hrs later.
• Maintenance dose is 0.01 m/Kg/day. This should be started 12 hr after full digitalization.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
117
HEART FAILURE (cont.):
• Toxicity:
• Incidence is low in infant and children and can occur without systemic manifestations. Features of toxicity are:
• Cardiac:
• brady-arrhythmia is commoner in young.
• AV block is commonest toxicity sign.
• Ventricular fibrillation & death may occur.
• Extra-cardiac:
• N. & V., anorexia, visual disturbance.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
118
HEART FAILURE (cont.):
• Factors that potentiate toxicity:• Prematurity
• Myocarditis
• Hypokalemia (k+ should be > 2.5 mg).
• Hypercalcemia
• Renal and hepatic disease.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
119
HEART FAILURE (cont.):
• Mx of toxicity:
• Observation of serum digoxin level.
• Stop administration of digoxin.
• Correct any electrolyte disturbance.
• Atropine or pacemaker for patients with bradycardia.
• Digoxin Fab antibody effect appear in 30-40 min.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
120
HEART FAILURE (cont.):
• 2. Diuretic:• Loop diuretic as frusemide 1-2 up to 2-4 mg to preload.
• 3. Vasodilators:
• ACE inhibitors captopril 0.6-6 mg/Kg
• Angiotensin II receptor blockers.
• 4. Inotropic agent dopamine, dobutamine
• 5. Medical Rx for underlying cause (e.g.. closing the VSD)
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
121
Main Menu
CARDIOMYOPATHY
SADIQ M. AL-HAMASH
Professor
M.B.Ch.B.; F.I.C.M.C.S. (Pediatrics); F.I.C.M.S. (Cardiology)
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH122
CARDIOMYOPATHY (cont.):
• It is a disease of the heart muscle itself, not associated with congenital, valvular, or coronary heart disease or systemic disorders. It is distinct from the specific heart muscle diseases of known cause.• It is either idiopathic or due to infection.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
123
CARDIOMYOPATHY (cont.):
Functional Classification of cardiomyopathy:12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
124
CARDIOMYOPATHY (cont.):
• Dilated Cardiomyopathy (DCM):
• In which there is myocardial dysfunction and ventricular dilatation.
• Causes:
• Idiopathic
• Viral infection Coxachi virus.
• Genetic
• Metabolic Beri Beri and carnitine deficiency
• Drugs adriamycin
• Autoimmune disease as SLE.
• Congenital .
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
125
CARDIOMYOPATHY (cont.):
• Clinical features:• Symptoms:
• Orthopnoea
• Dyspnoea
• Paroxysmal nocturnal dypnoea
• Then RV failure occurs. So, edema, pulsus alternans occurs.
• Signs:
• Gallop rhythm
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
126
CARDIOMYOPATHY (cont.):
• CXR: cardiomegaly, plethoric lung
• ECG:
• LVH; Sinus tachycardia, and ST-T changes are the most common findings. Left or right atrial hypertrophy (LAH or RAH) may be present.
• Atrial or ventricular arrhythmias and atrioventricular (AV) conduction disturbances may be seen.
• Echo: is the most important tool in the diagnosis of the condition and is important in the longitudinal follow-up of patients.
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
127
CARDIOMYOPATHY (cont.):
• Death occurs due to:• Dysrrhythmia
• Severe HF
• Severe resp. infection
• Thromboembolism
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
128
CARDIOMYOPATHY (cont.):
• Rx:• Rx the cause.
• Rx HF by inotropics, vasodilators, diuretics.
• Antiplatelet (aspirin), anticoagulant (warfarin)
• Anti-arrhythmic
• B-blockers metoprolol & carvidolol
• Carnitine
• Ventricular assisted device
• ICD
• Heart transplant
12/31/2015
Pediatric Cardiology.... Prof. SADIQ M. AL- HAMASH
129