1
DISEASES OF THE SMALL INTESTINE
Abdullah Alyouzbaki
Lecturer of Medicine/Mosul Medical College
Gastroenterologist and hepatologist
20/12/2015
Lec1
Disorders causing malabsorption:
Coeliac disease
is an inflammatory disorder of the small bowel
occurring in genetically susceptible individuals, which results from
intolerance to wheat gluten and similar proteins found in rye, barley
and, to a lesser extent, oats.
o
The condition occurs worldwide but is more common in northern
Europe.
o
The prevalence is approximately 1%,
o
50% of these people are asymptomatic.
o
‘silent’ coeliac disease ‘latent’ coeliac disease – genetically
susceptible people who may later develop clinical coeliac disease.
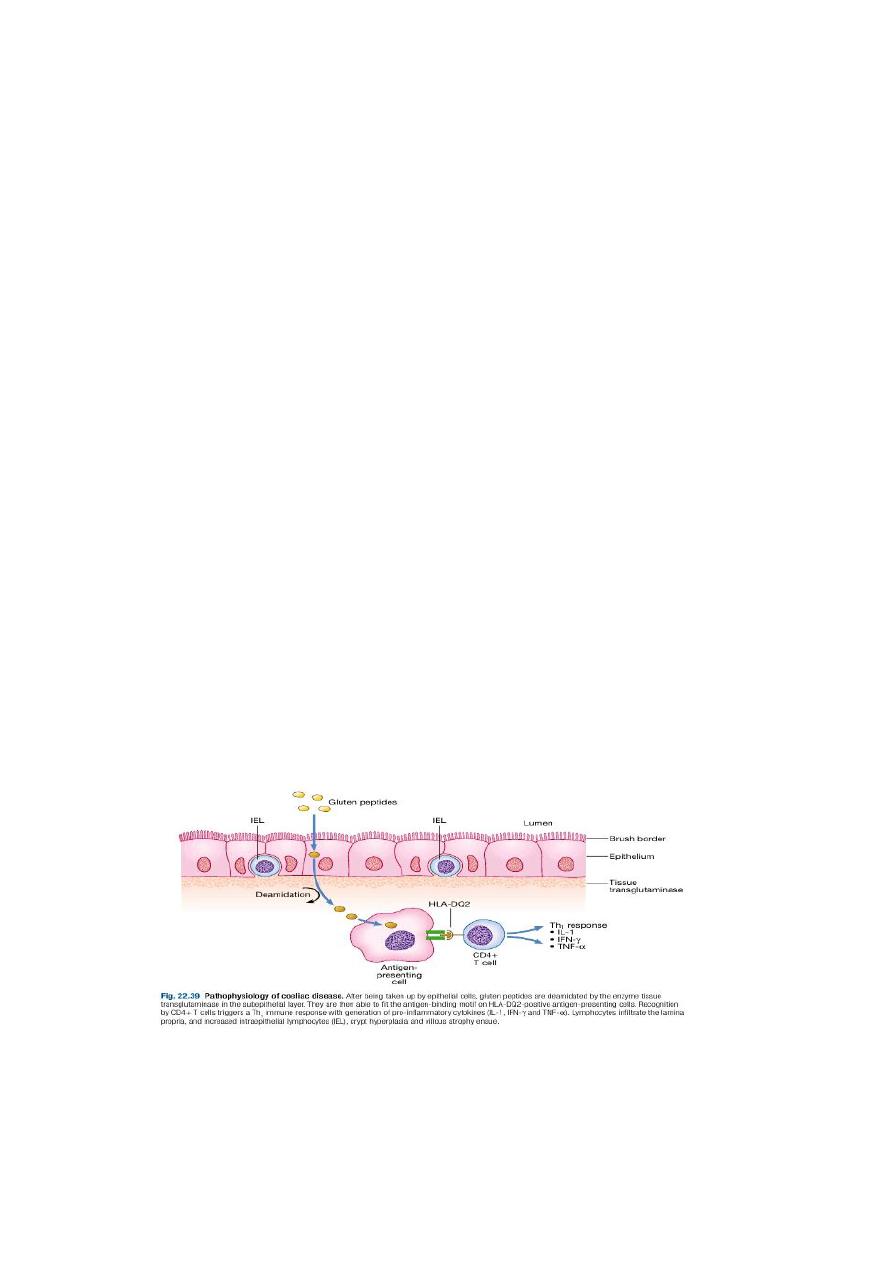
Pathophysiology

2
Presentation
Celiac disease can present at any age.
In infancy, it occurs after weaning on to cereals .
•
typically presents with diarrhea, malabsorption and failure to
thrive.
older children
o
:non-specific features such as delayed growth. Features of
malnutrition are found on examination and mild abdominal
distension.
o
pubertal delay
,
leading to short stature in adulthood.
In adults:
•
usually during the third or fourth decade
•
females > males.
•
The presentation is highly variable: florid malabsorption,
while others develop non-specific symptoms, such as
tiredness, weight loss, folate deficiency or iron deficiency
anaemia. oral ulceration, dyspepsia and bloating. mild
under-nutrition and osteoporosis.

3
Investigations
1)Duodenal biopsy: Endoscopic small bowel biopsy is the gold
standard. The histological features are usually characteristic but
other causes of villous atrophy should be considered.

4
2)Antibodies:
o
Anti tissue transglutamase antibodies and Anti-endomysial
antibodies of the IgA :They are sensitive (85–95%) and specific
(approximately 99%) for the diagnosis, except in very young
infants.
o
IgG antibodies, however, must be analysed in patients with coexisting
IgA deficiency.
o
they usually become negative with successful treatment.
3)Haematology and biochemistry:
•
A full blood count may show microcytic or macrocytic anaemia
from iron or folate deficiency and features of hyposplenism (target
cells, spherocytes and Howell– Jolly bodies).
•
Biochemical tests may reveal reduced concentrations of calcium,
magnesium, total protein, albumin or vitamin D.

5
Management
•
Exclusion of wheat, rye, barley and initially oats, although oats
may be re-introduced safely in most patients after 6–12 months.
•
Frequent dietary counselling.
•
Mineral and vitamin supplements.
•
Measurement of tTG or anti-endomysial antibodies.
Complications
•
Risk of malignancy, particularly of enteropathy-associated T-cell
lymphoma, small bowel carcinoma and squamous carcinoma of the
esophagus.
•
Ulcerative jejuno-ileitis.
•
Osteoporosis and osteomalacia.
Coeliac disease : still diarrhea in spite of gluten free diet??
•
Non Compliance , Non Compliance ,…..Non compliance.
•
Associations : pancreatic insufficiency , microscopic colitis,
inflammatory bowel disease.
•
Complications: ulcerative jejunitis , enteropathy associated T-cell
lymphoma, small bowel carcinoma and refractory coeliac disease.

6
Dermatitis herpetiformis
•
intensely itchy blisters over the elbows, knees, back and
buttocks.
•
Immunofluorescence shows granular or linear IgA deposition
at the dermoepidermal junction.
•
Almost all patients have partial villous atrophy on duodenal
biopsy, identical to that seen in coeliac disease, even though
they usually have no gastrointestinal symptoms.
•
The rash usually responds to a gluten free diet but some
patients require additional treatment with dapsone.
7
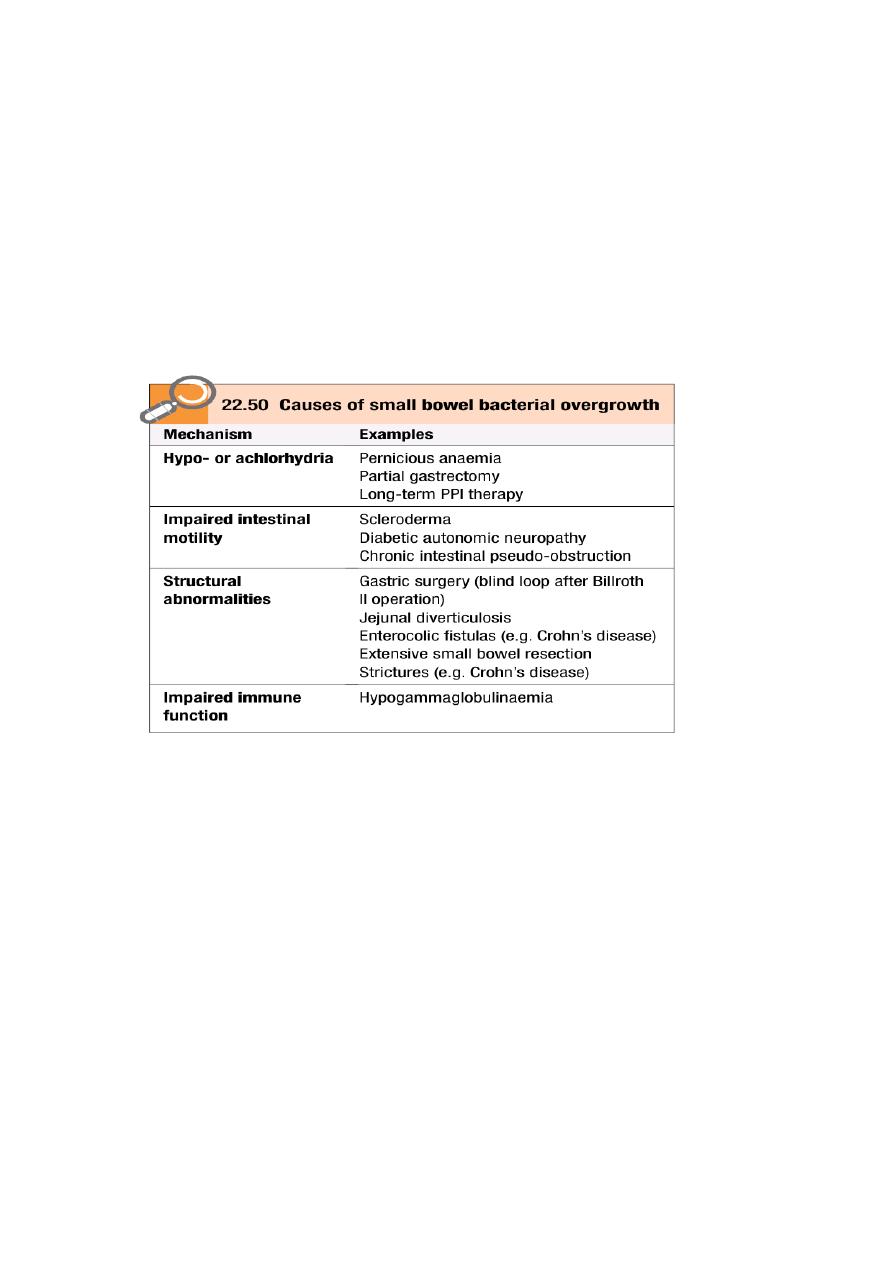
Small bowel bacterial overgrowth
(‘blind loop syndrome’)
•
The normal duodenum and jejunum contain fewer than
10⁴/mL. organisms, which are usually derived from saliva.
•
The count of coliform organisms never exceeds10⁴/mL .
•
In bacterial overgrowth, there may be 10
8
–10
10
/mL
organisms, most of which are normally found only in the colon.
Clinical features
The patient presents with watery diarrhoea and/or steatorrhoea, with
anaemia due to B12 deficiency. These arise because of deconjugation of
bile acids, which impairs micelle formation, and because of bacterial
utilisation of vitamin B12.

8
Investigations
•
Barium follow-through .
•
Jejunal contents for bacteriological examination can also be aspirated
at endoscopy (Gold standard) .
•
non-invasively using hydrogen breath tests.
•
Low serum levels of vitamin B12, with normal or elevated
folate levels because the bacteria produce folic acid.
Management
•
Treatment of the underlying cause of small bowel bacterial
overgrowth
•
Tetracycline (250 mg 4 times daily for 7 days) is then the
•
treatment of choice, Metronidazole (400 mg 3 times
daily) or ciprofloxacin (250 mg twice daily) is an alternative.
•
Some patients require up to 4 weeks of treatment and, in a few,
continuous rotating courses of antibiotics are necessary.
•
Intramuscular vitamin B12 supplementation.
9
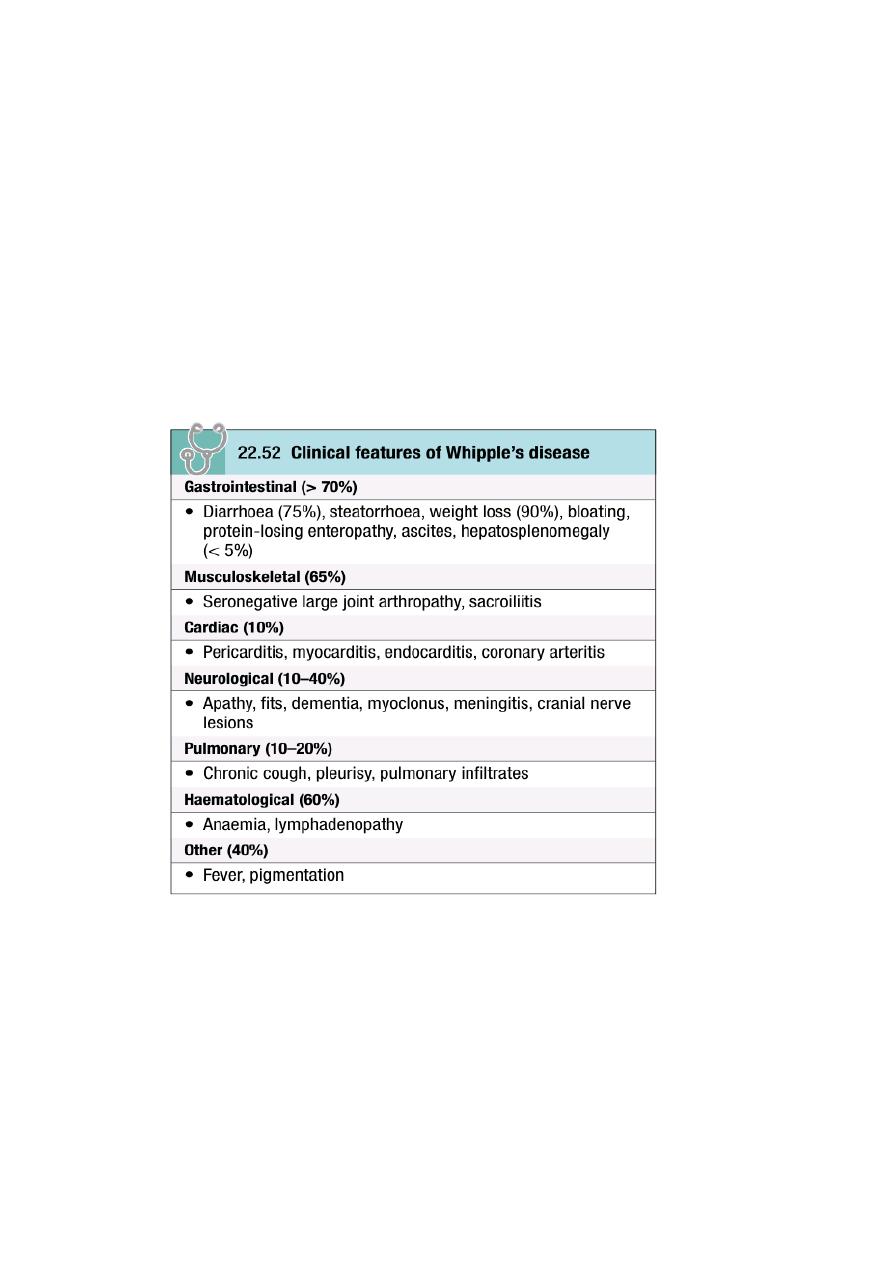
Whipple’s disease
•
This rare condition is characterised by infiltration of small intestinal
mucosa by ‘foamy’ macrophages, which stain positive with periodic
acid–Schiff (PAS) reagent.
•
Caused by infection with the Gram positive bacillus Tropheryma
whipplei.
•
The disease is a multisystem .
11
Diagnosis
:
•
characteristic features on small bowel biopsy, with characterisation of
the bacillus by polymerase chain reaction (PCR).
Management:
•
often fatal if untreated .
•
Responds well, at least initially, to intravenous ceftriaxone
(2g daily for 2 weeks), followed by oral co-trimoxazole for
at least 1 year.
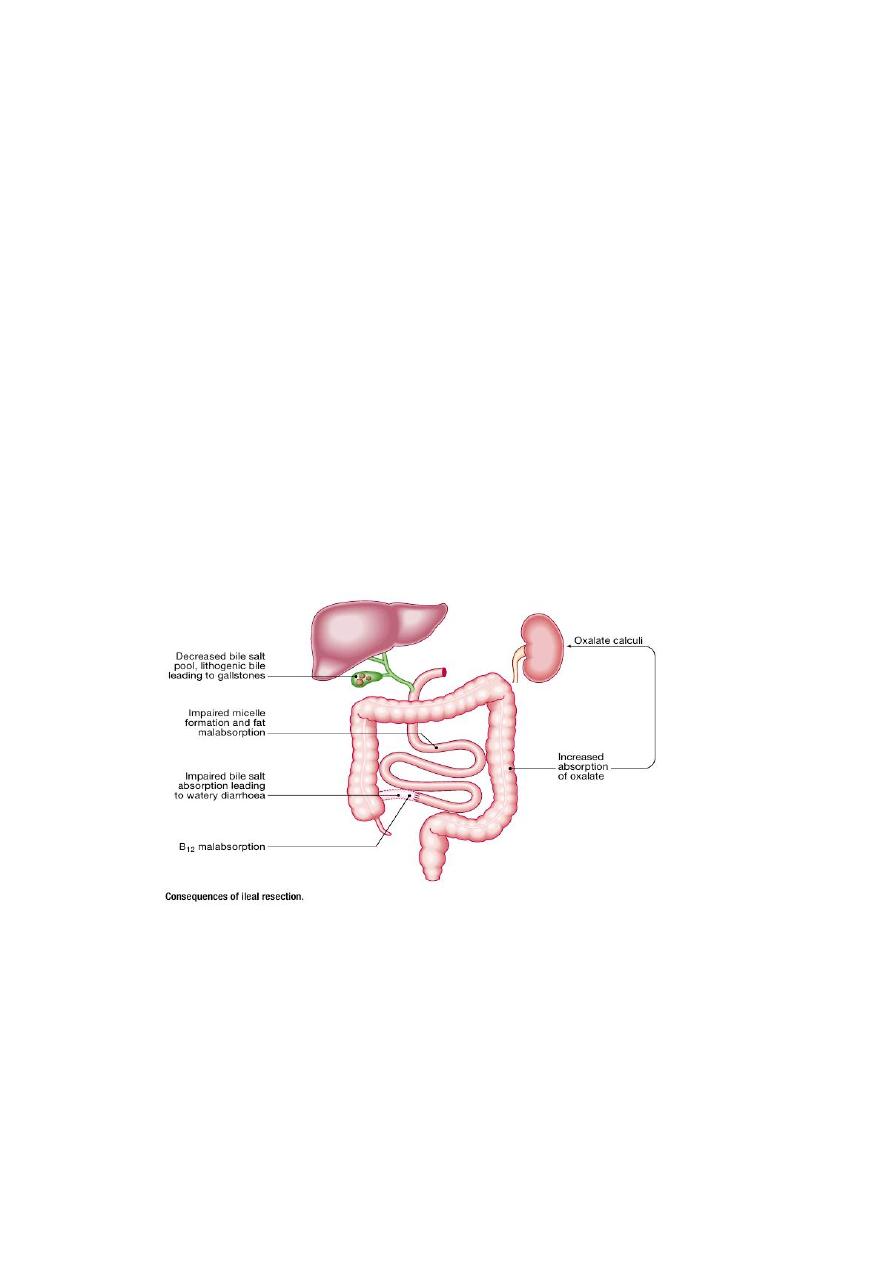
Ileal resection
•
The most common scenario is in patients with Crohn’s disease.
•
Diarrhea usually responds well to colestyramine, a resin which
binds bile salts in the intestinal lumen. Aluminium hydroxide can be
used as an alternative
.

11
Short bowel syndrome
•
Digestion and absorption are
normally completed within the
first 100 cm of jejunum, and
enteral feeding is usually still
possible if this amount of small
intestine remains.
•
The presence of some or all of
the colon can markedly
improve these losses by
increased water reabsorption.
•
The presence of an intact
ileocaecal valve ameliorates the clinical picture by slowing small
intestinal transit and reducing bacterialovergrowth.
Clinical features
•
Diarrhoea and steatorrhoea.
•
Dehydration and signs of hypovolaemia are common,
•
weight loss, loss of muscle bulk and malnutrition.

12
Management
•
In the immediate post-operative period: total parenteral nutrition
(TPN) should be started and PPI therapy given to reduce gastric
secretions.
•
Enteral feeding should be cautiously introduced after 1–2 weeks under
careful supervision and slowly increased as tolerated.
•
If less than 75 cm of small bowel remains, TPN is also needed.
•
Detailed nutritional assessments at regular intervals
•
Monitoring of fluid and electrolyte balance.
•
Adequate calorie and protein intake, Fats are a good energy source and
should be taken as tolerated. Medium-chain triglyceride are given
because they are more easily absorbed.
• Replacement of vitamin B12, calcium, vitamin D, magnesium, zinc and
folic acid.
•
Loperamide (2–4 mg 4 times daily) or codeine phosphate (30 mg 4–6
times daily) for diarrhoea.
•
Octreotide (50–200 μg 2–3 times daily by subcutaneous injection)
reduces gastrointestinal secretions.
•
some require long-term home TPN for survival .
•
Small bowel transplantation.

13
Radiation enteritis and proctocolitis
•
The risk varies with total dose, dosing schedule and the use of
concomitant chemotherapy.
•
Acute injury: nausea, vomiting , abdominal pain and diarrhea . When
the rectum and colon are involved, rectal mucus, bleeding and
tenesmus occur. rectal changes at sigmoidoscopy resemble ulcerative
proctitis or ulcerative colitis. Barium follow-through showing small
bowel strictures, ulcers and fistulae.
•
Chronic Phase
:Proctocolitis , Bleeding from telangiectasia, Small
bowel strictures, Fistulae: rectovaginal , colovesical , enterocolic ;
Adhesions, Malabsorption: bacterial overgrowth, bile salt
malabsorption(ileal damage).
Management
•
Diarrhoea : codeine phosphate, diphenoxylate or loperamide.
•
Local corticosteroid enemas can help proctitis.
•
Antibiotics may be required for bacterial overgrowth.
•
Nutritional supplements.
•
Colestyramine (4 g as a single sachet) is useful for bile salt
malabsorption.
•
Endoscopic argon plasma coagulation therapy may reduce bleeding
from proctitis.
•
Surgery should be avoided, if possible, because the injured intestine is
difficult to resect and anastomose, but may be necessary for
obstruction, perforation or fistula.

14
ISCHAEMIC GUT INJURY
•
Ischaemic gut injury is usually the result of arterial occlusion.
•
Severe hypotension and venous insufficiency are less frequent
causes.
•
The presentation is variable, depending on the different vessels
involved and the acuteness of the event.
•
Diagnosis is often difficult.

15
Acute small bowel ischaemia
•
An embolus from the heart or aorta to the superior mesenteric artery
is responsible for 40–50% of cases, thrombosis of underlying
atheromatous disease for approximately 25%, and non-o myocardial
infarction, heart failure, arrhythmias or sudden blood loss for
approximately 25%. Vasculitis and venous occlu cclusive ischaemia
due to hypotension complicating sion are rare causes.
•
The clinical spectrum ranges from transient alteration of bowel
function to transmural haemorrhagic necrosis and gangrene. Almost
all develop
•
abdominal pain that is more impressive than the physical findings.
•
In the early stages, the only physical signs may be a silent, distended
abdomen or diminished bowel sounds, peritonitis only developing
later.
•
Leucocytosis, metabolic acidosis, hyperphosphataemia and
hyperamylasaemia are typical.
•
Plain abdominal X-rays show ‘thumb-printing’ due to mucosal
oedema.
•
Mesenteric or CT angiography reveals an occluded or narrowed
major artery with spasm of arterial arcades, although most patients
undergo laparotomy on the basis of a clinical diagnosis without
angiography.
•
Resuscitation, management of cardiac disease and intravenous
antibiotic therapy, followed by laparotomy, are key steps.
•
If treatment is instituted early, embolectomy and vascular
reconstruction may salvage some small bowel.
•
In these rare cases, a ‘second look’ laparotomy should be undertaken
24 hours later and further necrotic bowel resected.
•
In patients at high surgical risk, thrombolysis may sometimes be
effective.

16
Chronic mesenteric ischaemia
•
This results from atherosclerotic stenosis of the coeliac axis,
superior mesenteric artery and inferior mesenteric artery. At least
two of the three vessels must be affected for symptoms to develop.
•
The typical presentation is with dull but severe mid- or upper
abdominal pain developing about 30 minutes after eating. Weight
loss is common because the patient is reluctant to eat, and some
experience diarrhoea.
•
Physical examination shows evidence of generalised arterial disease.
•
An abdominal bruit is sometimes audible but is non-specific.
•
The diagnosis is made by mesenteric angiography.
•
Treatment is by vascular reconstruction or percutaneous
angioplasty, if the patient’s clinical condition permits.
The condition is frequently complicated by intestinal infarction, if
left untreated.

17