DENTAL ANOMALIES
Dental anomalies include variations in normal number, size, eruption, or morphology of the teeth.*Developmental abnormalities: occurred during theformation of the tooth or teeth. Most of the defects considered are inherited.
*Acquired abnormalities: result from changes toteeth after normal formation.
Supernumerary.
Missing.Impaction.
Number and Eruption
Developmental abnormalities
• These are extra teeth that appear in addition to the regular number of teeth.
• Also called supplemental teeth: When they have normal morphology.
• Mesiodens :When they occur between the maxillary central incisors.
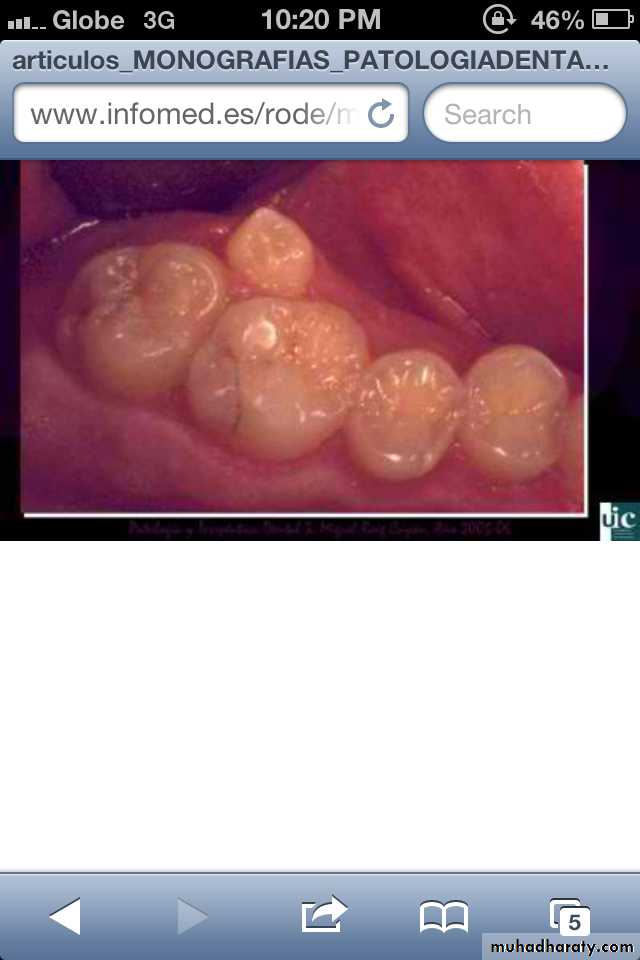
Parateeth(paramolar): Those occurring in the molar area .
Distodens or distomolar : Those that erupt distal to the third
molar.
Peridens supernumerary teeth: That erupt ectopically either
buccally or lingually to the normal arch .
• Common region of the jaws to be affected is the premaxilla.
Supernumerary teeth:

Paramolar blocking the eruption of 3rd molar.
Mesiodens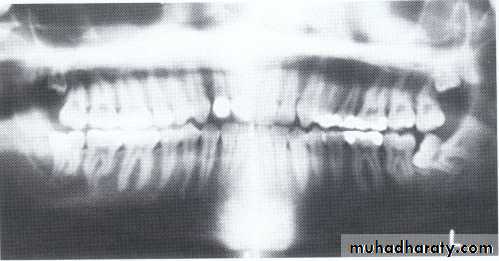
Distomolars(4th molar)

Mesiodens

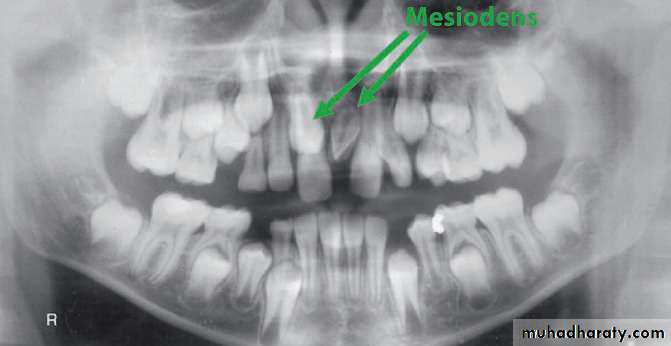
Mesiodens
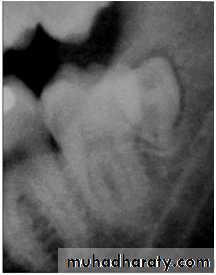
Distodens or distomolarParamolar

Supplemental
CAUSE: Is unknown, the tendency is familial. Most cases are polygenetic and represent initial spontaneous gene mutations. When the anomaly is re-stricted to supernumerary teeth, it is inherited as an autosomal recessive trait.
Many supernumerary teeth never erupt, but they may delay eruption of nearby teeth or cause other dental problems.
The TREATMENT is depend on:
Their potential effect on the developing normal dentition.
Their position and number, and the complications that may result from surgical intervention.
If they erupt, they can cause malalignment of the normal dentition.
They may cause root resorption or interfere with the normal eruption sequence.
Follicles of unerupted supernumerary teeth occasionally develop
into dentigerous cysts.
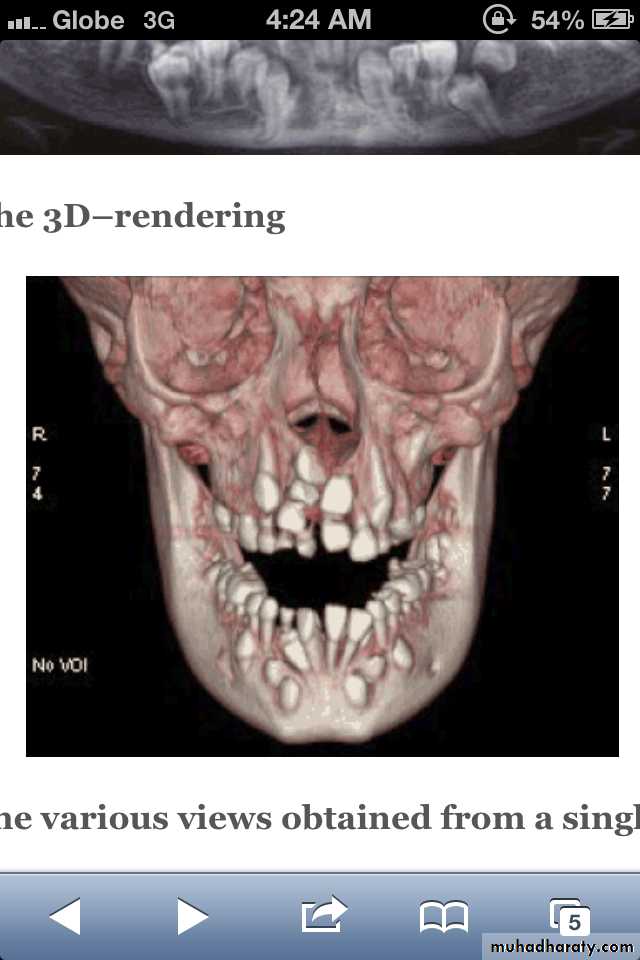
Supernumerary teeth characteristically found in cleidocranial dysostosis .
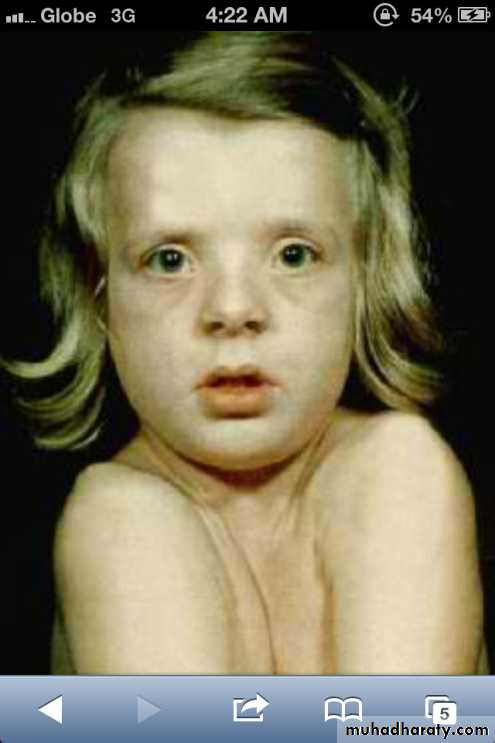
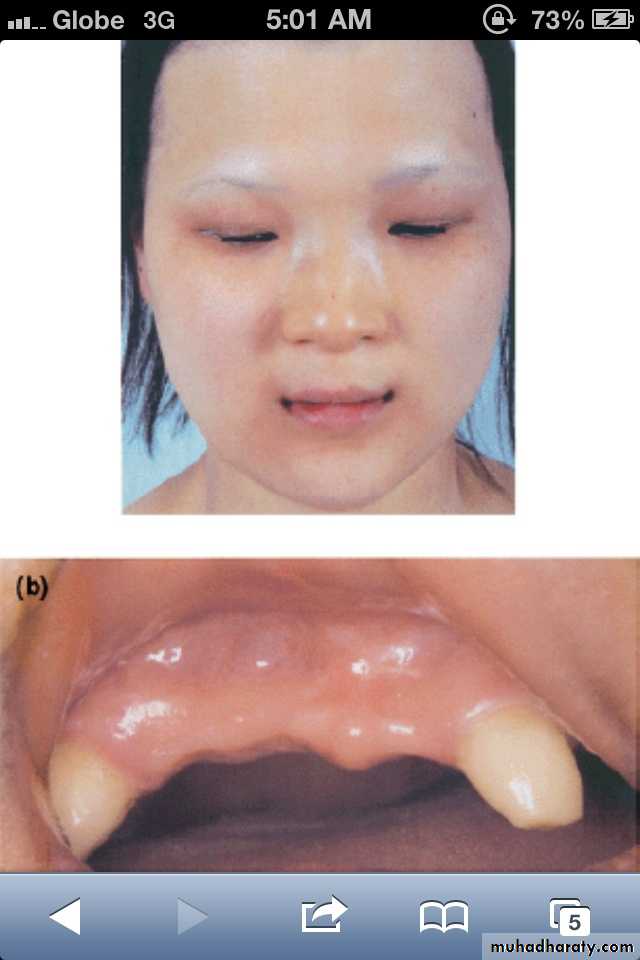
Missing teeth:
The expression of developmentally missingteeth may range from:
Hypodontia :the absence of one or a few teeth.
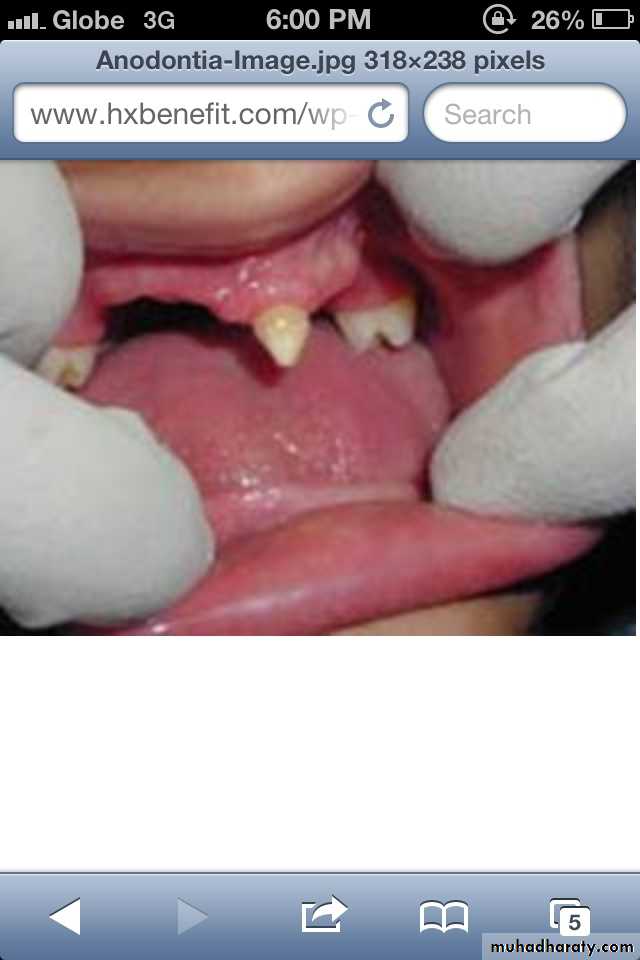
Oligodontia : the absence of numerous teeth .
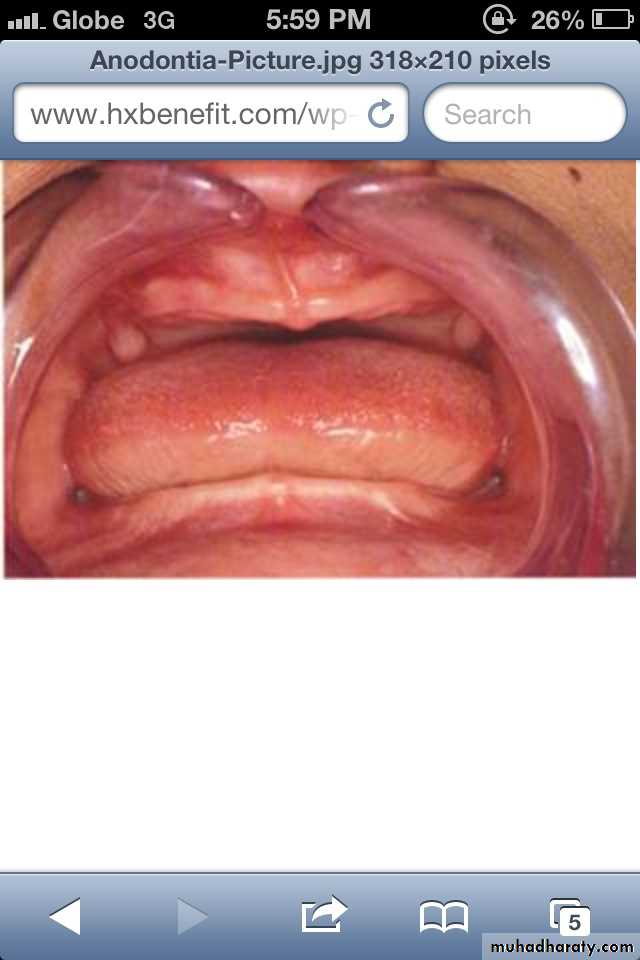
Anodontia : the failure of all teeth to develop .
Pseudoanodontia: when teeth are absent
clinically because of impaction or delayed eruption.
False Anodontia: when teeth have been
exfoliated or extracted.
*Anodontia or hypodontia associated with
systemic disease e.g. Down's syndrome,ectodermal dysplasia.
Hypodontia
Oligodontia
Anadontia
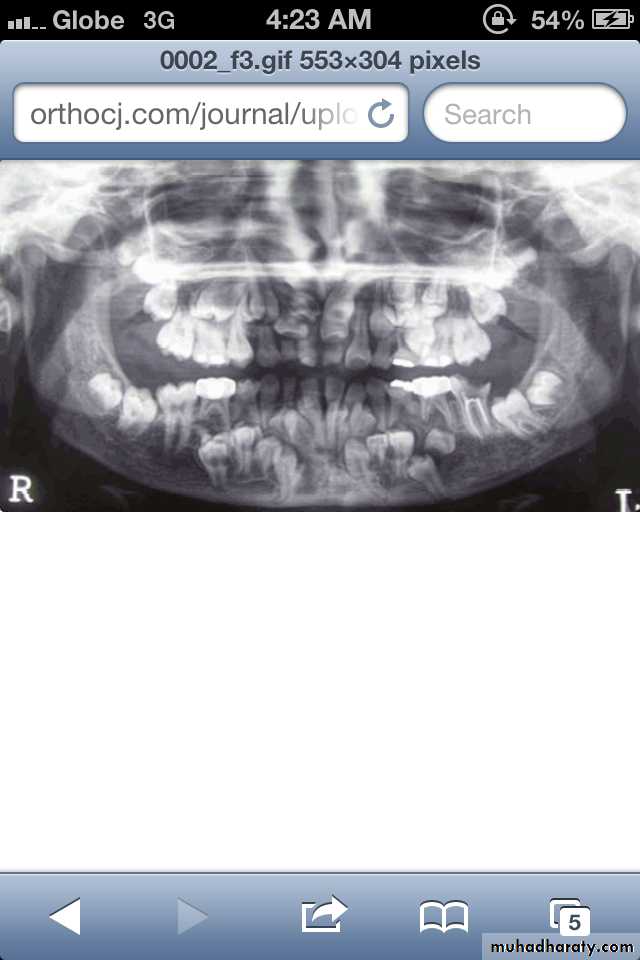
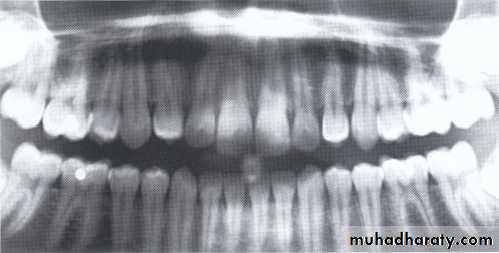
Developmental absence of all maxillary premolars and both mandibular second premolars. Note the retention of the maxillary primary canine as a result of the posterior position of the maxillary permanent canine.
CAUSES: may be the result of numerous independent pathologic mechanisms that can affect the orderly formation of the dental lamina (e.g.,orofaciodigital syndrome), failure of a tooth germ to develop at the optimal time, lack of necessary space imposed by a malformed jaw, and a genetically determined disproportion between tooth mass and jaw size.
MANAGEMENT: Missing teeth, abnormal occlusion, or altered facial appearance may cause patients psychologic
distress.
*Mild hypodontia by orthodontics.
*Severe cases by restorative,implant, and prosthetic procedures .
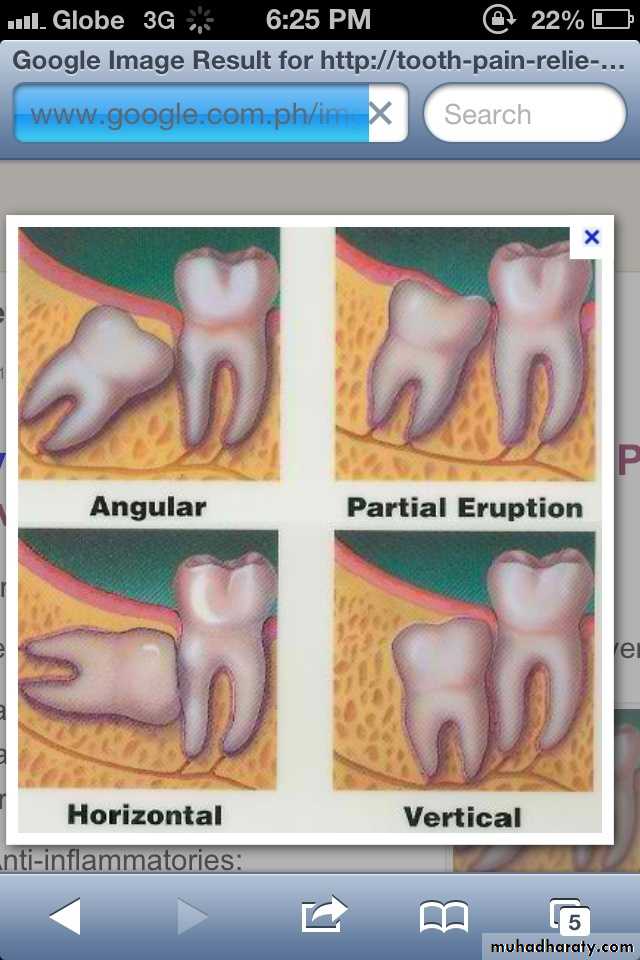
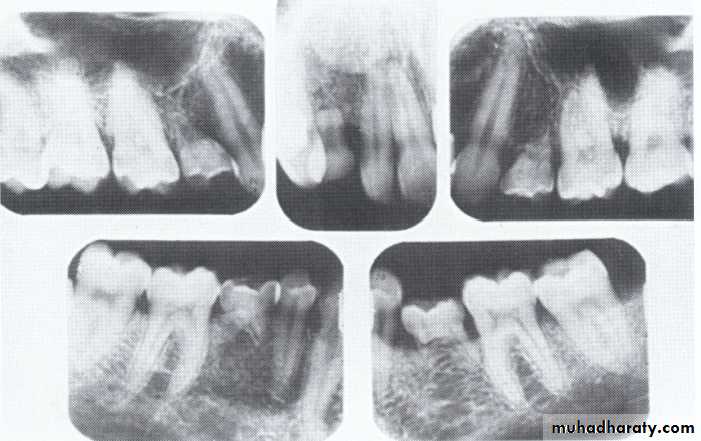
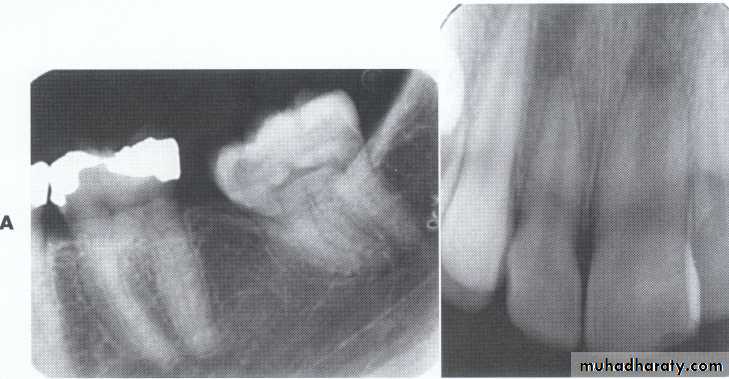
Impaction:
most often affects the mandibular 3rd molars &maxillary canines.
less commonly:
premolars
mandibular canines
second molars
CAUSES: due to obstruction from crowding.
occasionally, may be due to an abnormal eruption
path, presumably because of unusual orientation of
tooth germ.
Microdontia.
Macrodontia.Size
Microdontia:
(1) True Generalized Microdontia.
(2) Relative Generalized Microdontia.(3) Focal or Localized Microdontia.

All teeth are smaller than
normal.Occur in some cases of
pituitary dawrfism.
Exceedingly rare.
Teeth are well formed.
(1) True Generalized Microdontia

Normal or slightly smaller than normal teeth.
Are present in jaws that are somewhat larger than normal.(2) Relative Generalized Microdontia
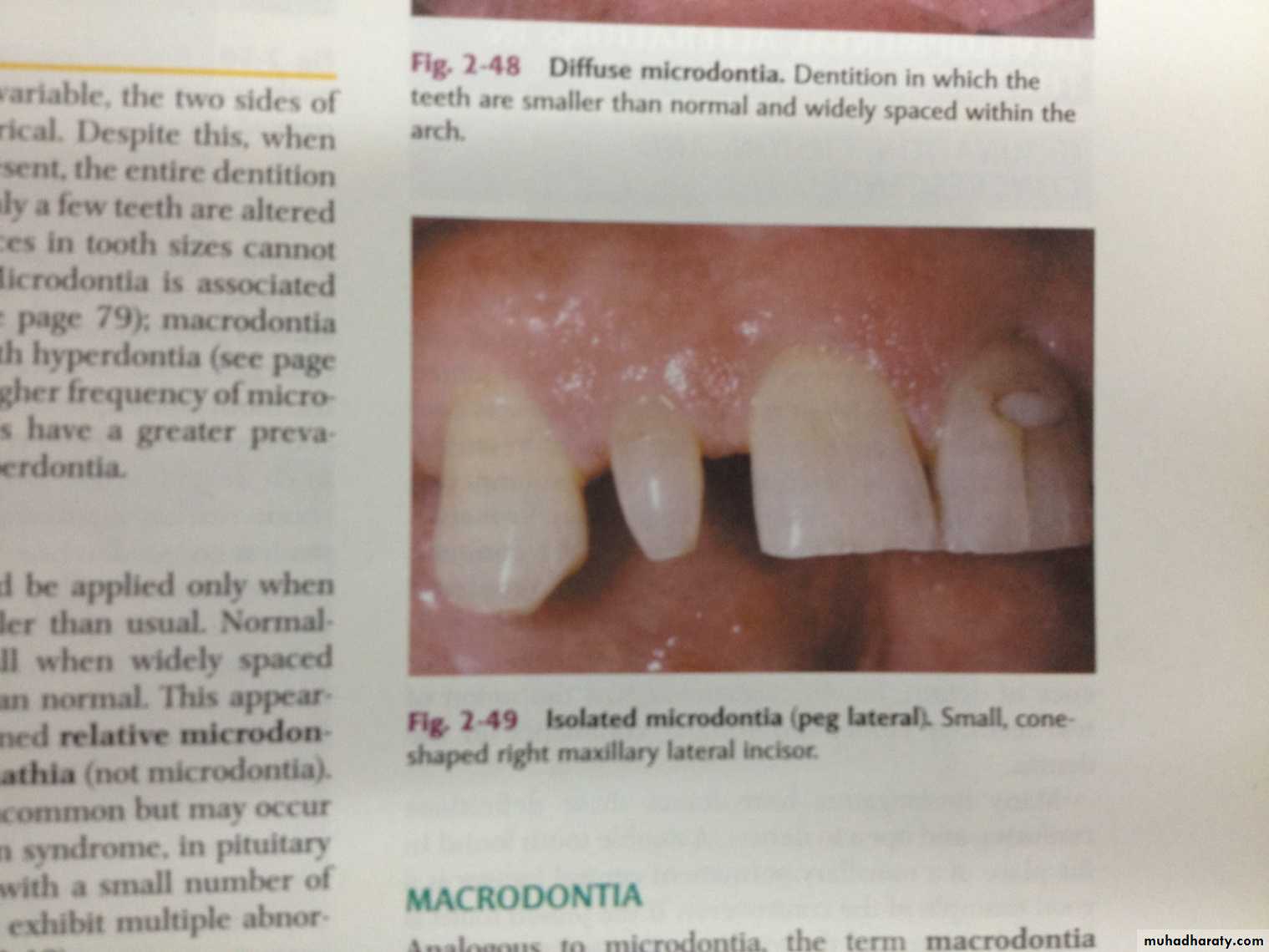
(3) Focal/Localized MicrodontiaCommon condition.
Affects most often maxillary
lateral incisior + 3rd molar.
These 2 teeth are most often
congenitally missing.

sides converge or taper
together incisallyforms cone-shaped crown
root is frequently shorter
than usual.
(3) Focal/Localized Microdontia
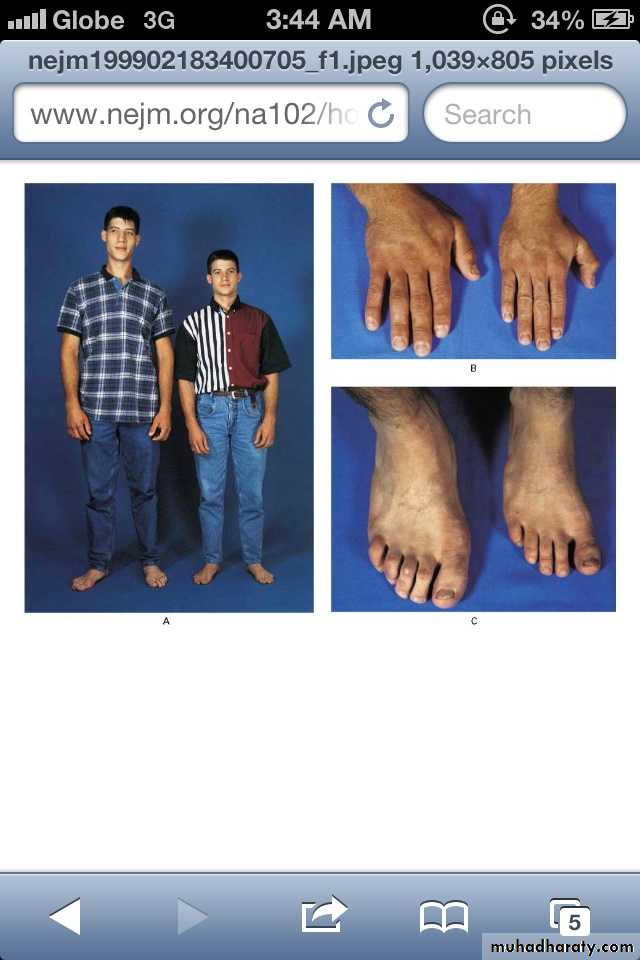
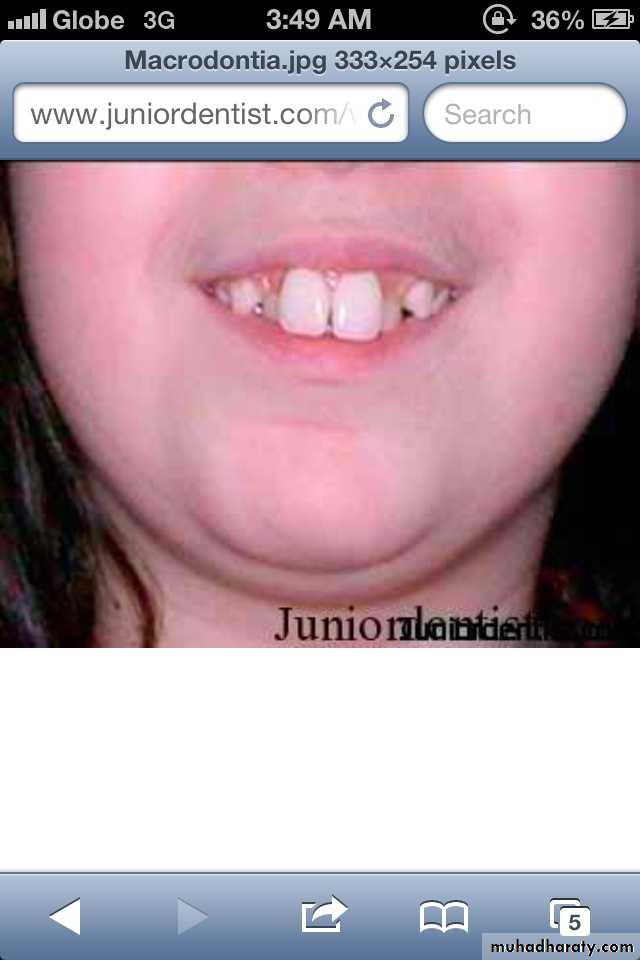
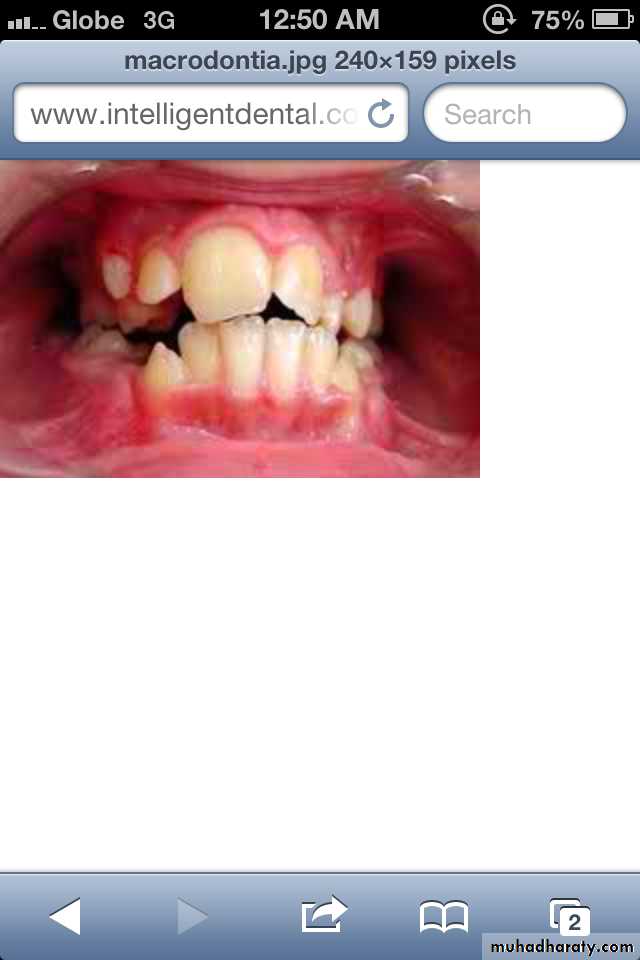
Macrodontia: the teeth are larger than normal, or the teeth are of normal size but occur in smaller than normal jaws.
(1) True Generalized Macrodontia
(2) Relative Generalized Macrodontia
(3) Focal or Localized Macrodontia
all teeth are larger than normal.
associated with pituitary giantism.exceedingly rare.
(1) True Generalized Macrodontia:

Normal or slightly larger than normal teeth in small jaws results in:
crowding of teethmalocclusion
impaction may occur.
(2) Relative Generalized Macrodontia
(3) Focal/Localized Macrodontiauncommon condition.
unknown etiology.
ERUPTION OF TEETH
Transposition:Transposition is the condition in which two teeth have exchanged positions.
Frequently transposed teeth are the permanent canine and first premolar.
Second premolars infrequently lie between first and second molars.
The transposition of central and lateral incisors is rare.
ALTERED MORPHOLOGY OF TEETH
Fusion:Fusion of teeth results from the combining of adjacent tooth germs,
resulting in union of the developing teeth.
OR fusion results when two tooth germs develop so close together
that as they grow, they contact and fuse before calcification.
OR a physical force or pressure generated during development
causes contact of adjacent tooth buds.
Appears as a single large tooth structure which may involve entire length of teeth, or may involve roots only, where the cementum &dentin are shared.


MANAGEMENT: It depends on which teeth are involved, the degree of fusion,and the morphologic result
*they may be retained as they are in deciduous teeth.
*In permenant teeth, the fused crowns may be reshaped with a restoration that mimics two independent crowns.
*Endodontic therapy may be necessary and perhaps may
be difficult or impossible if the root canals are of unusual
shape.
*In some cases it is most prudent to leave the teeth as they are.
Concrescence

*It occurs when the roots of two or more teeth are
united by cementum.*It may involve either primary or secondary teeth.
CAUSES: is unknown, space restriction during
development, local trauma, excessive occlusal force,
or local infection after development.
* Maxillary molars are most frequently involved,
especially 3rd molar and a supernumerary tooth.
*Involved teeth may fail to erupt or may
erupt incompletely.
Often requires no treatment unless
union interferes with eruption;
then surgical removal may be warranted.
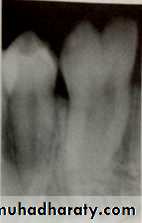
Concrescence of 7&8
Gemination (twining):

*Gemination is a rare anomaly that arises when the tooth bud of a single tooth attempts to divide.
The result may be an invagination of the crown, with
partial division, or in rare cases complete division
throughout the crown and root, producing identical
structures. Complete twinning results in a normal tooth
plus a supernumerary tooth in the arch.
CAUSE: is unknown, or it may be familial.
*The patient has a larger tooth but a normal number of teeth overall, in contrast to fusion, where the patient would appear to be missing one tooth.
MANAGEMENT : Affected teeth can cause malocclusion and lead to periodontal disease.
the affected tooth may be removed (if it is deciduous).the crown(s) may be restored or reshaped.
OR the tooth may be left untreated and periodically examined to preclude the development of complications.



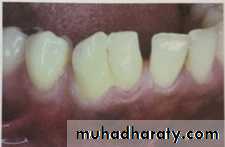
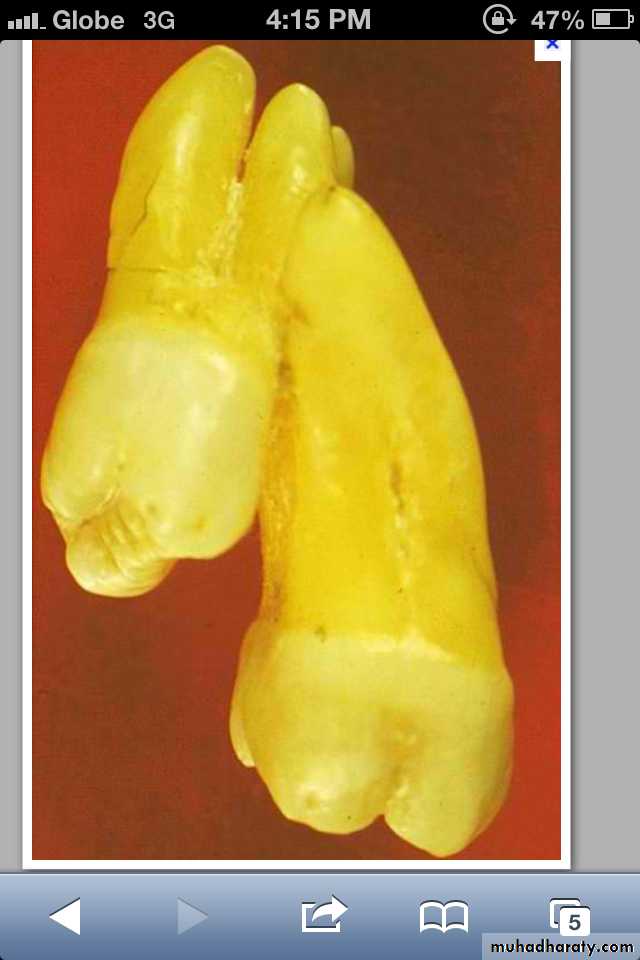
• Fusion of the left mandibular central and lateral incisors (twoindividual roots, two root canals and two joined crowns).
Gemination of right mandibular central incisor has one root, one root canal and a partially bifid dental crown.
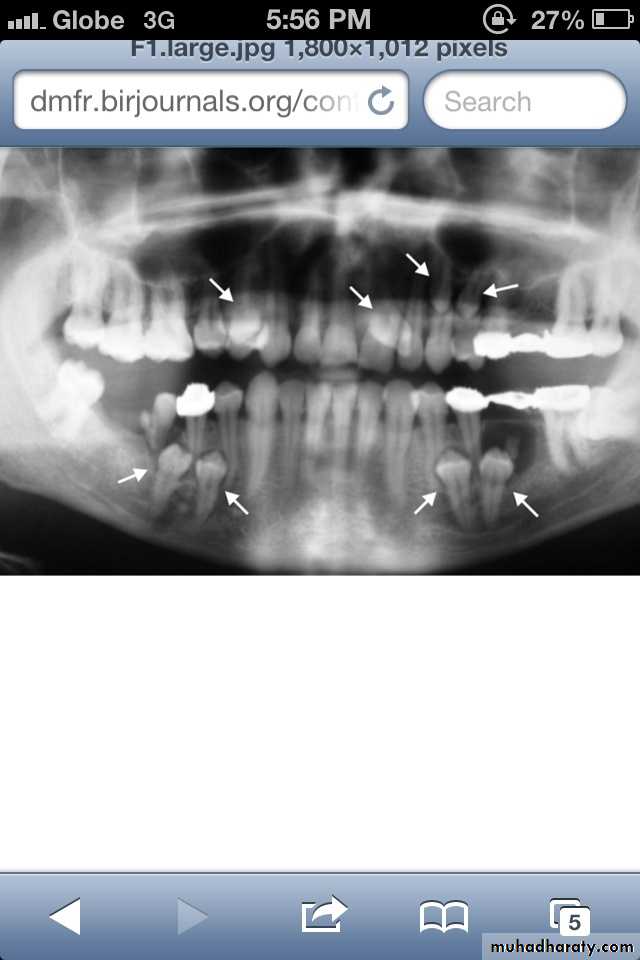
*Taurodont teeth have longitudinally enlarged pulp chambers.
*The crown is of normal shape and size, but the body is elongated and the roots are short.*The pulp chamber extends from a normal position in the crown throughout the length of the extended body, leading to an increased distance between the CEJ and the furcation.
Taurodontism



It may be associated with : Oral-facial-digital Syndrome.
Amelogenesis Imperfecta-Type IV,Down Syndrome.No treatment is required.
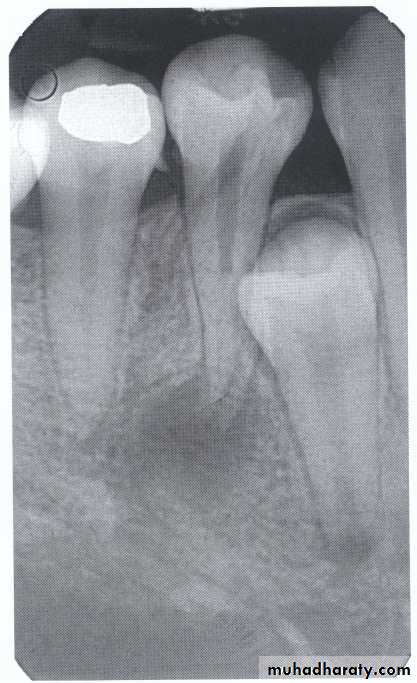
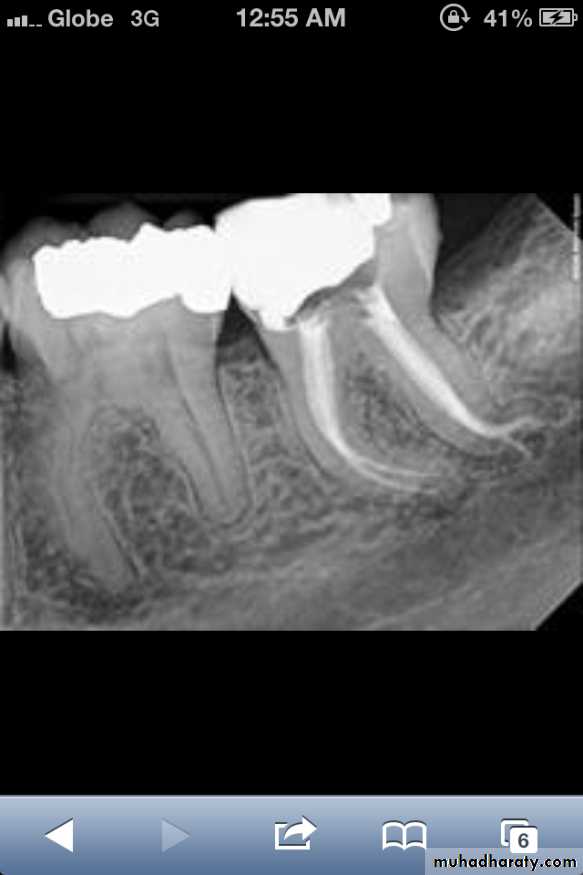
Dilaceration
*Dilaceration is a disturbance in tooth formation that produces a sharp bend or curve in the tooth (root or crown).
*CAUSES: trauma to the calcified portion of a partially formed tooth, or due to true developmental anomaly.
*Treatment:
No treatment. However, teeth with dilacerated roots
make extractions more complex.
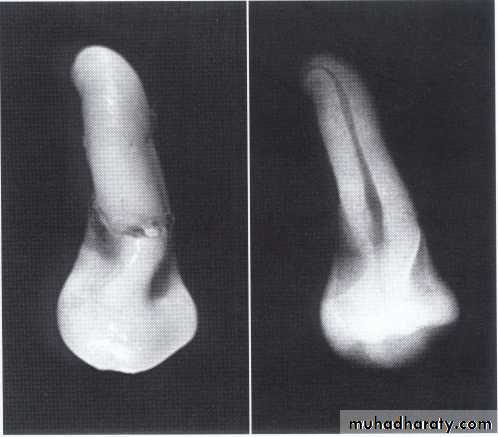
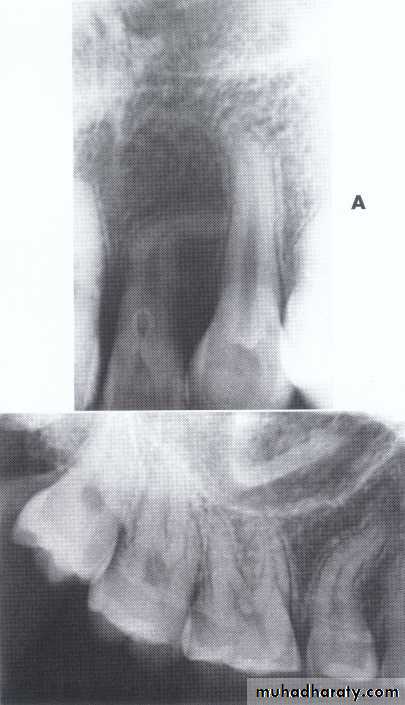
Dilaceration of the crown
specimenX-Ray
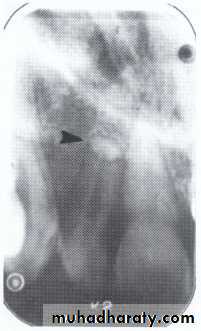
Dilacerated root. The apical portion of the root is bent buccally or lingually into the plane of the central ray. Note the halo in the apical region, produced by the PDL
space (arrow).
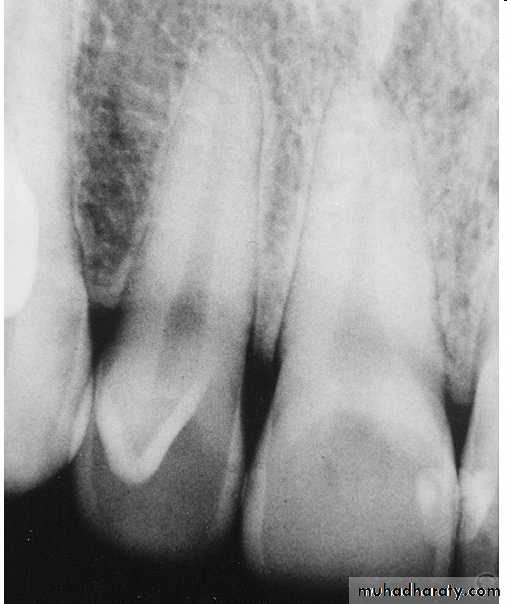
Dens in Dente (invaginated odontome) :
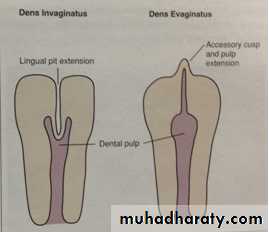
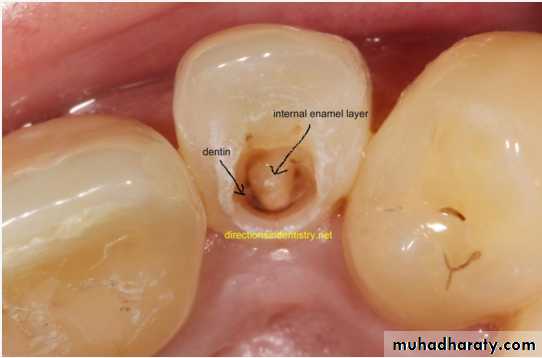
*It is an infolding of the outer surface of a tooth into the interior usually in the cingulum pit region of maxillary lateral incisors (tooth within a tooth).
*It is of 2 forms:coronal& radicular.
*Clinicaly varies from slight enlargement of cingulum
to a deep infolding that extends to the apex.
It has been classified into 3 major types:
*Type I:it is confined within the crown of the tooth and does not extend beyond the level of the external CEJ. *Type II :extends below CEJ ends in a blind sac, may or may not communicate with adjacent dental pulp. *Type III:extends through the root and communicates laterally with the periodontal ligament space through a pseudo-foramen or at the apical foramen . There is usually no communication with the pulp, which lies compressed within the root.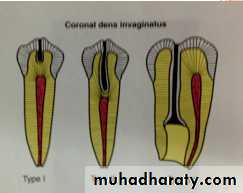
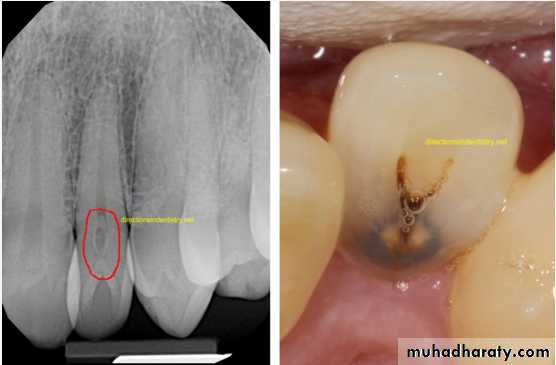

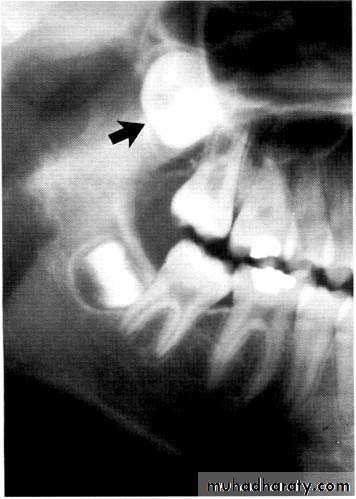
*Most cases of dens in dente are discovered radiographically. It is more radiopaque than the surrounding tooth structure and can easily be identified.
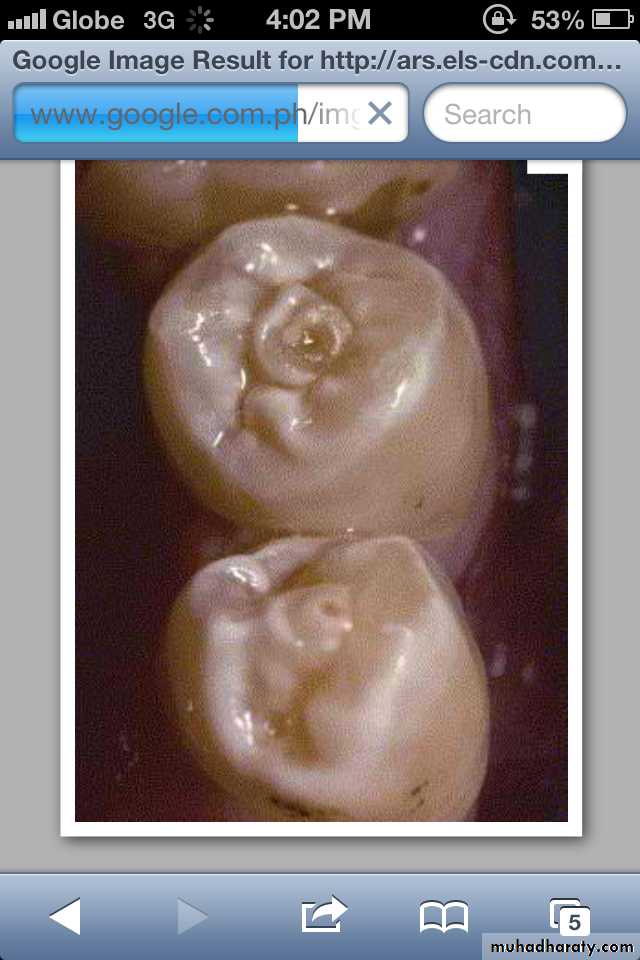
*In contrast to the dens in dente, Dens Evaginatus is the result of an outfolding of the enamel organ, involving an extra cusp or tubercle that protrudes from the tooth.
*Premolars are more likely to be affected than any other tooth.
*Located on occlusal surface between buccal & lingual cusps of premolars.It may be unilateral or bilateral.
*CAUSE:is unknown, but is thought to be a result of genetics or a disruption of the tooth during formation.
*TREATMENT:This condition requires monitoring as the tooth can lose its blood and nerve supply as a result,and may need root canal treatment.
Dens Evaginatus ( Leong's premolar)