Lecture 1
Sunday 23/9/2012
Prof.Dr H.D.El-Yassin
2012
Introduction to the Biochemistry of Digestion,
Absorption and Detoxification
Digestion is the chemical breakdown of large food molecules into smaller
molecules that can be used by cells. The breakdown occurs when
certain specific enzymes are mixed with the food.
Main components of food are:
Carbohydrates
1.
Monosaccharides
or simple sugars are either hexoses (6-carbon)
like glucose, galactose and fructose, or pentoses (5-carbon) like
ribose. These are the breakdown products of more complex
carbohydrates and can be efficiently absorbed across the wall of
the digestive tube and transported into blood.
2.
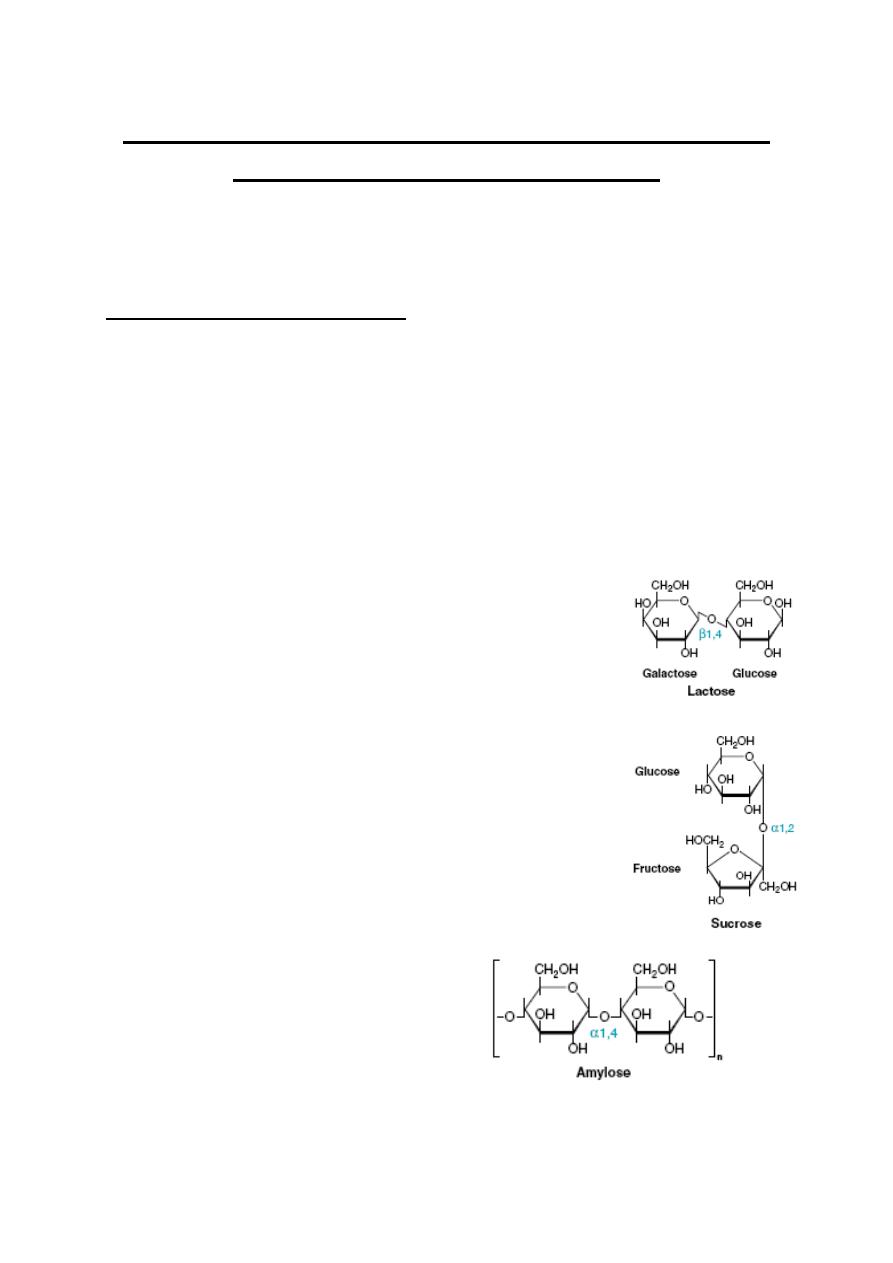
Disaccharides
are simply two monosaccharides linked together by
a glycosidic bond. The disaccharides most
important in nutrition and digestion are:
•
lactose or "milk sugar": glucose + galactose
•
sucrose or "table sugar": glucose + fructose
•
maltose: glucose + glucose
•
Oligosaccharides are relatively short chains of
monosaccharides which typically are
intermediates in the breakdown of
polysaccharides to monosaccharides.
3.
Polysaccharides
:
•
Starch is a major plant storage form of glucose.
It occurs in two forms:
•
alpha-amylose, in which the
glucoses are linked together
in straight chains,
Lecture 1
Sunday 23/9/2012
Prof.Dr H.D.El-Yassin
2012
•
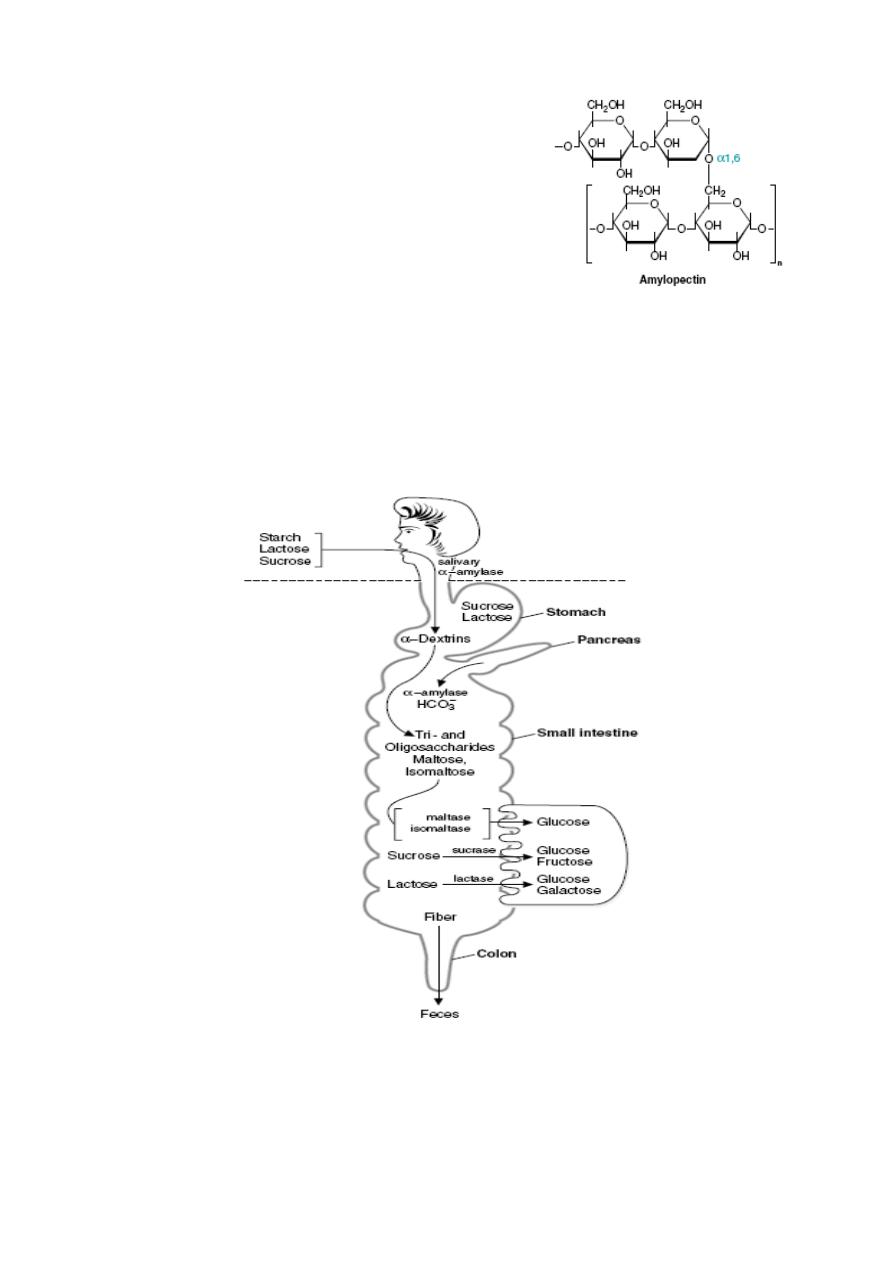
and amylopectin, in which the glucose
chains are highly branched. Except for
the branch points of amylopectin, the
glucose monomers in starch are linked
via alpha(1->4) glycosidic bonds,
which, in the digestive tract of
mammals, are hydrolyzed by
amylases.
•
Dietary fibers (Cellulose) is the other major plant carbohydrate. It
is the major constituent of plant cell walls, and more than half of the
organic carbon on earth is found in cellulose. Cellulose is
composed on unbranched, linear chains of D-glucose molecules,
linked to one another by beta(1->4) glycosidic bonds, which no
vertebrate has the capacity to enzymatically digest.
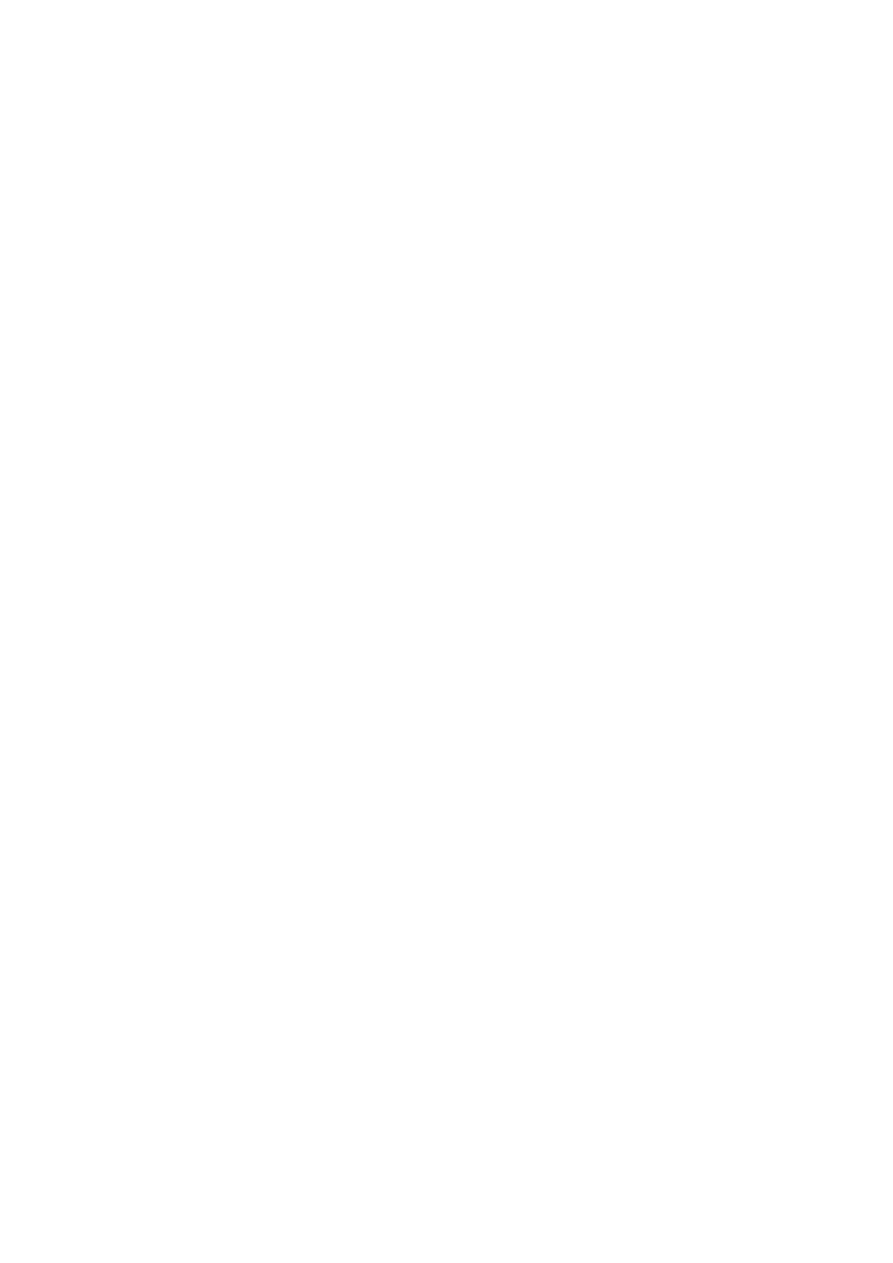
Overview of carbohydrate digestion. Digestion of the carbohydrates
occurs first, followed by absorption of monosaccharides. Subsequent
metabolic reactions occur after the sugars are absorbed.
Lecture 1
Sunday 23/9/2012
Prof.Dr H.D.El-Yassin
2012
Clinical cases in carbohydrate digestion and absorption:
1. Deria Voider is a 20-year-old exchange student from Nigeria who
has noted gastrointestinal bloating, abdominal cramps, and
intermittent diarrhea ever since arriving in the United States 6
months earlier. A careful history shows that these symptoms occur
most commonly about 45 minutes to 1 hour after eating breakfast
but may occur after other meals as well. Dairy products, not a part
of Deria’s diet in Nigeria, were identified as the probable offending
agent because her gastrointestinal symptoms disappeared when
milk and milk products were eliminated from her diet.
2. Ann Sulin’s fasting and postprandial blood glucose levels are
frequently above the normal range in spite of good compliance with
insulin therapy. Her physician has referred her to a dietician skilled
in training diabetic patients in the successful application of an
appropriate American Diabetes Association diet. As part of the
program, Ms. Sulin is asked to incorporate foods containing fiber
into her diet, such as whole grains (e.g., wheat, oats, corn),
legumes (e.g., peas, beans, lentils), tubers (e.g., potatoes,
peanuts), and fruits.
3. Nona Melos (no sweets) is a 7-month-old baby girl, the second
child born to unrelated parents. Her mother had a healthy, full-term
pregnancy, and Nona’s birth weight was normal. She did not
respond well to breastfeeding and was changed entirely to a
formula based on cow’s milk at 4 weeks. Between 7 and 12 weeks
of age, she was admitted to the hospital twice with a history of
screaming after feeding but was discharged after observation
without a specific diagnosis. Elimination of cow’s milk from her diet
did not relieve her symptoms; Nona’s mother reported that the
screaming bouts were worse after Nona drank juice and that Nona
frequently had gas and a distended abdomen. At 7 months she
was still thriving (weight above 97th percentile) with no abnormal
findings on physical examination. A stool sample was taken.

Lecture 1
Sunday 23/9/2012
Prof.Dr H.D.El-Yassin
2012
Proteins
Proteins are polymers of amino acids linked together by peptide bonds.
Chain length varies tremendously and many dietary proteins have been
modified after translation by addition of carbohydrate (glycoproteins) or
lipid (lipoprotein) moieties. Very short proteins, typically 3 to 10 amino
acids in length, are called peptides
Digestion of proteins. The proteolytic enzymes, pepsin, trypsin,
chymotrypsin, elastase, and the carboxypeptidases, are produced
as zymogens (the [pro] and [ogen] accompanying the enzyme name)
that are activated by cleavage after they enter the gastrointestinal lumen.

Lecture 1
Sunday 23/9/2012
Prof.Dr H.D.El-Yassin
2012
Clinical cases in protein digestion and absorption:
1. Sissy Fibrosa, a young child with cystic fibrosis, has had repeated
bouts of bronchitis caused by Pseudomonas aeruginosa. With
each of these infections, her response to aerosolized antibiotics
has been good. However, her malabsorption of food continues,
resulting in foul-smelling, glistening, bulky stools. Her growth
records show a slow decline. She is now in the 24th percentile for
height and the 20th percentile for weight. She is often listless and
irritable, and she tires easily. When her pediatrician discovered that
her levels of the serum proteins albumin, transferrin, and thyroid
hormone binding prealbumin (transthyretin) were low to low-normal
(indicating protein malnutrition), Sissy was given enteric-coated
microspheres of pancreatic enzymes. Almost immediately, the
character of Sissy’s stools became more normal and she began
gaining weight. In the next 6 months, her growth curves showed
improvement, and she seemed brighter, more active, and less
irritable.
2. For the first few months after a painful episode of renal colic, during
which he passed a kidney stone, Cal Kulis had faithfully
maintained a high daily fluid intake and had taken the medication
required to increase the pH of his urine. Because he has cystinuria,
these measures were necessary to increase the solubility of the
large amounts of cystine present in his urine and, thereby, to
prevent further formation of kidney stones (calculi). With time,
however, he became increasingly complacent about his preventive
program. After failing to take his medication for a month, he
experienced another severe episode of renal colic with grossly
bloody urine. Fortunately, he passed the stone spontaneously,
after which he vowed to faithfully comply with therapy. His mother
heard that some dietary amino acids were not absorbed in patients
with cystinuria and asked whether any dietary changes would
reduce Cal’s chances of developing additional renal stones.
Lecture 1
Sunday 23/9/2012
Prof.Dr H.D.El-Yassin
2012
Lipids
Fatty acids are present in only small amounts in animal and plant
tissues, but are the building blocks of many important complex lipids.
True fatty acids possess a long hydrocarbon chain terminating in a
carboxyl group. Nearly all fatty acids have an even number of carbons
and have chains between 14 and 22 carbons in length. The principle
differences among the many fatty acids are the length of the chain
(usually 16 or 18 carbons) and the positions of unsaturated or double
bonds.
The most abundant storage form of fat in animals and plants, and hence
the most important dietary lipid, is triglyceride. A molecule of triglyceride
is composed of a molecule of glycerol in which each of the three carbons
is linked through an ester bond to a fatty acid. Triglycerides cannot be
efficiently absorbed, and are enzymatically digested by pancreatic lipase
into a 2-monoglyceride and two free fatty acids, all of which can be
absorbed. Other lipases hydrolyse a triglyceride into glycerol and three
fatty acids.
fatty acids and glycerol

Lecture 1
Sunday 23/9/2012
Prof.Dr H.D.El-Yassin
2012
Clinical cases in lipid digestion and absorption:
1. Will Michael had several episodes of mild back and lower
extremity pain over the last year, probably caused by minor sickle
cell crises. He then developed severe right upper abdominal pain
radiating to his lower right chest and his right flank 36 hours before
admission to the emergency room. He states that the pain is not
like his usual crisis pain. Intractable vomiting began 12 hours after
the onset of these new symptoms. He reports that his urine is the
color of iced tea and his stool now has a light clay color. On
physical examination, his body temperature is slightly elevated,
and his heart rate is rapid. The whites of his eyes (the sclerae) are
obviously jaundiced (a yellow discoloration caused by the
accumulation of bilirubin pigment). He is exquisitely tender to
pressure over his right upper abdomen. The emergency room
physician suspects that Michael is not in sickle cell crisis but
instead has either acute cholecystitis (gallbladder inflammation) or
a gallstone lodged in his common bile duct, causing cholestasis
(the inability of the bile from the liver to reach his small intestine).
His hemoglobin level was low at 7.6 mg/dL (reference range _12–
16) but unchanged from his baseline 3 months earlier. His serum
total bilirubin level was 3.2 mg/dL (reference range _ 0.2–1.0), and
his direct (conjugated) bilirubin level was 0.9 mg/dL (reference
range _0 –0.2). Intravenous fluids were started, he was not allowed
to take anything by mouth, a nasogastric tube was passed and
placed on constant suction, and symptomatic therapy was started
for pain and nausea. When his condition had stabilized, Michael
was sent for an ultrasonographic (ultrasound) study of his upper
abdomen.
2.
Al Martini has continued to abuse alcohol and to eat poorly. After
a particularly heavy intake of vodka, a steady severe pain began in
his upper mid-abdomen. This pain spread to the left upper
quadrant and eventually radiated to his mid-back. He began
vomiting nonbloody material and was brought to the hospital
emergency room with fever, a rapid heart beat, and a mild
reduction in blood pressure. On physical examination, he was
dehydrated and tender to pressure over the upper abdomen. His
vomitus and stool were both negative for occult blood. Blood
samples were sent to the laboratory for a variety of hematologic
and chemical tests, including a measurement of serum amylase
and lipase, digestive enzymes normally secreted from the exocrine
pancreas through the pancreatic ducts into the lumen of the small
intestine.
Lecture 1
Sunday 23/9/2012
Prof.Dr H.D.El-Yassin
2012
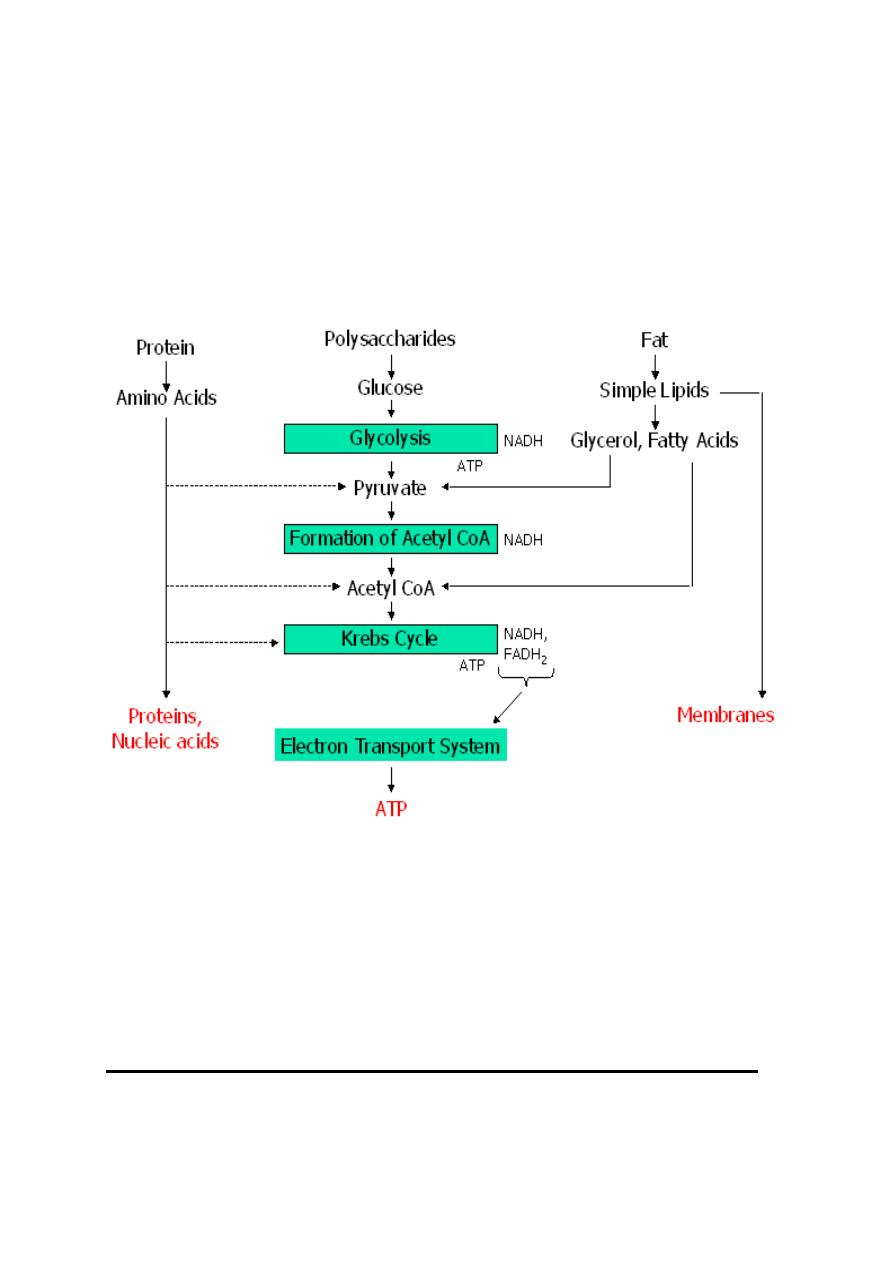
The process of digestion produces glucose, amino acids, glycerol, and
fatty acids (see above). The energy in glucose is used to produce ATP
via the reactions of glycolysis, cellular respiration, and the electron
transport system (see diagram below). The body uses amino acids to
construct proteins. Excess amino acids can be used to synthesize
pyruvate, acetyl CoA, and alpha ketogluterate, which enters the Krebs
cycle. Glycerol and fatty acids can be converted to pyruvate and Acetyl
CoA and then enter cellular respiration.
Digestion and absorption in the GI tract
Lecture 1
Sunday 23/9/2012
Prof.Dr H.D.El-Yassin
2012
Mouth
Chewing breaks food into smaller particles so that chemical digestion
can occur faster.
• Enzymes: Salivary amylase breaks starch (a polysaccharide)
down to maltose (a disaccharide).
• Bicarbonate ions in saliva act as buffers, maintaining a pH between
6.5 and 7.5.
• Mucins (mucous) lubricate and help hold chewed food together in a
clump called a bolus.
Stomach
The stomach stores up to 2 liters of food. Gastric glands within the
stomach produce secretions called gastric juice.
The muscular walls of the stomach contract vigorously to mix food with
gastric juice, producing a mixture called chyme.
Gastric juice
• Pepsinogen is converted to pepsin, which digests proteins.
Pepsinogen production is stimulated by the presence of gastrin in
the blood.
• HCl
Hydrochloric acid (HCl) converts pepsinogen to pepsin which breaks
down proteins to peptides. HCl maintains a pH in the stomach of
approximately 2.0.
It also dissolves food and kills microorganisms.
Mucous protects the stomach from HCl and pepsin.
Secretion of Gastric Juice: Gastrin is a hormone that stimulates the
stomach to secrete gastric juice.
Duodenum
The duodenum is the first part of the small intestine.
Chyme enters in tiny spurts. At this point, proteins and carbohydrates are
only partially digested and lipid digestion has not begun.
Lecture 1
Sunday 23/9/2012
Prof.Dr H.D.El-Yassin
2012
Pancreas
The pancreas acts as an exocrine gland by producing pancreatic juice
which empties into the small intestine via a duct.
The pancreas also acts as an endocrine gland to produce insulin.
• Pancreatic Juice
Pancreatic juice contains sodium bicarbonate which neutralizes the
acidic material from the stomach.
• Pancreatic amylase digests starch to maltose.
• Trypsin and Chymotrypsin digest proteins to peptides. Like
pepsin (produced in the stomach), they are specific for certain
amino acids, not all of them. They therefore produce peptides.
• Lipase digests fats to glycerol and fatty acids.
Liver
The liver produces bile which is stored in gallbladder and sent to the
duodenum through a duct.
Bile emulsifies fats (separates it into small droplets) so they can mix with
water and be acted upon by enzymes.
Other Functions of the Liver
• The liver detoxifies blood from intestines that it receives via the
hepatic portal vein.
• The liver stores glucose as glycogen (animal starch) and breaks
down glycogen to release glucose as needed. This storage-release
process maintains a constant glucose concentration in the blood
(0.1%). If glycogen and glucose run short, proteins can be
converted to glucose.
• It produces blood proteins.
• It destroys old red blood cells and converts hemoglobin from these
cells to bilirubin and biliverdin which are components of bile.
• Ammonia produced by the digestion of proteins is converted to a
less toxic compound (urea) by the liver.
Hormones Involved in Digestion

Lecture 1
Sunday 23/9/2012
Prof.Dr H.D.El-Yassin
2012
1. Gastrin: The presence of food in the stomach stimulates specific
receptors which in turn stimulates endocrine cells in the stomach to
secrete the hormone gastrin into the circulatory system. Gastrin
stimulates the stomach to secrete gastric juice.
2. Secretin: Secretin is produced by cells of the duodenum.
It’s production is
stimulated by acid
chyme from
stomach.
It stimulates the
pancreas to produce sodium bicarbonate, which neutralizes the acidic
chyme. It also stimulates the liver to secrete bile.
3. CCK (cholecystokinin): CCK production is stimulated by the
presence of food in the duodenum. It stimulates the gallbladder to
release bile and the pancreas to produce pancreatic enzymes.
4. GIP (Gastric Inhibitory Peptide):Food in the duodenum
stimulates certain endocrine cells to produce GIP.
It has the opposite effects of gastrin; it inhibits gastric glands in the
stomach and it inhibits the mixing and churning movement of stomach
muscles. This slows the rate of stomach emptying when the duodenum
contains food.
Small Intestine
The small intestine is approximately 3 m long. Like the stomach, it
contains numerous ridges and furrows. In addition, there are numerous
projections called villi that function to increase the surface area of the
intestine. Individual villus cells have microvilli which greatly increase
absorptive surface area.
The total absorptive surface area is equivalent to 500 or 600 square
meters.
Each villus contains blood vessels and a lacteal (lymph vessel).
Peptidases and maltase are embedded within the plasma membrane of
the microvilli.
Peptidases complete the digestion of peptides to amino acids.
Maltase completes the digestion of disaccharides.
Absorption:
Lecture 1
Sunday 23/9/2012
Prof.Dr H.D.El-Yassin
2012
The Large Intestine:
It functions in three processes:
•
Recovery of water and electrolytes from ingesta
: By the time
ingesta reaches the terminal ileum, roughly 90% of its water has
been absorbed, but considerable water and electrolytes like
sodium and chloride remain and must be recovered by absorption
in the large gut.
•
Formation and storage of feces
: As ingesta is moved through the
large intestine, it is dehydrated, mixed with bacteria and mucus,
and formed into feces.
•
Microbial fermentation
: The large intestine of all species teems with
microbial life. Those microbes produce enzymes capable of
digesting many of molecules that to vertebrates are indigestible,
cellulose being a premier example.
Absorption:
water, sodium ions
and chloride ions
•
Secretion:
bicarbonate ions and mucus
Summary of Digestive Enzymes
The digestive enzymes in the table below are summarized
according to type of food that they digest.
Lecture 1
Sunday 23/9/2012
Prof.Dr H.D.El-Yassin
2012
FOOD TYPE
ENZYME
SOURCE
PRODUCTS
CARBOHYDRATES Salivary amylase
Pancreatic
amylase
Maltase
Salivary
glands
Pancreas
Small intestine
Maltose
Maltose
Glucose
PROTEINS
Pepsin
Trypsin
Peptidases
Stomach
mucosa
Pancreas
Intestinal
mucosa
Peptides
Peptides
Amino acids
FATS
Lipase
Pancreas
Fatty acids
and glycerol
The table below shows digestive enzymes grouped by source of the
enzyme.
SOURCE
ENZYME
FOOD
PRODUCT
MOUTH (salivary
glands)
Salivary
amylase
Polysaccharides Maltose
STOMACH
Pepsin
Proteins
Peptides
PANCREAS
Pancreatic
amylase
Trypsin
Lipase
Polysaccharides
Proteins
Fats
Maltose
Peptides
Fatty acids
and
glycerol
SMALL INTESTINE
Maltase
Peptidases
Maltose
Peptides
Glucose
Amino
acids