Dr.Athal CNS3
HeadacheDDX
Migraine
Tension headache
↑ ICP
Headache and migraine
Worrisome headachemost severe on awakening.
that awaken the patient in the middle of night.
severely exacerbated on coughing or bending.
acute without previous history.
present daily & getting progressively more severe.
associated with vomiting.
Migraine headache
Common migraine (with out aura):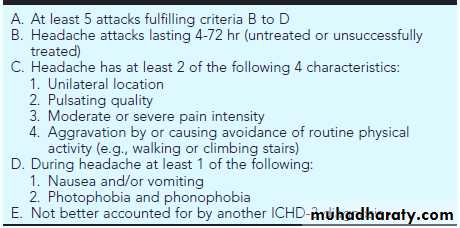
ICHD-3: The International Classification of Headache Disorders, ed 3
Precipitating factors:by menstruation
after heavy exercise.
psychological stress.
lack of food or sleep.
food or drugs(cheese,chocolate, oral C.C pill)
Relieve with sleep.
Diagnosis of migraine
History & physical examination.Lipid profile
Radiological study (CT and MRI) to rule out any SOL.
Treatment of migraine
Non medical :elimination of precipitating factor.
reassurance.
psychotherapy.
Drugs Therapy :
Analgesia :
acetaminophen.
NSAIDS
Minor tranquilizers:
benzodiazepam
antihistamine
barbiturate
Serotonin agonist:
Triptans
Antiemetics:
metocloppramide
promethazine
Prophylactic agents:
TCA (Amitriptyline )
Beta-blocker (Propranolol )
Calium channel blocker (Flunarizine)
Anticonvulsants : Valproic acid.
Antihistamines : Cyproheptadine.
Migraine variants
Cyclic vomitingAbdominal migraine
Basilar-type migraine
Benign paroxysmal vertigo.
Cyclic Vomiting
Mainly occur in infant and young children.Recurrent vomiting (dehydration with electrolyte disturbance).
Systemic manifestations such as fever, abdominal pain, and diarrhea are initially absent, but they may become prominent in association with excessive fluid losses secondary to vomiting.
Pallor, fright follow by deep sleep→releave symptoms.
Family history of migraine.
Typical migraine headache in future.
Treatment:
1- Fluid replacement.
2- Rectal antiemetics (ondansetron)
D.Dx: (intestinal obstruction, peptic ulcer, IBD ,IEM ,CNS lesion).
Abdominal migraine
It is a recurrent disorder characterized by mid-abdominal pain with pain-free periods between each attack. The pain is usually described as “dull” and may be moderate to severe. The pain may persist from 1 to 72 hr and, although usually midline, may be periumbilical or poorly localized by the child.
To meet the criteria of abdominal migraine, the child must complain at the time of the abdominal pain of at least two of the following: anorexia, nausea, vomiting, or pallor.
As with cyclic vomiting, a thorough history and physical examination with appropriate laboratory studies must be completed to rule out an underlying gastrointestinal disorder as a cause of the abdominal pain.
Basilar-type migraine
It is considered to represent a precursor of childhood migraine. Brainstem signs predominate in these patients because of vasoconstriction of the basilar and posterior cerebral arteries.The major symptoms include: ataxia, vertigo, tinnitus, diplopia, blurred vision, scotoma,, and an occipital headache. The pupils may be dilated, and ptosis may be evident. Alterations in consciousness followed by a generalized seizure may result.
Tension headache
Daily with work or school.
Present all the day with worsening in afternoon
Moderate band-like pain.
Multiple somatic symptoms (SOB, abdominal pain, dizziness).
Increased intracranial pressure
↑ICP is both a symptom of serious intracranial pathology and a cause of irreversible neurological injury.The skull is rigid container enclosing fixed volume, which include the brain which accounts for 80-85% of volume, CSF 10-15% & blood 5-10%.
Etiology:
mass lesion , hydrocephalus , brain swellingSymptoms:
headache, vomiting, lethargy, irritability, 6th nerve palsy, diplopia, papillodema except in infant due to bulging fontanel?
Sign:
bulging fontanel , suture diastasis , distended scalp veins , sun set eyes , rapid growth of OFC.FND will reflect the site of the lesion producing the ↑ICP .
Cushing triad :a late sign of critically ↑ICP & include ↑ BP, ↓pulse, irregular respiration.
Brain herniation:
It occur when the brain shift in response to the continuing elevation of ICP, transtentorial & foramen magnum herniation are immediately life threatening & indicate critically raised ICP.Brain Abscess
It causes ↑ICP by :1-large size 2-blockage of CSF 3- blockage of venous outflow
4-cerebral edema (vasogenic edema)
Etiology:
chronic cardiac or pulmonary disease by embolization.The responsible bacteria include streptococci,anaerobic organisms, and gram-negative aerobic bacilli.
Symptoms:
- focal neurological sign.
- ↑ICP- fever , malaise , anorexia , stiff neck.
Diagnosis :
CT scan (LP is contraindicated)Treatment :
A brain abscess can be treated with antibiotics (combination of vancomycin, a 3rd-generation cephalosporin, and metronidazole) without surgery if:the abscess is <2 cm in diameter.
the illness is of short duration (<2 wk).
there are no signs of increased ICP.
the child is neurologically intact.
If the decision is made to treat with antibiotics alone, the child should have weekly neuroimaging studies to ensure the abscess is decreasing in size.
An encapsulated abscess, particularly if the lesion is causing a mass effect or increased intracranial pressure, should be treated with a combination of antibiotics and aspiration.
Surgical excision of an abscess is indicated when:
the abscess is >2.5 cm in diameter.
gas is present in the abscess.
the lesion is multiloculated.
the lesion is located in the posterior fossa.
a fungus is identified.
The duration of antibiotic therapy depends on the organism and response to treatment, but is usually 4–6 wk.