PATHOLOGY OF THE BREAST
INFLAMMATIONSAcute mastitis: usually develop during the early weeks of nursing.
Mammary duct ectasia :nonbacterial chronic inflammation of the breast, inspissation of breast secretions in the main excretory ducts, ductal dilation with ductal rupture.
Traumatic fat necrosis
Galactocele is cystic dilatation of one or more ducts occurring during lactation.
FIBROCYSTIC CHANGE
the most common benign breast conditionproducing vague ‘lumpy’ breast.
incidence range from 10-20% in adult women
3rd and 5th decades of life
role of oestrogen in its pathogenesis
Features of fibrocystic disease
i) Cystic dilatation of terminal ducts.ii) Relative increase in inter- and intralobular fibrous tissue.
iii) Variable degree of epithelial proliferation in the terminal ducts.
two clinicopathological relevant groups
1-Nonproliferative Fibrocystic Changes.
2- Proliferative Fibrocystic Changes (epithelial hyperplasia)

EPITHELIAL HYPERPLASIA
increase in the layers of epithelial cells over the basement membrane to three or more layersIt could be in the ducts or in the lobule.
Ductal hyperplasia may show various grades of epithelial proliferations (mild, moderate and atypical),
lobular hyperplasia involving the ductules or acini is always atypical:



Types of hyperplasia
1. Mild ductal hyperplasia consists of at least three layers of cells above the basement membrane, focally or evenly throughout the duct.2. Moderate and florid hyperplasia is associated with tendency to fill the ductal lumen with proliferated epithelium. The proliferations into the lumina of ducts may be focal, forming papillary epithelial projections called ductal papillomatosis, or may be more extensive, termed florid papillomatosis, or may fill the ductal lumen leaving only small fenestrations in it.
Types of hyperplasia
3. Atypical ductal hyperplasia is more ominous ,the proliferated epithelial cells in the atypical ductal hyperplasia partially fill the duct lumen and produce irregular microglandular spaces or cribriform pattern.
4. Atypical lobular hyperplasia is closely related to lobular carcinoma in situ but differs from the latter in having cytologically atypical cells only in half of the ductules or acini
TUMORS OF THE BREAST
1-FIBROADENOMA2-PHYLLODES TUMOUR
3-INTRADUCTAL PAPILLOMA
4-CARCINOMA OF THE BREAST
1-FIBROADENOMA
Is a benign tumor of fibrous and epithelial elements.It is the most common benign tumor of the female breast.
Most patients between 15 to 30 years of age.
solitary, discrete, freely mobile nodule within the breast.
Grossly: small (2-4 cm diameter), solitary, well encapsulated, spherical or discoid mass.
Microscopy: Fibrous tissue comprises most of a fibroadenoma.
2-PHYLLODES TUMOUR (CYSTOSARCOMA PHYLLODES)
It is an uncommon bulky breast tumor.aggressive clinical behaviour.
Most patients are between 30 to 70 years of age.
Grossly: large, 10-15 cm in diameter, round to oval, bosselated, and less encapsulated than a fibroadenoma.
grey-white with cystic cavities, areas of haemorrhages, necrosis and degenerative changes.
Microscopy: extremely hypercellular stroma, accompanied by proliferation of benign ductal structures.
benign, borderline and malignant
Cellularity, frequency of mitoses; cellular atypia;; and infiltrative margins..
phyllodes tumour
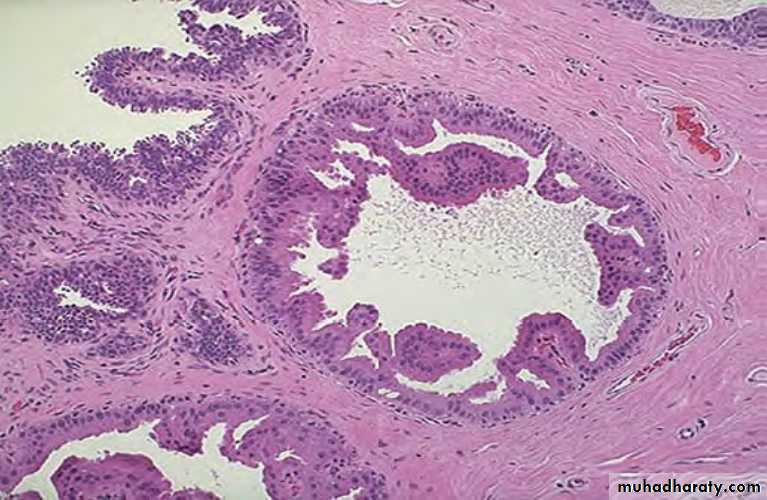
3-INTRADUCTAL PAPILLOMA
benign papillary tumor occurring in a lactiferous duct or lactiferous sinus near the nipple.Clinically, it produces serous or serosanguineous nipple discharge.
most common in 3rd and 4th decades of life.
Gross: usually solitary, small, less than 1 cm in diameter, commonly located in the major mammary ducts close to the nipple.
Microscopy: multiple papillae having well-developed fibrovascular stalks attached to the ductal wall and covered by benign cuboidal epithelial cells supported by myoepithelial cells.
4-CARCINOMA OF THE BREAST
1.Geography.2. Genetic factors. First-degree relatives of women with breast cancer have 2 to 6-fold higher risk of development of breast cancer.
ii) Genetic mutations: About 10% breast cancers have been found to have inherited mutations.
3. Estrogen excess. There is sufficient evidence to suggest that excess endogenous oestrogen or exogenously administered oestrogen for prolonged duration is an important factor in the development of breast cancer. Normal breast epithelium possesses oestrogen and progesterone receptors. The breast cancer cells secrete many growth factors which are oestrogendependent.
4. Miscellaneous factors. These include a host of following environmental influences and dietary factors associated with increased risk of breast cancer:
i) Consumption of large amounts of animal fats, high calorie foods.
ii) Cigarette smoking.
iii) Alcohol consumption.
iv) Breast augmentation surgery.
v) Exposure to ionising radiation during breast development.
5. Fibrocystic change. atypical epithelial hyperplasia, has about 5-fold higher risk of developing breast cancer subsequently.
Classification
NON-INVASIVE (IN SITU) BREAST CARCINOMA
Intraductal Carcinoma
Lobular Carcinoma in Situ
INVASIVE BREAST CARCINOMA
Infiltrating (Invasive) Duct Carcinoma
Infiltrating (Invasive) Lobular Carcinoma
Intraductal Carcinoma
initially begins with atypical hyperplasia of ductal epithelium followed by filling of the duct with tumor cells.Clinically, it produces a palpable mass in 30-75% of cases
Grossly : The tumor may vary from a small poorly-defined focus to 3-5 cm diameter mass.
cut section, the involved area shows cystically dilated ducts containing cheesy necrotic material (in comedo pattern), or the intraductal tumor may be polypoid and friable resembling intraductal papilloma (in papillary pattern).
Microscopy : The proliferating tumor cells within the ductal lumina may have 4 types
i) Solid pattern is characterised by filling and plugging of the ductal lumina with tumor cells.
ii) Comedo pattern is centrally placed necrotic debris surrounded by neoplastic cells in the duct.
iii) Papillary pattern has formation of intraductal papillary projections of tumor cells which lack a fibrovascular stalk so as to distinguish it from intraductal papilloma.
iv) Cribriform pattern is recognised by neat punched out fenestrations in the intraductal tumor.
Ductal carcinoma in situ
Lobular Carcinoma in Situ
It is not a palpable or grossly visible tumor.
The Patients of have a much higher incidence of developing a contralateral breast cancer (30%).
Grossly : No visible tumor is identified.
Microscopy: In situ lobular carcinoma is characterised by filling up of terminal ducts and ductules or acini by uniform cells which are loosely cohesive and have small, rounded nuclei with indistinct cytoplasmic margins.
Invasive Duct Carcinoma
Groosly: The tumor is irregular, 1-5 cm in diameter, hard mass that cuts with a grating sound.cut surface of the tumor is grey white to yellowish .
Microscopy: A variety of histologic features commonly present :
i) Anaplastic tumor cells forming solid nests, cords, poorly-formed glandular structures and some intraductal foci.
ii) Infiltration by these patterns of tumor cells into diffuse fibrous stroma and fat.
iii) Invasion into perivascular and perineural spaces as well as lymphatic and vascular invasion.
Infiltrating (Invasive) Lobular Carcinoma
comprises about 5% of all breast cancers.more frequently bilateral; and within the same breast,
have multicentric origin.
Grossly: The appearance varies from a well-defined mass to a poorly defined area of induration .
Microscopy:
i) Pattern—A characteristic single file (Indian file) linear arrangement of stromal infiltration by the tumor cells with very little tendency to gland formation is seen.Infiltrating cells may be arranged concentrically around ducts in a target-like pattern.
ii) Tumor cytology—Individual tumor cells resemble cells of in situ lobular carcinoma. They are round and regular with very little pleomorphism and infrequent mitoses.