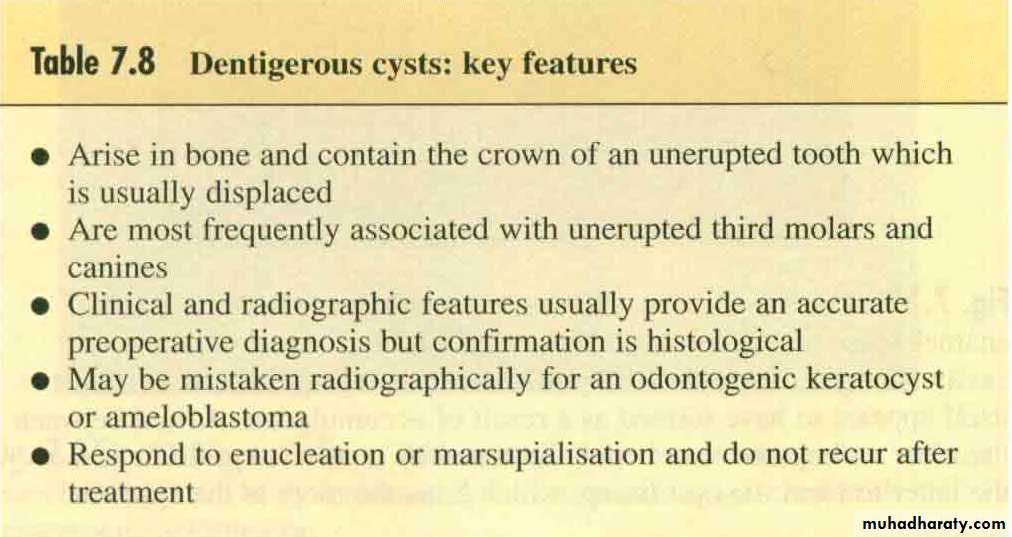
Dentigerous cyst
clinical features
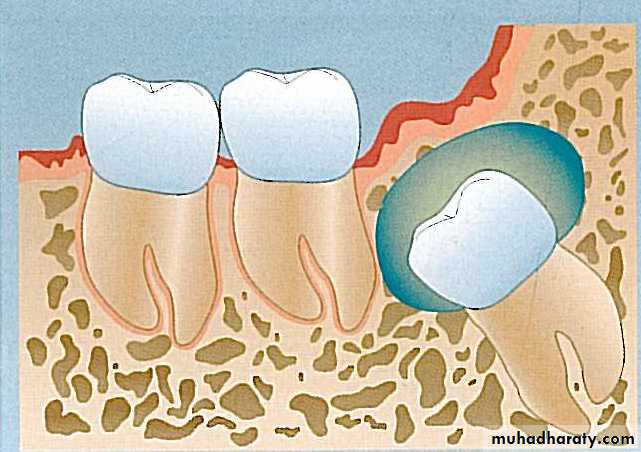
DC contain the crown of an un-erupted tooth ( mostly 3rd molar and canine) and have epithelium lining derived from enamel epithelium, attached to the tooth at the cementoenamel junction. Prevent the tooth from eruptionTwice common in male than female.
Uncommon in children and often found between the ages of 20 – 50.
clinical features
It may be a chance radiographic finding or found when the cause is sought for missing tooth.Infection of DC cause the usual symptoms of pain and accelerated swelling.
radiographical features
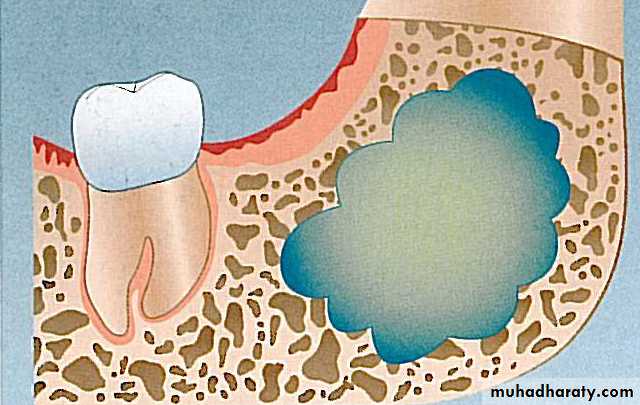
The cavity well circumscribed, rounded and unilocular and contain the crown of a tooth displaced from normal position.
The slow growth of DC result in a seclerotic bony outline and well defined cortex.
Some times shoe pseudo- loculation due to bone trabeculation
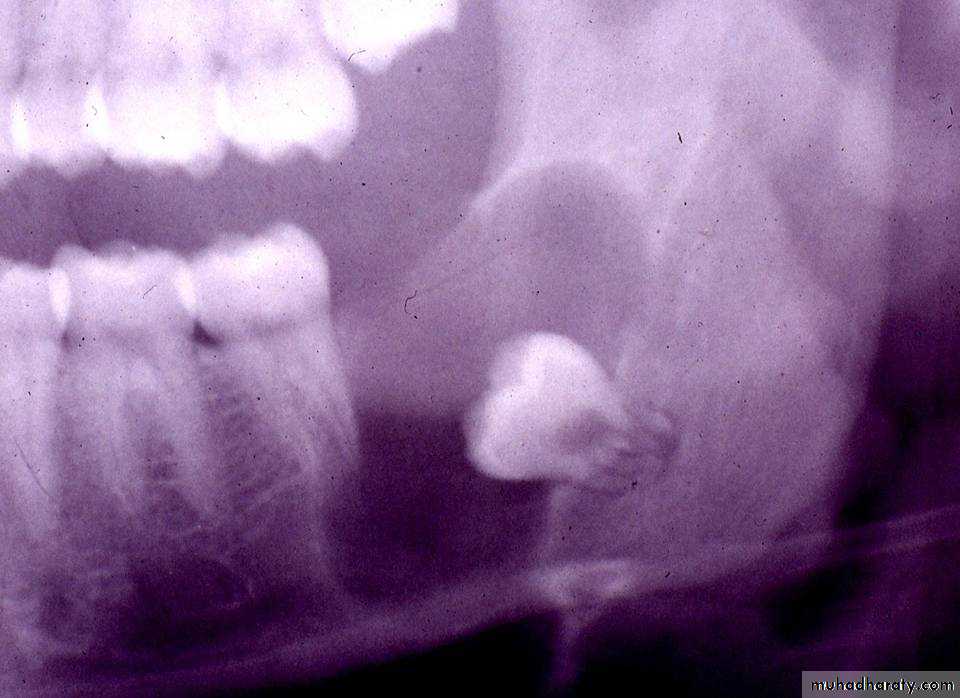
• The affected tooth is often displaced to considerable distance and the lower third molar may be pushed to the lower border of the mandible.
* If the cyst remain un-recognised for long period the enclosed tooth may be resorbed.
jrPathogenesis
Odontogenic keratocyst
OKC uncommon but important because of their strong tendency to recur after treatment .Form posteriorly , most frequently in the posterior alveolar ridge and angle of the mandible.
Peak incidence between ages 20 – 30 years, other series bet. 50-70 years.
The mandible usually affected, 50% of OKC form in angle of the mandible, extending forwards in to the body and upwards in to the ramus.
Odontogenic keratocyst
OKC are symptoms less until the bone expand or become infected.
the expansion of the cyst is much less than radiographic extent
Frequently recur after enucleation,.
Do not respond to marsupialusation.
Definitive diagnosis is only by histopathological examination although clinical and radiographical features may allow fairly accurate diagnosis.
Odontogenic keratocyst
OKC may be confused radiographically with ameloblastoma or with Dentigerous cyst.Spread extensively through marrow space before expanding the jaw
May be part of the jaw cyst/ basal cell naevus syndrome.
radiographical features
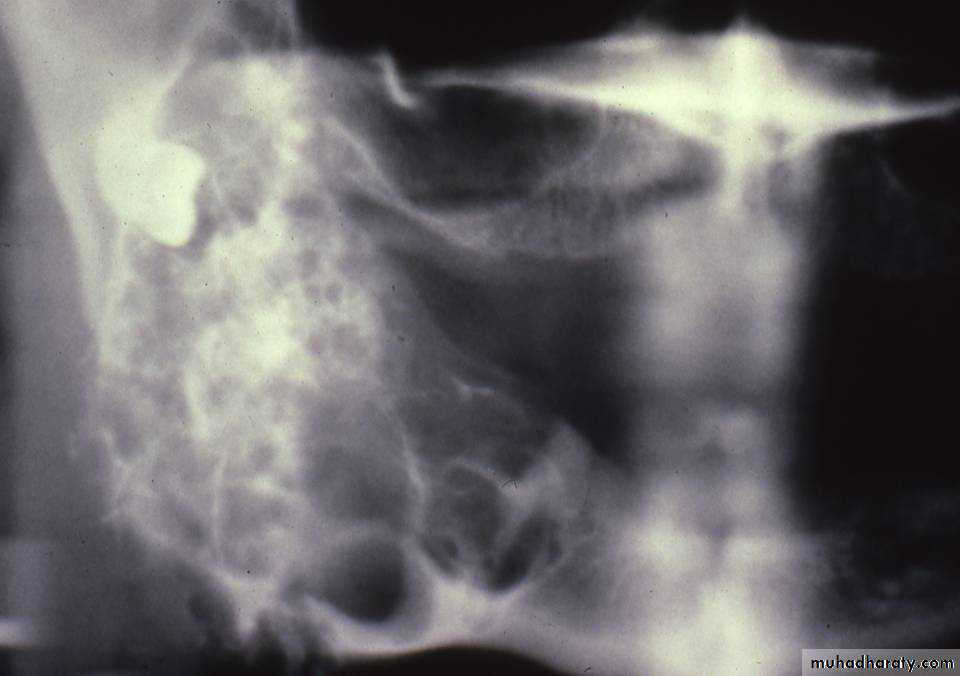
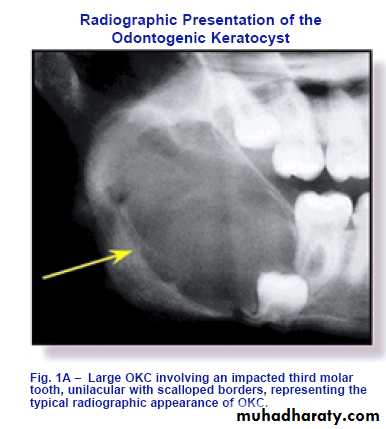
Appear as well defined radiolucent area more or less rounded with a scalloped margin, or multiloculated radiolucency resembling ameloblastoma.The bony wall appear sharply demarcated.
It may envelop an unerupted tooth and in this case it may be indistinguishable from dentigerous cyst.
Roots of the adjacent teeth may become displaced.
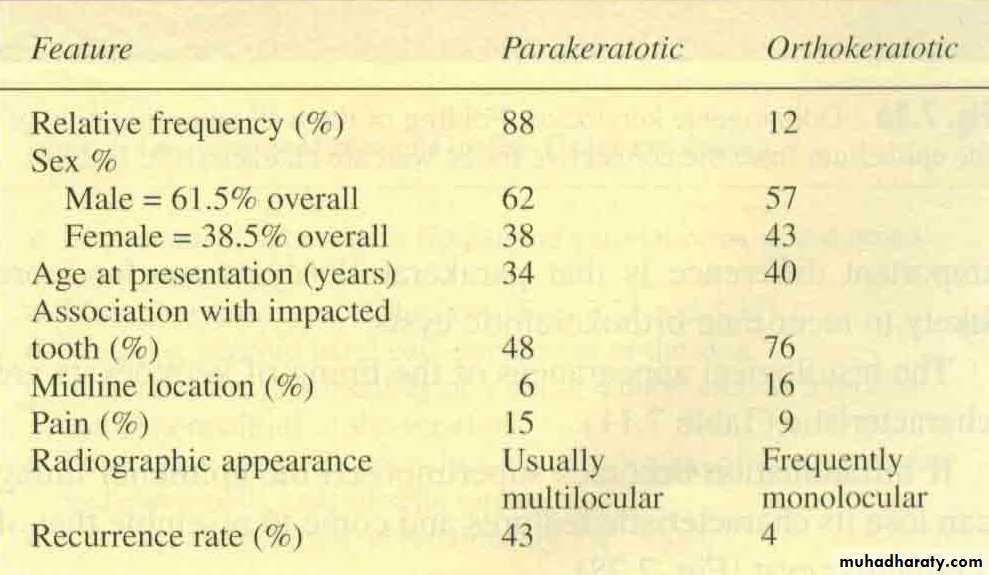
Two types of keratocyst are recognized, parakeratotoc and orthokeratotic . differences between them are as follow
Causes of recurrence of OKC
Thin, fragile lining, difficult to enucleate intact.Finger like extensions in to the cancellous bone.
Daughter cyst in the wall.
Rapid proliferation of the KC epithelium.
Other dental lamina remnant.
Gingival cyst
Dental lamina cyst of the newborn( Bohn's nodule).Up to 80% of newborn infants have small nodules or cyst in the gingiva due to proliferation of epithelial rest of serres.
Resolve spontaneously.

cyst ( Epstein pearl ) may arise from the non odontogenic epithelium along the midpalatal raphe, may enlarge sufficiently to appear as creamy- colourd swelling a few millimeters in diameter, but also resolve spontaneously in a matter of months.

Gingival cyst of adults
Exceedingly rare.Usually form after the age of approximately 40 years.
They form dome shape swelling less than 1 cm in diameter and some time erode the underlying bone.
They are lined by very thin, flat stratified sequamous epithelium.
May contain fluid or layers of keratin.
Unlikely to recur after enucleation.


Nasopalatine duct cyst
Which form in the midline of the anterior maxilla, un common.Nasopalaine, incisive canal, medianpalatine, median alveolar cysts are variants of the same lesion.
Slowly growing, occasionally they cause intermittent discharge with salty taste.
Large cyst may cause swelling in the midline of the anterior palate.
When it is superficial called palatine papilla cyst.
Nasopalatine duct cyst
Arise from the vestiges of the nasopalatine duct and may be lined by columnar respiratory epithelium.The long sphenopalatine nerve and vessels may be present in the wall.
Do not recur after treatment .
Can be recognized radiographically.
Nasopalatine duct cyst
Radiograph shows a rounded radiolucent area with well defined sclerotic margin in the anterior part of the midline of the maxilla.
They occasionally appear heart-shaped because of radiographic superimposition of the nasal spine.
They are usually symmetrical but may be larger to one side.
Incisive Canal Cyst

Nasolabial cyst
This very un common cyst form out side the bone in the soft tissues, deep to the nasolabial fold.It arise from the remnant of the nasolabial duct and occasionally bilateral.
Large cyst produce swelling of the upper lip and distort the nostril.
Treatment by simple excision.

Bone cystAneurysmal bone cyst
Rare in the jaws.Jaw lesions are frequently in the mandibular angle and ramus.
affected patients usually between 10 and 20 years.
Are of unknown etiology.
form very expansile soap bubbles radiolucencies which may be mistaken radiographically and clinically for ameloblastoma or odonto.keratocyst.
histologically consist of mass of blood-filled spaces which has been likened a blood filled sponge with scattered giant cells.
treatment consist of thorough curettage which may need to be repeated , as the lesion occasionally recurs.
Bone cystsimple(solitary, traumatic bone cyst)
Most often seen in teenagers and un common after age of 25.They form painless swelling or are chance radiographic findings.
The mandible is mainly affected.
Radiographically. Theses cysts form rounded, radiolucent areas which generally tend to be less sharply defined than odontogenic cysts.
They have 2 unusual features:
• The area of radiolucency much larger than the size of the swelling suggests.• The radiolucency arch up between the roots of the teeth.
Traumatic Bone Cyst
bone cystsimple(solitary, traumatic bone cyst
It is also known as hemorrhagic or traumatic bone cyst.The cystic cavity has a rough bony wall, thin connective lining, few red blood cells , blood pigment and few giant cells .
There is often no cystic contents but there may be some time little fluid.
Resolve after surgical opening and closure, or spontaneously .
Cyst of the soft tissues
Most of the soft tissues cysts are non odontogenic.
The most common soft tissue cyst are mucoceles ( extravasation and retention type) and the ranula which originate in the minor salivary glands, but the sublingual dermoid is developmental anomaly.
Sublingual dermiod
Form as a result of some abnormality of the development of the branchial arches or pharyngeal pouch.It develop between the hyoid bone and the mandible or may form immediately beneath the tongue.
Some time filled with desquamated keratin giving them a semi-solid consistency.
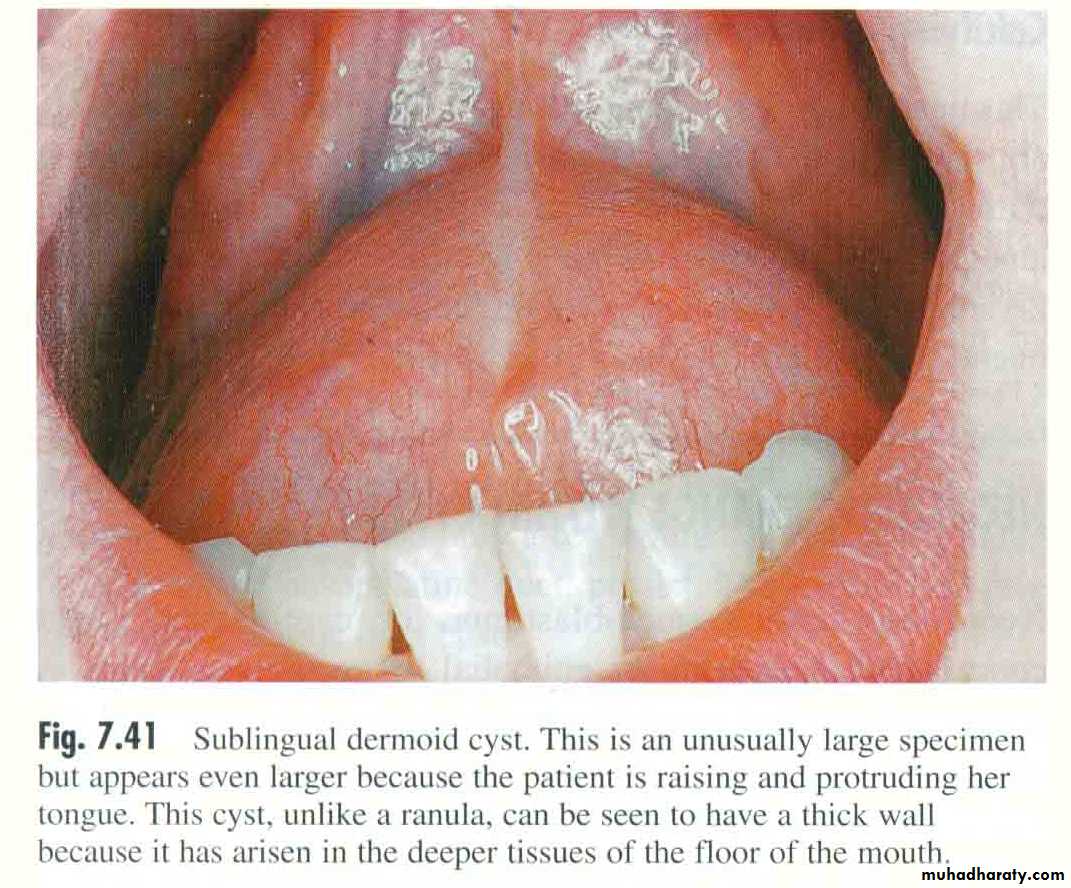
Sublingual dermiod
A dermoid cyst cause no symptoms until large enough to interfere with speech or eating.Large swelling can be accommodated in the floor of the mouth with out disability and can be concealed with the tongue in its resting position.
Treated by surgical excision.
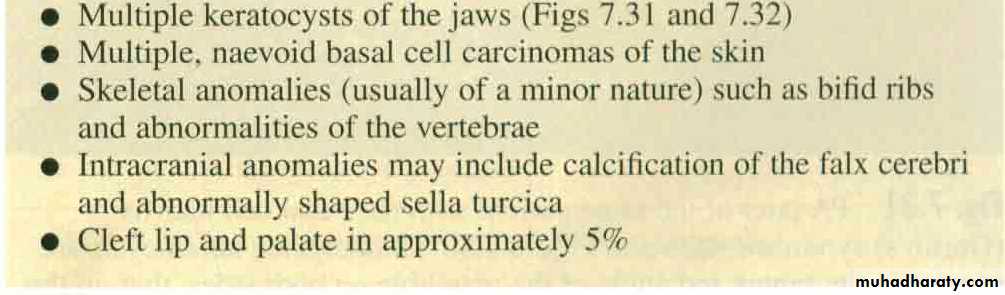
Gorlin –Goltz, basal cell carcinoma