4th stage
SurgeryLec-
Dr.Samir alsaffar
28/2/2016
Stomach & DuodenumGross anatomy of stomach
Microscopic anatomy :
The gastric epithelial cells are mucus producing and turned over rapidlyIn the pyloric part , mucus secreting glands are found
Parietal cells : Present in the body”acid-secreting” of stomach , Responsible for acid secretion
Chief cells : Pepsinogen
Endocrine cells :G cells; in the gastric antrum---gastrin
Enterochromaffin-like (ECL) cells ---Histamine
D cells ---somatostatin
Microscopic anatomy of Duodenum :
Lined by mucus secreting columner epithe
Brunner’s glandsEndocrine cells----cholecystokinin secretin
Physiology :
Storage “reservoir”Mechanical break up of ingested food
Production of chyme by the actions of acid and pepsin
Programmed passage of contents into duodenum
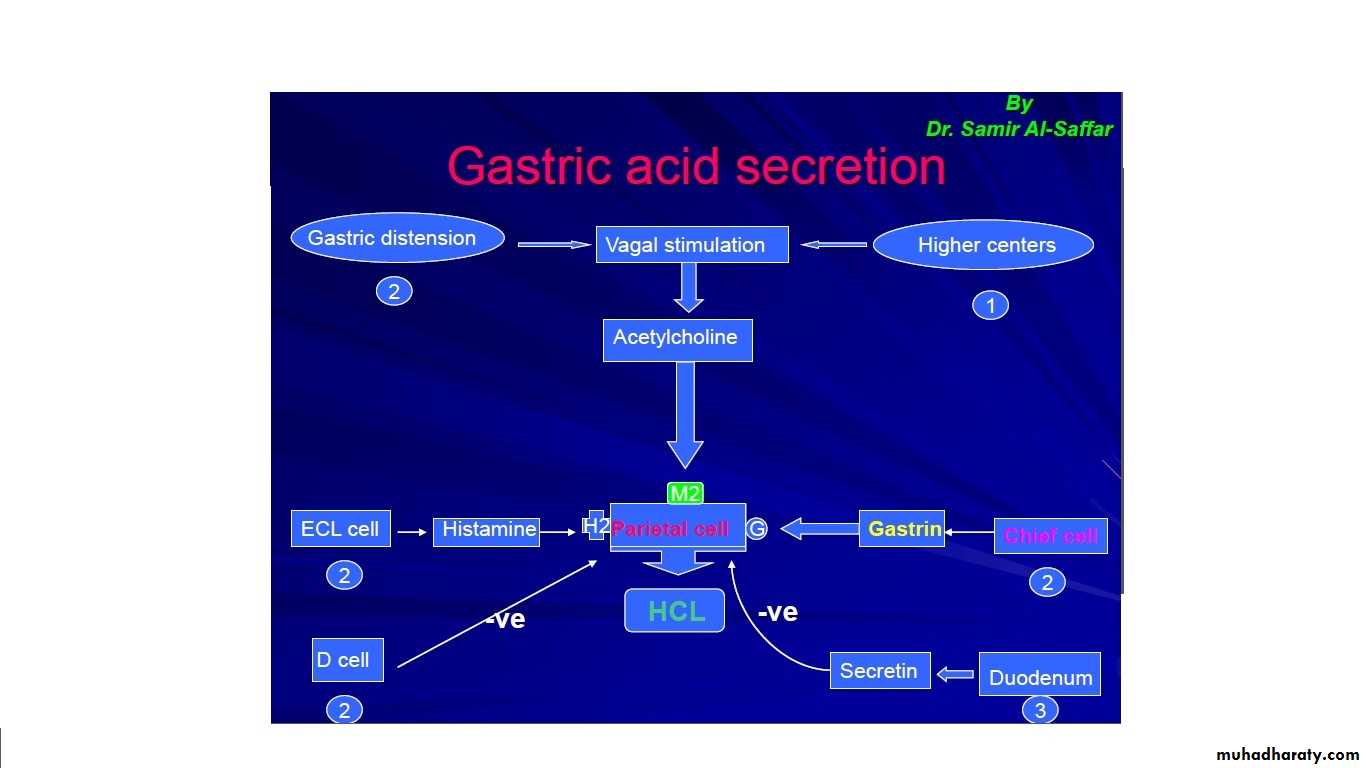
Gastric acid secretion :
Investigation of stomach and duodenum :
Flexible Endoscopy:Is more sensitive than conventional radiology in the assessment of the majority of GD conditions, e.g. peptic ulceration, gastritis, and duodenitis.
Upper GIT bleeding
Early gastric cancer
Diagnostic:
Visual
Biopsy
Endoluminal Ultrasound
Therapeutic:
Control of bleeding, inj. Laser, diathermyEndoscopic gastro-cystostomy
Endoscopic Gastrostomy
Removal of Foreign bodies
Disadvantages:
Invasive, discomfortPerforation, of pharynx, oesophagus
Miss-diagnosis,early gastric cancer.
Contrast radiology
Less commonly asked forOf value in;
Hiatus Hernia specially of the rolling type
Volvulous of stomach
Linitus plastica
Ultrasonography
Conventional US
Detection of large gastric tumor
Metastases to liver
Endoluminal US
Depth of wall invasion” T staging”
Local LN
Liver metastases
Laparoscopic US
CT scan and MRI
CT scanIn Gastric malignancy
Miss smaller lesions
Less accurate in T staging
Less easy to detect small liver metastases
MRI
Higher sensitivity for detection of gastric cancer liver metastases
Laparoscopy
Well used for assessment of patients with gastric cancerParticularly for detection of peritoneal seedlings
Other investigations
Gastric emptying studies
Angiography
Measurement of gastric acid secretion
Gastric motility
Plasma gastrin
Paediatric Disorders :
Hypertrophic pyloric stenosis of infancy
Aetiology:3:1000 births
4:1 male to female
Familial
Pathology:
Hypertrophy of musculature of pylorus and adjacent antum
Clinical features :
Commonly present at 4 wks of ageVomiting of milk without bile---2-3 days become forcible and projectile
Immediately after vomiting, the baby is usually hungery
Wt loss---emaciation, dehydration
Diagnosis
Test feed
Imaging:
Ultrasonography Olive mass
Contrast radiology no longer necessary
Differential Diagnosis
Gastro-oesophageal refluxFeeding problems
UTI
Raised intracranial pressure
Treatment
Correction of dehydration and electrolyte abnormalites; by using Dextrose saline plus potassiumFollowed by Operation “ Ramstedt’s”
Duodenal Atresia
Occur at the point of fusion between the foregut and midgut, in the neighbourhood of the ampulla of Vater.Other defects
Antenata Dx : US
The child vomits from birth and the vomitus is bile stained
Differential DX. : High intestinal obstruction , Pyloric stenosis
Treatment : Duodenoduodenostomy
Helicobacter PyloriProved its importance in the aetiology of ch.gastritis, peptic ulceration,and cancer
Waren and Marshal in 1980 proved casual relation between HP and Gastritis
HP is spiral shaped, able to hydrolyse urea to ammonia “a strong alkali”
Spread Feco-oral
Incidence 80 –90 %
Pathogensis
Antral gastritis---relase of ammonia---decrease in acidity---G cell stimulation--increase gastrin----increase in HCLDisruption of gastric mucosa through a number of cytotoxins
Diagnosis of HP infection
Brith testCLO
Histological examination of biopsy
Serological tests
Treatment
Eradication therapy :
Combination of antibiotics like : Metronidazol + Amoxil or Claithromycin + Amoxil
With the use of proton pump inhibitor like : Omerprazol, Lansoprazol