


Laryngeal masses
Benign lesionsBenign tumors
Malignant tumors
Benign laryngeal lesions
Vocal cord nodulesPolyp
Renkie’s edema
Granuloma
Anatomy of the true vocal cord
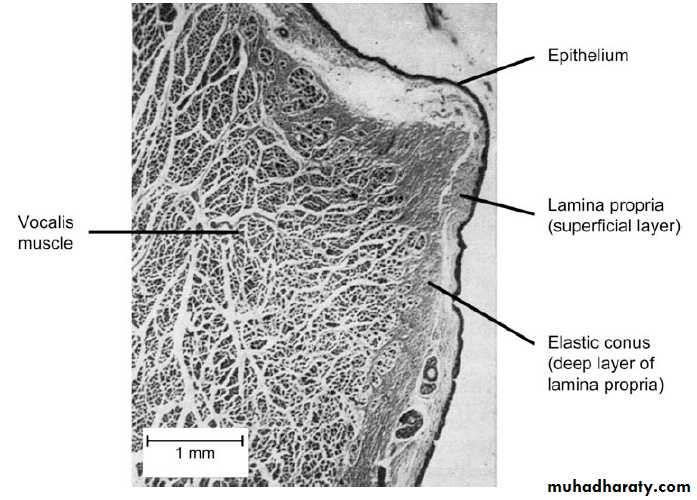
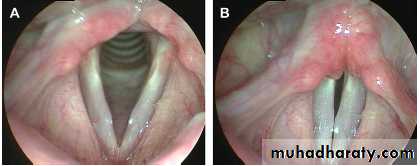
Vocal cord nodules(singer’s nodules)
Bilateral, symmetrical situated at the junction of anterior third with the posterior 2 thirds of the true vocal cords.Aetiology: voice abuse or misuse
More prevalent in children, teachers, lawyers, singers, house wife and other habitual voice users.
Treatment: voice rest
speech therapy
Microsurgery in longstanding cases after failure of conservative treatment.


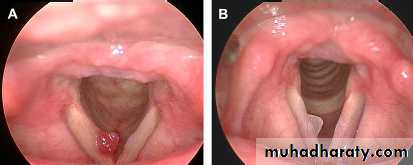
Vocal cord polyp
UnilateralBroad-based or pedunculated
Hemorrhagic or non-hemorrhagic
Caused by localized collection of fluid in Renkei’s
space.
Aetiology:
Voice abuse
Smoking
Gastroesophageal reflux
Treatment:
Microsurgery
Laser ( Co2 or pulsed dye )
Renkie’s edema
Bilateral diffuse involvement of true vocal cords.Subepithelial collection of fluid in Renkie’s space.
In addition to hoarseness might cause dyspnea and stridor if large and obstructing the airway.
Treatment:
Microsurgery
Laser

Granuloma
Specific: TB granulomaNon-specific: intubation granuloma (due to rough traumatic endotracheal intubation)
Affects the posterior part (arytenoid) of the vocal cord.
Unilateral.
Treatment:
Microsurgery
Laser
Intralesional steroid injection (for small granulomas)

Benign Tumors of the Larynx
Papilloma: 85%Chondroma
Hemangioma
Schwannoma
Neurofibroma
Adenoma
Fibroma,lipoma and leiomyoma
Papilloma: 2 types
a- Juvenile: usually multiple, recurrent after treatment but might regress after pubertyb- Adult: single lesion and no spontaneous regression
HPV type 6 and 11 play role in juvenile type , less consistently in adult type, presentation usually hoarseness, dyspnea and stridor
Treatment:
Microsurgical exicision
Co2 laser .
Antiviral agents: cidofovir or Interferones
Every effort should be made to avoid tracheotomy.

Malignant laryngeal tumors
Squamous cell ca is the commonest(more than 90%), adenocarcinoma, sarcoma, lymphoma...etcSCC of the larynx is the most common head and neck cancer with high cure rate reaching 90%.
Incidence:
Male more thane female 5:1
Elderly , 7th decade
Aetiology:
1- tobacco
2- alcohol
3- asbestose
4- radiation
5- premalignant conditions
Pathology:
Site:
Glottic 75%
Supraglottic 20%
Subglottic 5%
Histopathology:
The vast majority SCC with different grades of differetiation( poor, moderate or well differentiated)
Risk Factors
Etiology
The incidence of laryngeal tumors is closely correlated with smoking, as head and neck tumors occur 6 times more often among cigarette smokers than among nonsmokers.The age-standardized risk of mortality from laryngeal cancer appears to have a linear relationship with increasing cigarette consumption.
Risk Factors<<<
Although alcohol is a less potent carcinogen than tobacco, alcohol consumption is a risk factor for laryngeal tumors.In individuals who use both tobacco and alcohol, these risk factors appear to be synergistic, and they result in a multiplicative increase in the risk of developing laryngeal cancer.
Anatomy
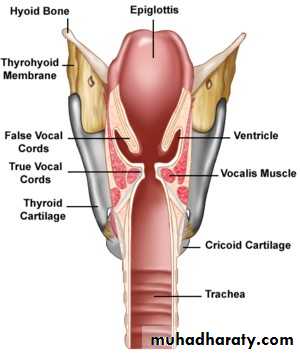
The supraglottic larynx
It consists of epiglottis, false vocal cords, ventricles, aryepiglottic folds, and arytenoids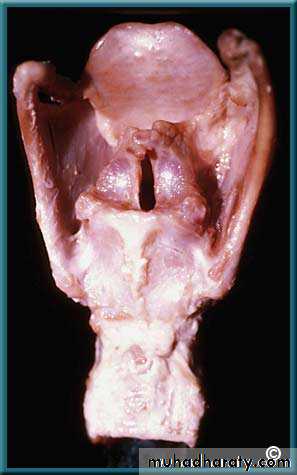
The glottic larynx
It consists of the true vocal cords and anterior commissure and posterior commissure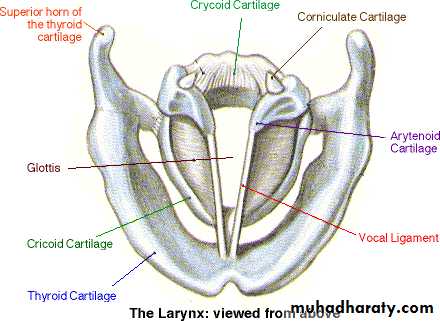
The subglottic larynx
It consists of the region between the vocal cords and the trachea.
Spread
Direct spread: vertical and circumferential, inside the larynx and to the nearby organsLymph node spread: to the pre-tracheal, paratracheal and deep cervical LNs. more common in the supraglottic and subglottic tumors. Pure glottic tumors rarely metastasize because practically there is no lymphatic drainage in the glottic region.
Distant: only 5 % at the time of presentation have distant metastasis.
Clinical features:
1- progressive unremitting dysphonia or hoarseness, early symptom in glottic t.2- pain : more prominent in supraglottic t.
3- dyspnea and stridor: in advanced tumors and could be the first presentation of subglottic t.
4- dysphagia: due to invasion of pharynx or esophagus
5- cervical lymphadenopathy: neck mass
6- cough and hemoptysis
7- anorexia and cachexia: late features
On examination: by a mirror or flexible endoscopy might shows the presence of a mass or ulcerative lesion . The vocal cords mobility should be assessed.
True vocal cord immobility in Ca larynx: causes
1- Nerve palsy (recurrent laryngeal nerve)
2- Vocal cord muscle involvement
3- Laryngeal joints involvement
4- Mass effect of the tumor
Investigations
. Assessment of general condition and fitness. Diagnosis of the disease
. Determination of the extent and stage
1- hematological : CBP, ESR
2- biochemical profile: renal and liver function tests, serum electrolytes and blood sugar3- radiological : CXR, CTS and MRI
4- ECG
5- Endoscopic exam. Of the larynx, pharynx, bronchial tree and esophagus and biopsy from any suspicious lesion.
TNM classification of glottic tumors
T1: Tumor limited to the vocal cord with normal mobilityT2: Tumor extension to the supraglottis and/or subglottis and/or impaired vocal cord mobility
T3: Tumor limited to the larynx with vocal cord fixation
T4: Tumor invasion through the thyroid cartilage and/or other tissues beyond the larynx .
Staging- Nodes
• N0
• No cervical lymph nodes positive
• N1
• Single ipsilateral lymph node ≤ 3cm
• N2a
• Single ipsilateral node > 3cm and ≤6cm
• N2b
• Multiple ipsilateral lymph nodes, each ≤ 6cm
• N2c
• Bilateral or contralateral lymph nodes, each ≤6cm
• N3
• Single or multiple lymph nodes > 6cm
M = metastasis
M0 : no distant metastasisM1 : distant metastasis is present
Staging
Stage 1: T1N0M0
Stage 2: T2N0M0
Stage 3: T3N0M0
Or T1N1M0
Or T2N1M0
Or T3N1M0
Stage 4: anything else
Treatment
1- Early tumours :( stage 1 and 2)
Best treated by radiotherapy (with or without chemotherapy) , external beam or interstitial radiation with preservation of the larynx.Cure rate : 85-90%
The alternatives to radiotherapy are:
1- partial laryngectomy as cordectomy or epiglottectomy
2- laser therapy: applicable for small marginal tumours and Carcinoma in situ.
Complications of radiotherapy:
1- oral mucositis2- skin complications: necrosis, depigmentation, hair loss
3- perichondritis
4- laryngeal oedema
5- general side effects: malaise, anorexia
6- late: induction of other malignancies as osteosarcoma
2- advanced tumours( stage 3 and 4):
The best is radical surgery in the form of total laryngectomy with or without partial pharyngectomy if the pharynx is involved, or neck dissection for lymph node metastasis. Post-operative radiotherapy might be given for extenssive tumours to erradicate microscopic metastasis.3- palliative treatment : indicated when there is
. Distant metastasis. Inoperable primary tumour
. Poor general health (unfit for surgery )
Includes:
1- pain relief
2- tracheostomy for airway obstruction
3- radiotherapy and chemotherapy.
