
Diabetes Mellitus
Part 2
Dr: Hussein Mohammed Jumaah
CABM
Lecturer in internal medicine
Mosul Medical College
2016
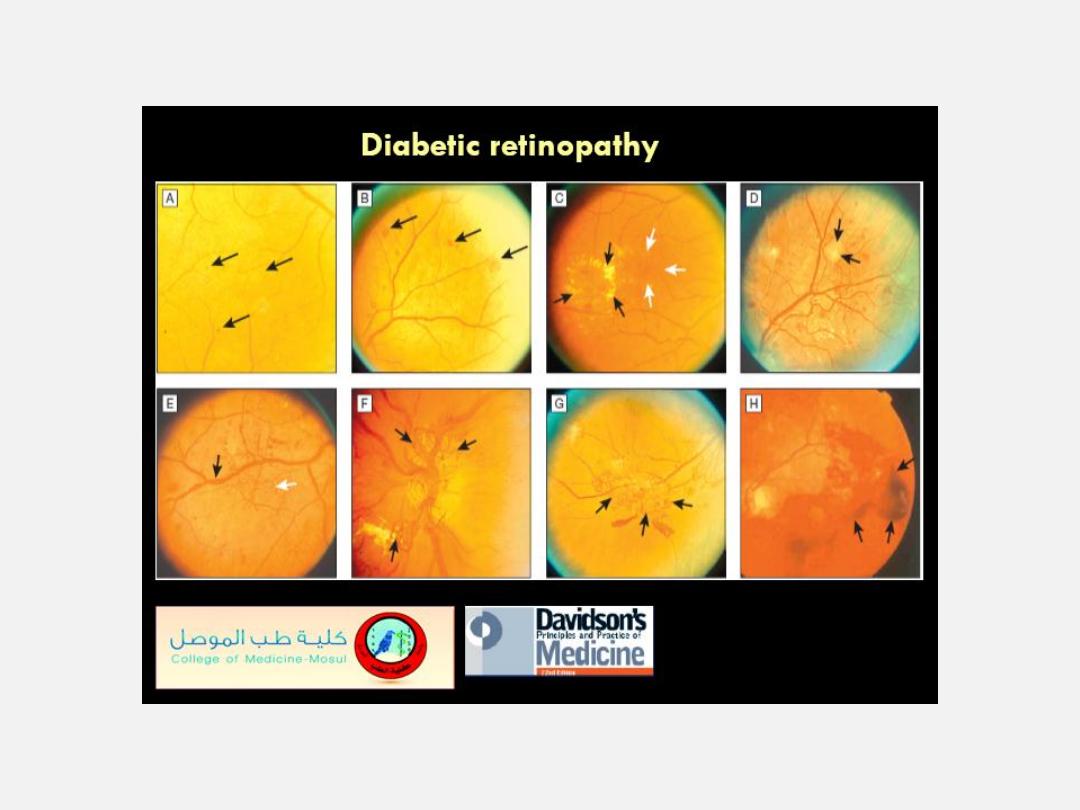
Diabetic retinopathy.
A
Microaneurysms. Usually the earliest clinical abnormality, these tiny
aneurysms arise mainly from the venous end of capillaries and appear as discrete, circular,
dark red dots.
B
Haemorrhages. Larger than a microaneurysm, with indistinct margins occur in
deeper layers of the retina (arrows). They result either from microaneurysms that have burst
or from leaky capillaries. Superficial flame-shaped haemorrhages in the nerve fibre layer
may also occur, particularly if the patient is hypertensive.
C
Hard exudates. These irregularly
shaped lesions are formed from leaking of cholesterol (black arrows). They can be
associated with retinal oedema; if this affects the centre of the macula, it can cause clinically
significant macular oedema (CSMO, white arrows), which is sight-threatening.
D
Cotton wool spots. These white, feathery, fluffy lesions indicate capillary infarcts within the
nerve fibre layer (arrows). They are most often seen in rapidly advancing
retinopathy or in association with uncontrolled hypertension.
E
Venous beading. In extensive
retinal ischaemia, walls of veins develop saccular bulges, (black arrow).
F
and
G
Neovascularisation. New vessel formation in response to widespread retinal ischaemia may
arise from the venous circulation either on the optic disc arrows in F) or elsewhere in the
retina (arrows in G)..
H
Vitreous haemorrhage. New vessels are fragile and liable to rupture
during vitreous movement, causing a pre-retinal (‘subhyaloid’) or a vitreous haemorrhage
(arrows), which may lead to sudden visual loss.
Monday , 7 March, 2016