Suprarenal gland:
The two adrenal glands, lie at the superior poles of the two kidneys, each gland is composed of two distinct parts, the adrenal medulla and the adrenal cortex.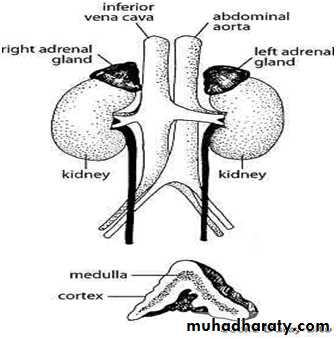
The adrenal medulla, the central part of the gland, is functionally related to the sympathetic nervous system; it secretes the hormones epinephrine and norepinephrine in response to sympathetic stimulation.
The adrenal cortex (the outer part) secretes an entirely different group of hormones, called corticosteroids. These hormones are:
1-Mineralocorticoids: they have gained this name because they especially affect the electrolytes (the “minerals”) of the extracellular fluids-sodium and potassium, in particular.
2-The glucocorticoids have gained their name because they exhibit important effects that increase blood glucose concentration.
Approximately 90 to 95 per cent of the cortisol in the plasma binds to plasma proteins
. About 2% is in the free form which is the active form .This high degree of binding to plasma proteins slows the elimination of cortisol from the plasma; therefore, cortisol has a relatively long half life (the bound cortisol act as a reservoir for the hormone )
3-Sex hormones.
Functions of the Glucocorticoids:
At least 95 per cent of the glucocorticoid activity of the adrenocortical secretions results from the secretion of cortisol,Cortisol:
The physiological action of cortisol:
1-Effects of Cortisol on Carbohydrate Metabolism:
It increases blood glucose concentration(antihypoglycemic effect) .
a-It stimulates gluconeogenesis (formation of carbohydrate from proteins and some other substances) by the liver, this effect is part of the effect on protein ,because it increases the enzymes required to convert amino acids into glucose in the liver cells.
As a result, more amino acids become available in the plasma to enter into the gluconeogenesis process of the liver and thereby to promote the formation of glucose.
The increase in glucose level will stimulate insulin secretion; also it reduces the sensitivity of many tissues, especially skeletal muscle and adipose tissue, to the stimulatory effects of insulin on glucose uptake and utilization. If this persists for long time it will cause B cell exhaustion →diabetes mellitus.
b- Decreased Glucose Utilization by Cells:
Cortisol causes a moderate decrease in the rate of glucose utilization by most cells in the body (skeletal , muscles and adipose tissue) ,by inhibiting glucose entry to the cells→ increase blood glucose concentration to be available for normal brain function ,so it protect the brain from hypoglycemia.2-Effect on protein metabolism:
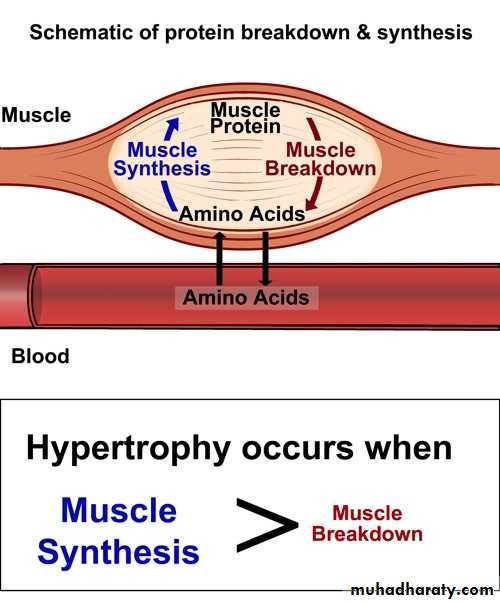
It exerts catabolic effect on protein. Because of decreased amino acid transport into extrahepatic tissues also depresses the formation of RNA and subsequent protein synthesis in many extrahepatic tissues, especially in muscle and lymphoid tissue.It diverts amino acids from the muscles and the liver for the process of deamination and gluconeogenesis, so it facilitates the breakdown of proteins.
3-Effects of Cortisol on Fat Metabolism:
It promotes mobilization of fatty acids from adipose tissue. This increases the concentration of free fatty acids in the plasma, which also increases their utilization for energy.4-Effect on minerals:
It has a similar effect to aldosterone, although it is weaker than it (1/10 the power of Aldosterone).
It promotes sodium retention and potassium elimination, but no edema because there is increase in the glomerular filtration rate (GFR).
5-Effect on respiration:
It is important for the synthesis of surfactant during intrauterine life (to prevent respiratory distress syndrome). In females who are about to deliver preterm babies we usually give them cortisol to promote the formation of surfactant)6-Effect on water balance:
It causes sodium retention which leads to water retention .It also causes increase in GFR (glomerular filtration rate), which counteract the water retention and the person does not develop edema.7-Effect on cardiovascular system:
Cortisol restores vascular reactivity. It helps in maintaining arterial response to sympathetic tone. Deficiency of the hormone leads to hypotensive subject due to failure to maintain the peripheral resistance. While patients with hyperfunction of the adrenal cortex are hypertensive(because of the increase in peripheral resistance).8-Effect on GIT:
Cortisol reduces the resistance of gastric mucosa to HCL so increase secretion of it leads to ulcer (so before giving the patient steroid tablets ask him if he has gastric pain or ulcer otherwise it may cause perforation to the stomach). Also it has an anti vitamin D effect .It prevent the absorption of the vitamin from the intestine.9-Effect on lymphoid tissue and heamopoiesis:
Cortisol suppresses the production of antibodies (used in chronic inflammatory diseases) in which inappropriate antibodies are produced in the subject against his own tissues (The administration of large doses of cortisol causes decreases the output of both T cells and antibodies from the lymphoid tissue. As a result, the level of immunity for almost all foreign invaders of the body is decreased).Conversely, this ability of cortisol and other glucocorticoids to suppress immunity makes them useful drugs in preventing immunological rejection of transplanted hearts, kidneys, and other tissues.
10-Effect on bones:
Excessive secretion leads to osteoporosis due to destruction of the matrix of the bone (catabolic effect of cortisol on protein found in the matrix). This effect of cortisol in mobilizing proteins could make amino acids available to needs of the cells to synthesize substances essential to life.
11-Anti- inflammatory effect of cortisol:
It has the following effects to prevent inflammation:1-Cortisol stabilizes the lysosomal membranes, so decreases the proteolytic enzymes that are released by the lysosomes.
2. Cortisol decreases the permeability of the capillaries. This prevents loss of plasma into the tissues.
3. Cortisol decreases both migration of white blood cells into the inflamed area and phagocytosis of the damaged cells.
4. Cortisol suppresses the immune system, causing lymphocyte reproduction to decrease markedly(especially T lymphocytes).
5. Cortisol attenuates fever mainly because it reduces the release of interleukin-1 from the white blood cells.
So it can be used in disease that are characterized by severe local inflammation like rheumatoid arthritis, rheumatic fever, and acute glomerulonephritis.
12-Effect on allergy:
It blocks the inflammatory response to allergic reactions in the same way that it blocks the other types of inflammatory response.13-Effect on blood:
It decreases the number of eosinophils and lymphocytes in the blood. It also increases the production of red blood cells (mechanisms unclear).
When excess cortisol is secreted by the adrenal glands, polycythemia often results, and conversely, when the adrenal glands secrete no cortisol, anemia often results.
Mineralocorticoids:
They are secreted by the adrenal cortex ,the most important is Aldosterone which increases the reabsorption of Na from the tubules of the kidney ,salivary ,sweat ,gastric and intestinal glands ,so it elevates the level of sodium in blood while K level is eliminated in the opposite direction.Mineralocorticoids:
Control of aldosterone secretion:
The release of aldosterone is under the influence of:
1-The level of K and Na in plasma:
the increased level of K and the reduction in Na level will cause stimulation of aldosterone secretion (direct effect on the adrenal gland).
2-Heamorhage and hypovolemia:
This result in decrease in venous return decrease in cardiac output→ pressure in afferent arterioles in the kidney is reduced →stimulation of juxtaglomerular apparatus in the kidney
→release of renin which acts on angiotensinogen, and convert it to angiotensin I .
During its passage to the capillaries of the lung converted to angiotensin II by converting enzyme secreted by the endothelial lining of the blood vessel of the lung.
Angiotensin II
1- increases the peripheral resistance and
2- it has direct stimulation to the adrenal cortex to release aldosteron→ Na retention and K elimination as a result we have increase in the blood pressure
Clinical conditions related to the adrenal gland disturbances:
1-Hyperadrenalism-Cushing’s SyndromeHypersecretion by the adrenal cortex (or prolonged exposure to high level of steroids) causes a complex cascade of hormone effects called Cushing’s syndrome.
The cause for this abnormality is either:
ACTH dependent causes :
Increase of ACTH →↑ cortisol level. As I case:
1-Tumor (like adenoma) of the anterior pituitary.
2-Abnormal function of the hypothalamus that causes high levels of corticotropin-releasing hormone (CRH),
3-“ectopic secretion” of ACTH by a tumor elsewhere in the body, such as an abdominal carcinoma;
When Cushing’s syndrome is secondary to excess secretion of ACTH by the anterior pituitary, this is referred to as Cushing’s disease.
2-Non- ACTH dependent causes:
1-Adrenocortical hyperplasia.
2-Adenoma of the adrenal cortex.( Primary overproduction of cortisol by the adrenal glands is usually associated with reduced ACTH levels due to cortisol feedback inhibition of ACTH secretion by the anterior pituitary gland).
3-Iatrogenic : administration of large amounts of synthetic glucocorticoid ,as in case of asthma, skin diseases and renal disorder.
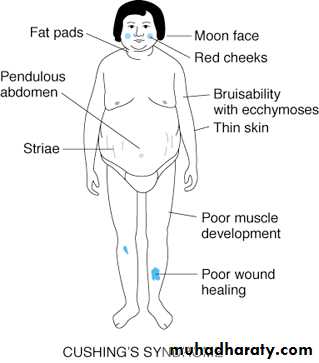
Symptoms of Cushing’s disease:
1-Effects on Carbohydrate Metabolism:Increased blood glucose concentration.
May cause diabetes mellitus.
2-The effects of glucocorticoids on protein:
Protein catabolism is often profound in Cushing’s syndrome, causing greatly decreased tissue proteins almost everywhere in the body. Severe muscles weakness and wasted thin limbs. Skin atrophy (bruises) and osteoporosis of the bones (back pain).


The loss of protein synthesis in the lymphoid tissues leads to a suppressed immune system, so that many of these patients die of infections. Also because of loss of protein in the subcutaneous tissues, they tear easily, resulting in development of large purplish striae in the skin.

3-The most striking feature of the disease:
Buffalohamp : mobilization of fat from the lower part of the body and abnormal deposition of fat in the lower part of the neck, the thoracic and upper abdominal regions.Moon face
Increase of Na and water retention.
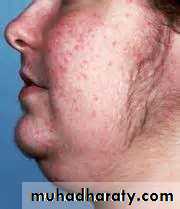
Excessive secretion of sex hormone acne, hirsutism (excess growth of hair on the face).
About 80 per cent of patients have hypertension, presumably because of the slight mineralocorticoid effects of cortisol.

Hypofunction of the adrenal cortex:
Hypoadrenalism-Addison’s Disease:Primary →tumor in the adrenal gland Addisson's disease.
Secondary→ reduction of the ACTH secretion due to pituitary or hypothalamic disorder.
The causes of Addisson's disease:
Autoimmune disease: antigene –antibody reaction.
Tuberculosis or invasion of the adrenal cortices by cancer →destruction of the gland. The symptoms partly due to aldosteron deficiency but mainly due to glucocorticoid deficiency.
Symptoms of Addisson's disease:
1-Mineralocorticoid Deficiency:
Sodium ions, chloride ions, and water are lost into urine in great amounts while K is preserved. The net result is a greatly decreased extracellular fluid volume which leads to hypotension. Cardiac output decreases, and the patient dies in shock if not treated.
2-Glucocorticoid Deficiency:
Hypoglycemia due to reduction of gluconeogenesis. It reduces the mobilization of both proteins and fats from the tissues, thereby depressing many other metabolic functions of the body.
Melanin Pigmentation: pigmentation of the mucous membranes and skin. Especially of the area that is already pigmented exposed to light e.g. face, neck, back of the neck, hand, elbow ,knee. Also mucus membrane like lips, eyelids and vagina.
The cause of pigmentation is as follows:
When cortisol secretion is depressed, the normal negative feedback to the hypothalamus and anterior pituitary gland is also depressed, therefore allowing tremendous rates of ACTH secretion as well as simultaneous secretion of increased amounts of MSH. Probably the tremendous amounts of ACTH cause most of the pigmenting effect because they can stimulate formation of melanin by the melanocytes in the same way that MSH does.13 24 39
↓ ↓This is like MSH ↑ All the activity of the ACTH is due to this limit
Addisonian Crisis. Great quantities of glucocorticoids are occasionally secreted in response to different types of physical or mental stress. In a person with Addison’s disease, at rest the patient is normal but the output of glucocorticoids does not increase during stress. Yet whenever different types of trauma, disease, or other stresses, such as surgical operations, a person is likely to have an acute need for excessive amounts of glucocorticoids and often must be given more than the normal quantities of glucocorticoids to prevent death.
This critical need for extra glucocorticoids and the associated severe debility in times of stress is called an addisonian crisis, in which GIT symptoms happen and acute abdominal pain, and hypotension . We have to correct it rapidly by dexamethazol injection.
The crises happens sometimes in cases like asthma we give the patients high doses of cortisol, so we have suppression of the activity of the adrenal gland, when stop giving the drug we have to stop it gradually not suddenly to avoid Addissonian crises.
Adrenal medulla:
This gland secretes adrenalin and noradrenalin (catecholamine), it is not under the control of pituitary gland or hypothalamus, but it is controlled by the autonomic nervous system so the hormones are called the hormones of emergency.
The quantity of adrenalin is about 4-5 times as much as that of noradrenalin The metabolic effect of catecholamine is mainly due to the effect of adrenalin rather than noradrenalin these effects include:
A-Increase the glucose level in the blood by:
1- stimulation of gluconeogenesis.
2-Inhibiting the release of insulin.
B-Increase the level of free fatty acids in blood so it is concerned as a ketogenic factor.
These effects of the hormones in various tissues are grouped according to the receptors with which they interact .We have 2 groups:
-Alpha receptors serve excitatory function as vasoconstriction.
-Beta receptors: serve predominantly inhibitory function as vasodilatation and bronchodiltation.
Except the effect on the heart → increase the force of concentration→ increase cardiac output→ increase systolic blood pressure→ increase pulse pressure.
Adrenalin causes tachycardia with an increase in cardiac output and a fall in the peripheral resistance, so we have increase in systolic blood pressure and a drop in the diastolic pressure, increase in pulse pressure.
Noradrenaline increase the total peripheral resistance while adrenalin causes vasoconstriction in splanchnic areas and dilatation of skeletal muscle blood vessels→ decrease in peripheral resistance→ decrease in blood pressure.
The clinical conditions result from disturbances of the release of catecholamins:
Pheochromocytoma a tumor of the adrenal medulla → increase secretion of catecholamins continuously or periodically (in young age mainly 20-25 years old). Increase in blood pressure →decrease diastolic pressure→ increase in pulse pressure.This case is associated with flushing, sweating (perspiration), palpitation or tachycardia, tremor of the hand and the patient may have headache.
Estimation of adrenalin and noradrenalin is done through the estimation of their metabolites in urine which is called venyl mandillic acid (VMA).